1/14
What is the mechanism of night sweats?
We ask about "fevers, chills, and NIGHT sweats", not "fevers, chills, and DAY sweats." Why?
To understand the answer, we'll need to cover temperature regulation, circadian rhythms, and more...
What is the mechanism of night sweats?
We ask about "fevers, chills, and NIGHT sweats", not "fevers, chills, and DAY sweats." Why?
To understand the answer, we'll need to cover temperature regulation, circadian rhythms, and more...
2/
Let’s start with a more basic question. What happens to core body temperature (Tc) as a result of sweating?
Let’s start with a more basic question. What happens to core body temperature (Tc) as a result of sweating?
3/
To understand the answer (Tc decreases), recall that the preoptic anterior hypothalamic region ensures that core body temperature (Tc) is kept within the narrow range that allows for organ function.
ncbi.nlm.nih.gov/pubmed/17875917
To understand the answer (Tc decreases), recall that the preoptic anterior hypothalamic region ensures that core body temperature (Tc) is kept within the narrow range that allows for organ function.
ncbi.nlm.nih.gov/pubmed/17875917

4/
Regulators of Tc (thermoeffectors) include shivering and sweating.
The range between the Tc prompting shivering (or vasoconstriction in some reports) and the Tc prompting sweating is the core interthreshold zone (CIZ).
ncbi.nlm.nih.gov/pubmed/16410380
Regulators of Tc (thermoeffectors) include shivering and sweating.
The range between the Tc prompting shivering (or vasoconstriction in some reports) and the Tc prompting sweating is the core interthreshold zone (CIZ).
ncbi.nlm.nih.gov/pubmed/16410380

5/
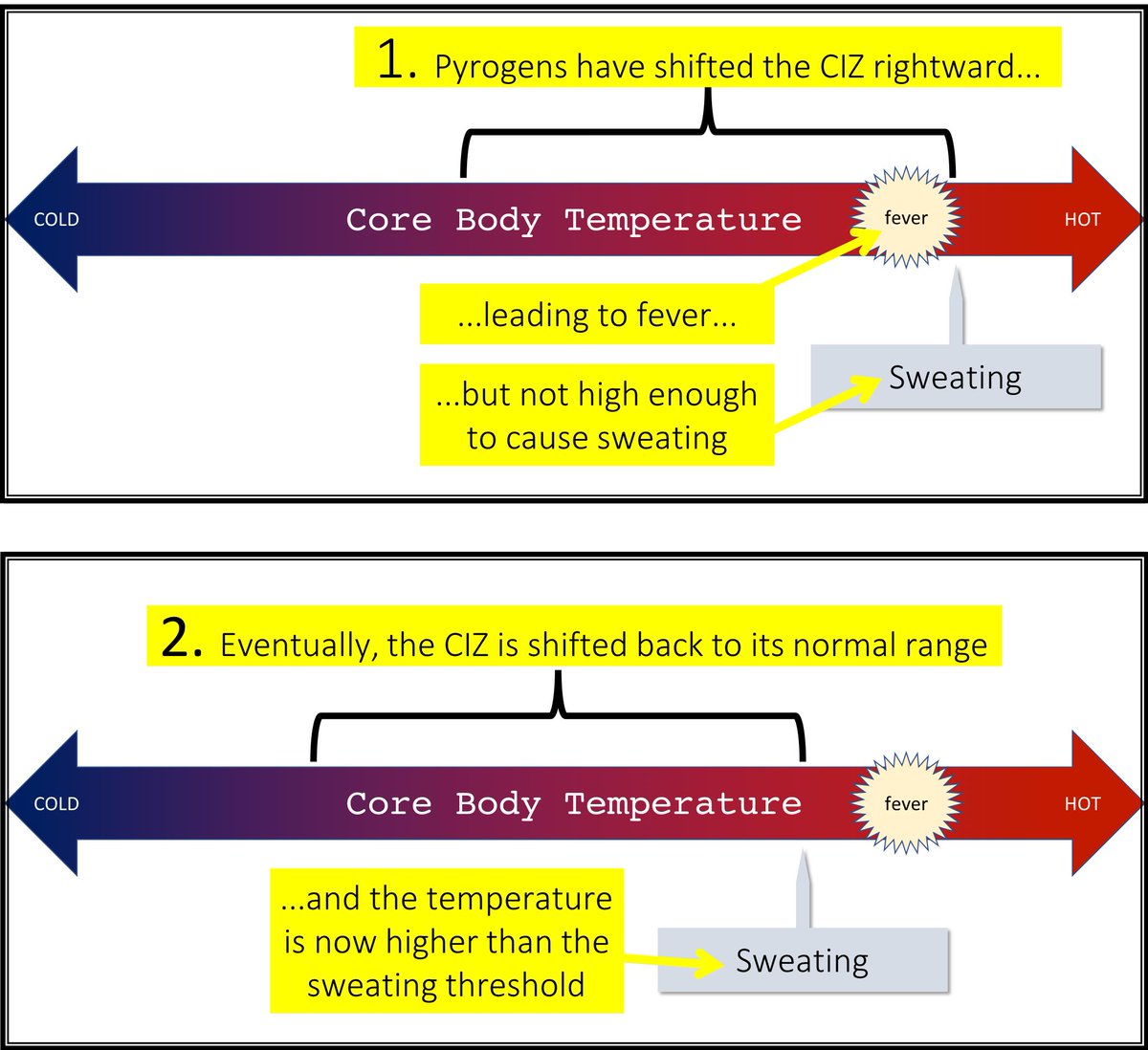
When cytokines released during inflammation (e.g., IL-1) lead to an increase in the hypothalamic set-point, shivering occurs at a temperature that would not have otherwise done so.
This helps to raise Tc, leading to fever.
ncbi.nlm.nih.gov/pubmed/30454596
When cytokines released during inflammation (e.g., IL-1) lead to an increase in the hypothalamic set-point, shivering occurs at a temperature that would not have otherwise done so.
This helps to raise Tc, leading to fever.
ncbi.nlm.nih.gov/pubmed/30454596
6/
Eventually, the hypothalamus returns the set-point to the prior (lower) range.
To lower the Tc, sweating and vasodilation occur. The fever has "broken".
Eventually, the hypothalamus returns the set-point to the prior (lower) range.
To lower the Tc, sweating and vasodilation occur. The fever has "broken".
7/
Let's move onto sleep. What happens to core body temperature during sleep?
Let's move onto sleep. What happens to core body temperature during sleep?
8/
In 1941, Richard Day showed that core temperature drops with sleep onset.
This decrease likely resulted, in part, from sweating (presumed to have occurred based on concurrent weight loss with sleep onset).
dx.doi.org/10.1001/archpe…
In 1941, Richard Day showed that core temperature drops with sleep onset.
This decrease likely resulted, in part, from sweating (presumed to have occurred based on concurrent weight loss with sleep onset).
dx.doi.org/10.1001/archpe…

