I think we should protect people worldwide from severe disease first, but since that wasn’t ACIP’s reason, this insistence seems confusing. Don’t we vaccinate against varicella & flu, even if mild?
2/4
Aug 18, 2021 • 5 tweets • 1 min read
This "simple rule" = locking in the inequity of initial vaccine distribution.
Boosters should be based on risk of severe outcomes if infected after vaccination, not based on how many months ago you were vaccinated--especially given that they admit 8 months is guesswork.
Based on this approach, we are going to put dedicated Jan 2020 vaccine-hunters & a bunch of random hospital employees who were conveniently near our early distribution sites before higher-risk populations who had to overcome hesitancy, access barriers, & unfair eligibility rules
Aug 17, 2021 • 4 tweets • 1 min read
I’ve been critical of booster moratoria as overbroad. There are people at documented high risk here who may benefit greatly from a 3rd dose.
But this throw-the-door-open approach willfully ignores tradeoffs & global scarcity, & rests on scant evidence. apnews.com/article/health…
And the idea we need to give Pfizer recipients 3x Pfizer confuses following the manufacturer with following the science.
If we’re going to do this, at least use fractional-dosing or mix&match boosters so we can use supply to save more lives. Not 150M mRNA vaccines for tiny gains
Aug 16, 2021 • 5 tweets • 2 min read
Below I discuss why we should avoid wasting vaccine doses & redirect them where they can be used—including abroad.
But another interviewee's comments exemplify a systematic pandemic ethics error: seeking to avoid blame & ignoring background risk
npr.org/sections/goats…
1/5
Dr. Plescia @ASTHO says "particularly if it's been distributed to local communities, pulling it all back is kind of asking for some error or problem.”
Are errors possible? Could something go wrong? Yes
But what’s worse—risk of error, or risk of delayed/no vaccine access?
2/5
Jul 30, 2021 • 5 tweets • 2 min read
This is the most compelling slide in the set, and makes a very good case for universal masking right now, which I agree with.
However, I'd have liked to see CDC grapple with this: what's the overall reduction in R if vaccinated people mask, but unvaccinated people don't?
My other concern about some framing (in reporting/Twitter, not the slides) is that it may fuel the following misinterpretation: "a vaccinated/vaccinated person encounter is as likely to transmit Covid as an unvaccinated/unvaccinated one"
That isn't what the slides/data say!
2/5
Jul 30, 2021 • 6 tweets • 2 min read
This is valuable reporting but there's a lot in here that's confusing. Would the Post or the CDC consider just publishing the slide deck?
1/ washingtonpost.com/health/2021/07…
"there is a higher risk among older age groups for hospitalization and death relative to younger people, regardless of vaccination status"
- but surely what should matter is whether vaccination reduces absolute risk for one or both groups, not risk relative to one another?
2/
Jul 29, 2021 • 5 tweets • 1 min read
The plurality answer in my (unscientific!) poll was the CDC's rec: require masks for everyone everywhere, but allow any type
A less popular answer--don't require masks everywhere (esp. for vaccinated people), but sometimes require KN95+ masks--may better balance benefit/burden.
But current guidance allows high risk (unvaxed hospital visitors w/1-layer cloth masks) & imposes burden w/o large benefit (masking in distanced/ventilated indoor spaces w/everyone vaccinated)
Also hard to square w/open indoor dining
Jul 7, 2021 • 6 tweets • 2 min read
Very detailed and helpful paper. Upshot:
- found a small (non-significant) *decrease* in full vax rates in Ohio post lottery
- found a small (non-significant) increase over all lottery states
Agree: "unlikely there are hugely positive or hugely negative effects"
As a non-expert, I like the preregistration & use of synthetic control. Some remaining questions
- is theirs the right counterfactual? (see thread)
- is the proper outcome to measure full vax, as they did, or 1 dose (I'd actually think 1 dose is the more lottery-relevant outcome)
Apr 22, 2021 • 4 tweets • 1 min read
"77% of white adults who want a shot have gotten one, compared with 60% of Black adults and 55% of Hispanics who want one."
Not everyone who WANTS a vaccine has been able to get one. "The survey suggests that vaccine access is at least as big of a problem as vaccine hesitancy."
"The racial gap persists across income levels, but is widest among people making less than $50,000 annually: 72 percent of white adults in that group who want a shot have gotten one, compared with 57 percent of Black adults and 47 percent of Hispanic adults in that income range."
