
#IDSA AMR Updates 2023
#IDtwitter
#Medtwitter
Updates in ESBL E
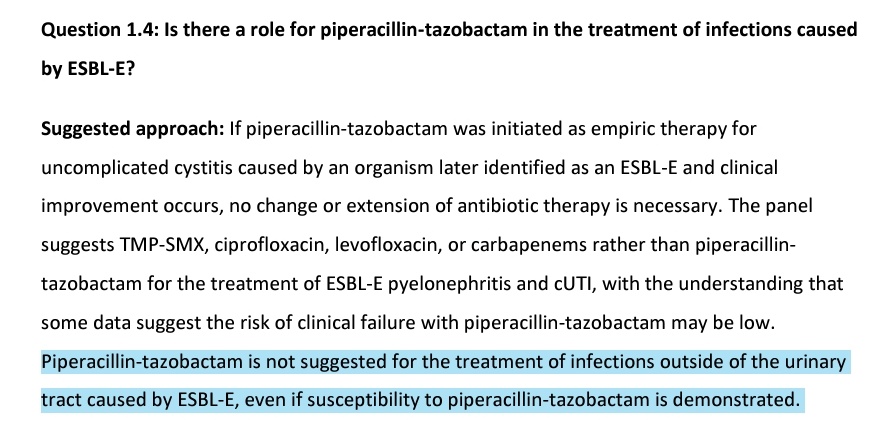
To avoid piptaz in non UTI
To avoid Cefepime
No role of Cephamycins
No role of Ceftalazone - Tazobactam
@CidsIndia
@idcon2022 @id_cure
@IDstewardship
#IDtwitter
#Medtwitter
Updates in ESBL E
To avoid piptaz in non UTI
To avoid Cefepime
No role of Cephamycins
No role of Ceftalazone - Tazobactam
@CidsIndia
@idcon2022 @id_cure
@IDstewardship



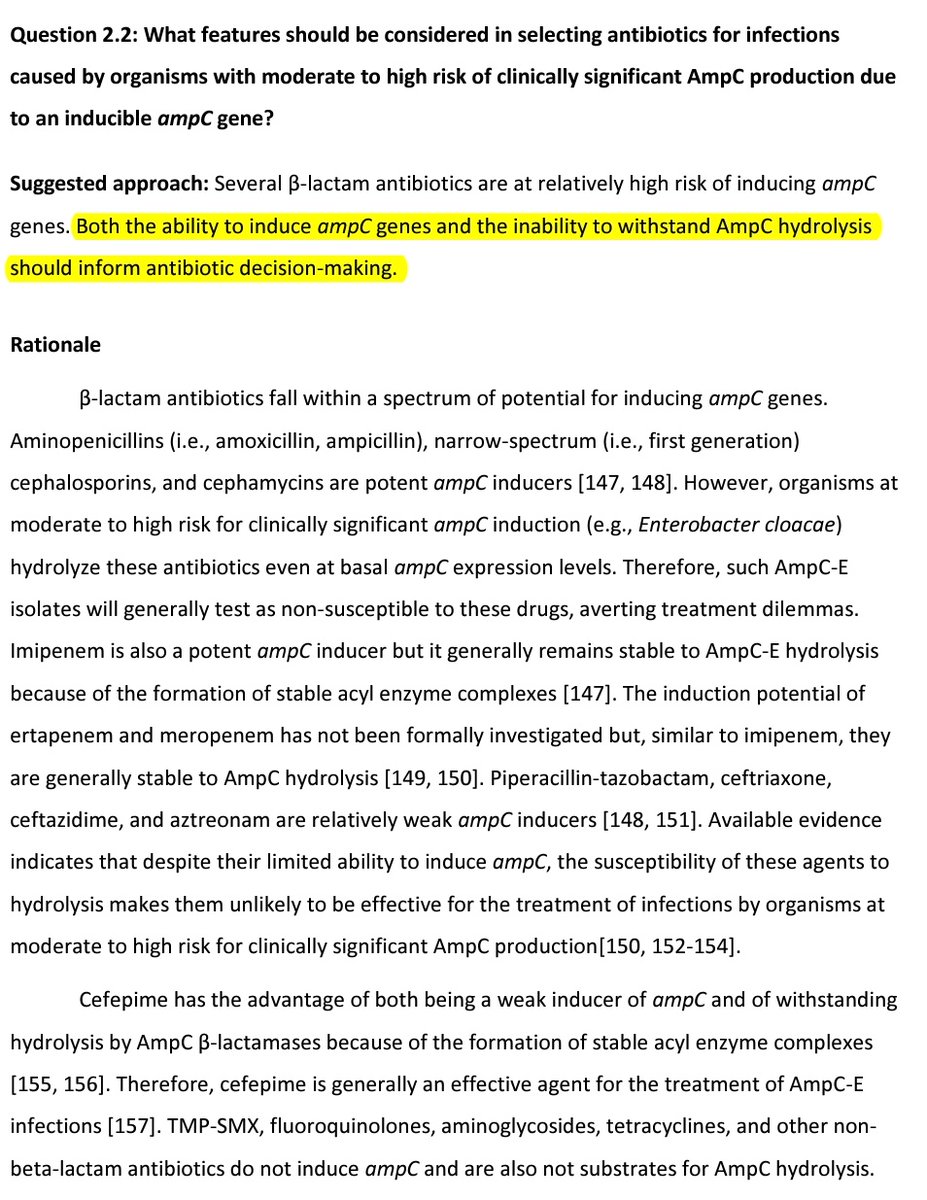
Updates in AmpC
Explained well about How to choose Antibiotics in AmpC -
Explained well about How to choose Antibiotics in AmpC -


Updates in CRE -
Explicitly mentions TOC for NDM, OXA, KPC & while awaiting reports.
No role of Tetracycline derivatives in UTI/ BSI
Explicitly mentions TOC for NDM, OXA, KPC & while awaiting reports.
No role of Tetracycline derivatives in UTI/ BSI




Updates in Pseudo
TOC for MDR Pseudo
TOC for MBL - No added benefit of Ceftazidime -avibactam+Aztreonam vs Aztreonam alone
Combination therapy in DTR Pseudo-Don't use Polymxin+Aminoglycosides -use Newer BL-BLI+Tobramycin if tobra is S, if R use Newer BL-BLI+ Polymyxin
TOC for MDR Pseudo
TOC for MBL - No added benefit of Ceftazidime -avibactam+Aztreonam vs Aztreonam alone
Combination therapy in DTR Pseudo-Don't use Polymxin+Aminoglycosides -use Newer BL-BLI+Tobramycin if tobra is S, if R use Newer BL-BLI+ Polymyxin


Updates in CRAB
CRAB therapy -Sulbactam + Mino>Tige , or Sulbactam + Polymyxin B, Mero + Poly B not to be used
If using Ampicillin - Sulbactam - panel suggest *against* the use of Meropenem in the combination
CRAB therapy -Sulbactam + Mino>Tige , or Sulbactam + Polymyxin B, Mero + Poly B not to be used
If using Ampicillin - Sulbactam - panel suggest *against* the use of Meropenem in the combination


Stenotrophomonas updates
Combination only - no role of single agent
Ceftazidime -avibactam + Aztreonam if clinical instability, intolerance
Combination only - no role of single agent
Ceftazidime -avibactam + Aztreonam if clinical instability, intolerance

• • •
Missing some Tweet in this thread? You can try to
force a refresh