9/
The reason we sweat overnight (thereby lowering Tc) is that the threshold for sweating is lowered. This means that we sweat at temperatures lower than what would prompt in the afternoon or evening.
ncbi.nlm.nih.gov/pubmed/9426297
The reason we sweat overnight (thereby lowering Tc) is that the threshold for sweating is lowered. This means that we sweat at temperatures lower than what would prompt in the afternoon or evening.
ncbi.nlm.nih.gov/pubmed/9426297

10/ INTERIM SUMMARY
•Core body temperature is kept within a narrow range with sweating/shivering acting as thermoreffectors engaged to help thermoregulate.
•At night, the threshold to sweat is lowered, leading to heat dissipation and a nadir core temperature.
•Core body temperature is kept within a narrow range with sweating/shivering acting as thermoreffectors engaged to help thermoregulate.
•At night, the threshold to sweat is lowered, leading to heat dissipation and a nadir core temperature.
11/
What about the increased frequency of night sweats seen in conditions like tuberculosis?
My hypothesis: If patients experience nocturnal release of pyrogens, a "fever" that wouldn't result in sweating at 3pm (because it remains within the CIZ) may result in sweating at 3am.
What about the increased frequency of night sweats seen in conditions like tuberculosis?
My hypothesis: If patients experience nocturnal release of pyrogens, a "fever" that wouldn't result in sweating at 3pm (because it remains within the CIZ) may result in sweating at 3am.
12/
One study of patients with Hodgkin's disease showed that their night sweats were preceded by bumps in Tc.
These bumps may occur more often in conditions associated with night sweats. And, they're just enough to cause sweating given the shifted CIZ.
ncbi.nlm.nih.gov/pubmed/2372772
One study of patients with Hodgkin's disease showed that their night sweats were preceded by bumps in Tc.
These bumps may occur more often in conditions associated with night sweats. And, they're just enough to cause sweating given the shifted CIZ.
ncbi.nlm.nih.gov/pubmed/2372772

13/
Before summarizing, a modified post-tweetorial question.
⭐️How would you explain the cause of night sweats to someone else?⭐️
Reply to this tweet with your answer. I'll reply back to all the answers I get!
Before summarizing, a modified post-tweetorial question.
⭐️How would you explain the cause of night sweats to someone else?⭐️
Reply to this tweet with your answer. I'll reply back to all the answers I get!
14/SUMMARY
What causes night sweats?
•At night, the threshold to sweat is lowered making everyone more likely to sweat while sleeping
•In conditions likely to cause intermittent increases in temperature, this lowered threshold to sweat is more likely to be reached
What causes night sweats?
•At night, the threshold to sweat is lowered making everyone more likely to sweat while sleeping
•In conditions likely to cause intermittent increases in temperature, this lowered threshold to sweat is more likely to be reached
• • •
Missing some Tweet in this thread? You can try to
force a refresh