COVID-19 remains a pandemic that causes serious, widespread, not fully understood harms
Universally stopping an efficacious COVID-19 vaccine should only be done after seriously weighing the harms of stopped access against side effects of the vaccine
Not just MDs but:
- health econ (@healthecon_dan)
- behavioral health (@abuttenheim)
- literally wrote the book on "nonmaleficence" (Jim Childress)
- tribal health (@echohawkd3)
et al
2/6
Apr 13, 2021 • 4 tweets • 2 min read
I agree that a pause isn't permanent & the FDA should track safety concerns
But forced "pausing" (AKA cancelling people's J&J appointments) isn't the right move
People should be given the info & allowed to choose
Deaths from Covid b/c you weren't vaccinated are permanent
We have enough supply that we could send MI more vaccines. Only Jeff Zients’ bizarre burden-insensitive conception of “fairness” prevents this
Or we could let MI extend dosing intervals by 2 weeks to get first doses to more people
Dec 20, 2020 • 6 tweets • 3 min read
For those following #ACIP vaccine prioritization debate - proposal to have 75+ alongside frontline workers in phase 1B is interesting, and different from prior discussion. But there are still pitfalls with any age cutoff, whether 75 or 65, as I explained in a comment to ACIP /1
Down Syndrome deaths are disparately high and happen before 75. 54%, 61%, and 69% of Black, Hispanic, and AI/AN deaths (respectively) happen before 75. I haven't seen US data on income x age at death, but a similar gradient is plausible, and may help explain the race data. /2
Dec 20, 2020 • 7 tweets • 4 min read
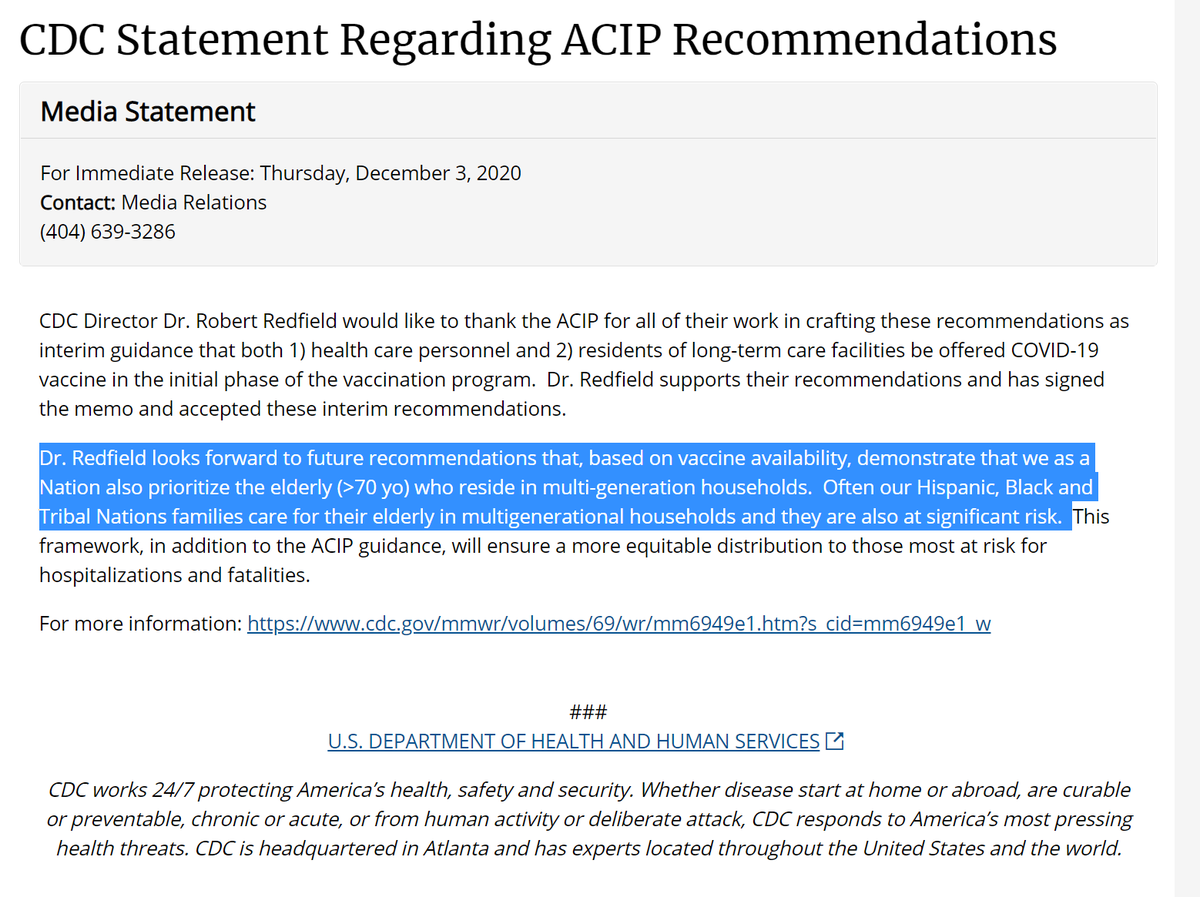
Last (grumpy) thread about #ACIP vax prioritization before bed. Sure, there are some hard tradeoffs, though looking for overlapping risk should make it easier, & ACIP could have had better framing. But critics have been a real mess. Exhibit A, dishonest quoting (aka lying): 1/6
Redfield: need to"demonstrate that we as a Nation also prioritize the elderly (>70 yo) who reside in multi-generation households. Often our Hispanic, Black and Tribal Nations families care for their elderly in multigenerational households and they are also at significant risk."2/
Dec 19, 2020 • 9 tweets • 6 min read
Thread on interconnected #bioethics problems in #COVID19 vaccine allocation: (1) the Stanford med center allocation debacle, (2) Rupert Murdoch, and (3) high-profile calls for age-only (“oldest first”) allocation policies. If you like (3), unfortunately you get (1) and (2). 1/7
People are right to be upset w/Stanford: see @CarolineYLChen excellent piece
. But it’s not “algorithms”, it’s inputs. If your inputs are too simplistic (age-only, ignore exposure or medical risk), you get bad outcomes, e.g. no residents, senior WFH 1st 2/7
Apr 16, 2020 • 9 tweets • 4 min read
This op-ed by Harald Schmidt @PennMEHP is a hugely valuable contribution to the #bioethics debate over ventilator allocation, & would have applications to other scarce resources as well. Some thoughts /1
Modifying SOFA score w/"weights" based on race would be struck down in federal court (& certainly by this SCOTUS) under #ParentsInvolved precedent scholar.google.com/scholar_case?c…. Not endorsing that precedent, but crucial to recognize it. Area Deprivation Index is better approach /2
Mar 12, 2020 • 11 tweets • 4 min read
Glad to be able to contribute to growing discussion on a timely and crucial topic--fair health care allocation in the Covid-19 pandemic--alongside Zeke Emanuel & @DrPhillipsMD: nytimes.com/2020/03/12/opi…. A quick summary of our recommendations (mini thread)
1.The group getting first priority should be health care workers and other first responders.