
This afternoon's #CBD will be moderated by Mr @AlexAlamri, neurosurgery trainee and co-founder @realbrainbook
A quick reminder of the rules before we begin... and let's get started! #BBGBM (plus your best excitement gifs on here please)
A quick reminder of the rules before we begin... and let's get started! #BBGBM (plus your best excitement gifs on here please)

1. A 63 year old female presents to clinic with several months history of intermittent neck pain. She reports weakness and clumsiness in both her hands. She further reports episodes of unsteadiness on her feet which has led to several falls over the past couple of months #bbcm
2. Based on the history, what are your thoughts on a differential diagnosis? #bbcm
3. Degenerative: herniated cervical disc, cervical spondylotic myelopathy, Neoplastic: spinal cord tumour, pathological fracture, Infectious: epidural abscess, Other: MS, ALS, osteoporosis, rheumatoid arthritis. #bbcm
4. Now that you have a few differentials in mind, you go on to obtain a further history. What questions would you like to ask?
#bbcm
#bbcm
5. SOCRATES for her neck pain/weakness, comprehensive neurological history, B symptoms: (fever, night sweats, weight loss) bladder/ bowl symptoms, past medical/ surgical history, drug history, family history, social history (impact on life is important/ADLs). #bbcm
6. The patient reports the neck pain has got progressively worse over the past 6 months. Intermittent and worse on movement in all directions. It often radiates over her shoulders and down her arms. It’s not relieved by OTC analgesia. She scores the pain as 7/10. #bbcm
7. She also reports tingling in the bilateral upper extremities. She reports loss of fine motor control of the hands and fingers (bilaterally) affecting her eating, writing and fastening buttons. As such, she’s finding it difficult to carry out her activities of daily life. #bbcm
8. She says her gait is also increasingly unsteady and she won't leave the house for fear of falling. She’s had no fever nor weight loss and has no bladder nor bowl symptoms. She has a PMH of hypertension and arthritis which are controlled with amlodipine and paracetamol. #bbcm
9. Based on this information, what do you think is now the most likely diagnosis? #bbcm
10. Cervical myelopathy is our most likely diagnosis based on the above signs & symptoms. #bbcm
11. Are there any examinations you’d like to perform at this stage? (You're all doing really well so keep it up 🔥) #bbcm
12. Comprehensive upper/lower limb neurological exam (tone, power, co-ordination, sensation, proprioception, reflexes), gait and balance exam (heel to toe, Romberg’s test), spinal exam (check range of movement, facet tenderness). Fantastic suggestions everyone! #bbcm
13. When examining for neurological deficits it’s important to understand the myotomes, dermatomes and reflexes that we are testing. By systematically examining these, we can determine the cord segments that have been injured. Let's go through them now #bbcm
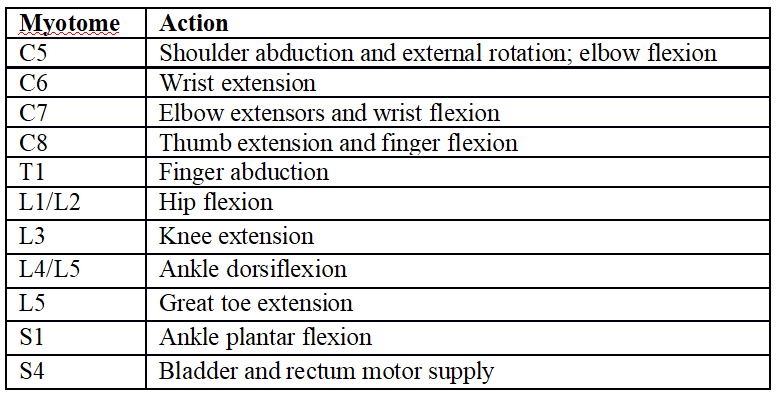
14. BUT FIRSTLY. Who can tell us what a myotome is? #bbcm
15. A myotome is a group of muscles innervated by a single spinal nerve. Below are myotomes of the upper and lower limb #bbcm
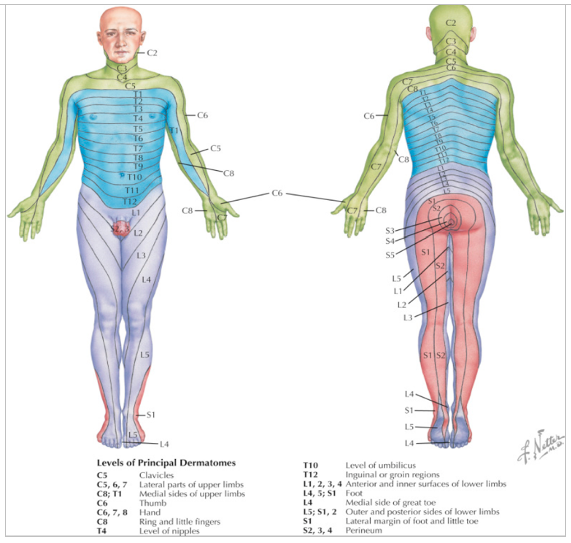
16. Now who can you tell us what a dermatome is? #bbcm
17. A dermatome is an area of skin supplied by a single spinal nerve. If you imagine the human body as a map, each dermatome represents the sensory innervation of a particular spinal nerve. Knowing your dermatomes can help to localise the level of spinal injury: #bbcm
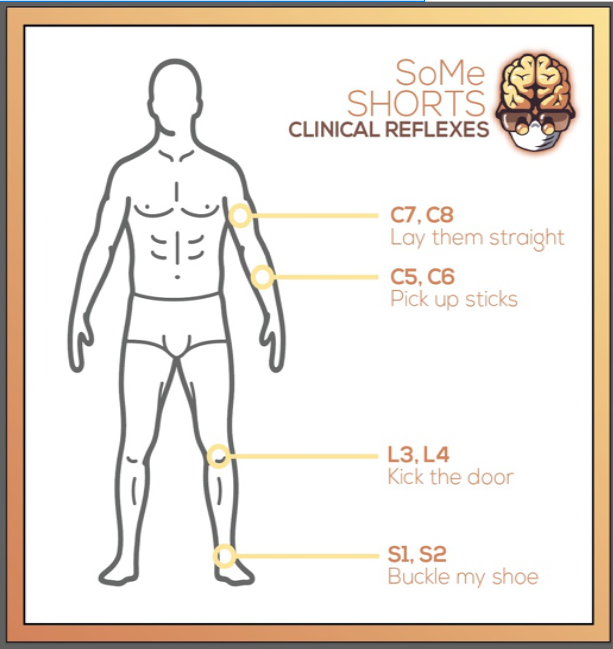
18. Understanding the nerve roots responsible for mediating specific reflexes are also useful in localising spinal pathology. Here is a useful diagram to help you remember some of the common reflexes we test. #bbcm
19. On neurological examination of the upper limb there is 4/5 weakness of all muscle groups bilaterally. Hyperreflexia is seen on testing of the biceps, triceps and brachioradialis reflex. Sensation to light touch and pin prick is reduced in all finger tips bilaterally. #bbcm
20. The patient demonstrates a positive Hoffman sign. On examination of the spine, the patient's cervical range of movement is reduced in all directions. #bbcm
21. Who can tell us what Hoffman’s sign is and what it indicates? #bbcm
22. Hoffman’s test is positive when tapping the finger nail of the ring or middle finger elicits flexion to the ipsilateral thumb. This indicates injury to the corticospinal pathway. This is a common sign seen in patients with cervical myelopathy #bbcm
23. LL examination demonstrates 5/5 strength in all muscle groups, clonus (>5 beats), hyperreflexia (3+) at both knee and ankle jerks, and an extensor plantar response (+Babinski). Sensation is intact. The patient demonstrates a stiff gait with frequent loss of balance #bbcm
24. So now that we have a diagnosis in mind, are there any specific neuro-imaging tests you’d like to perform at this stage? #bbcm
25. MRI of the cervical spine. This is the gold standard imaging modality to diagnose cervical myelopathy. It provides information about the degree of canal stenosis, disc degeneration and ligament hypertrophy. It can also delineate myelopathy caused by other pathologies. #bbcm

27. Sagittal MRI reveals multi-level cervical stenosis at C3-4, C4-C5, C5-6, C6-7 secondary to degenerative disc herniation. These findings demonstrate a spinal myelopathy secondary to cord compression #bbcm
28. Do you know any further tests we can perform? #bbcm
29. A CT scan and flexion and extension X-rays are also useful for evaluating alignment and stability especially if considering surgery! #bbcm
30. So, let's talk about cervical myelopathy #bbcm
31. In order to understand how cervical myelopathy results in the clinical presentation described it’s important to understand the anatomy of the spine. Click this link to recap on spinal anatomy #bbcm (our spinal anatomy video)
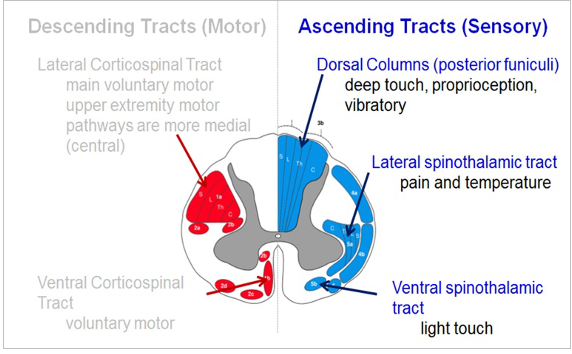
32. Cervical myelopathy is due to compression of the cervical spinal cord resulting in neurological deficits. Cervical myelopathy will frequently involve compression of the lateral corticospinal tract. This tract is involved in voluntary skeletal muscle control. #bbcm
33. The dorsal column may also be affected. This is responsible for conveying information about fine touch, 2 point discrimination, proprioception and vibration. The spinothalamic tracts (responsible for contralateral pain and temp sensation) are also commonly involved #bbcm
34. What causes cervical myelopathy? Compression can be secondary to e.g. osteophytes, hypertrophied liagamentum flavum, cervical subluxation or herniated disc. Degeneration secondary to these processes is referred to as spondylosis. #bbcm
35. This can lead to direct cord compression. As the spine ages there is a resultant degeneration of the intervertebral discs. This results in stress on the adjacent end plates and over time leads to the formation of osteophytes. #bbcm
36. As time goes on, these osteophytes can protrude into the spinal canal causing compression of the cervical spinal cord. This can also be exacerbated by hypertrophy of the liagamentum flavum which can cause stenosis by bulging into the spinal canal. #bbcm
37. These changes worsen on flexion and extension of the neck. This is because when the neck is flexed the cervical cord is compressed over the ventral osteophytes. If the neck is extended the hypertrophied liagamentum flavum protrudes into the canal and causes compression #bbcm
38. So, how does cervical myelopathy normally present? The clinical presentation of cervical myelopathy is variable and it typically depends on the extent of spinal cord injury. Symptoms are often subtle and can vary in severity from day to day #bbcm
39. Pain is usually one of the presenting features which can affect the neck, upper or lower limbs. There may be loss of motor function such as loss of digital dexterity, preventing tasks such as eating or doing up the buttons of a shirt #bbcm
40. Patients may have arm or leg weakness/stiffness leading to impaired gait and imbalance. There may be loss of sensory function causing numbness and tingling may be present. Patients may have urinary/faecal incontinence. This is less common but can occur in severe cases #bbcm
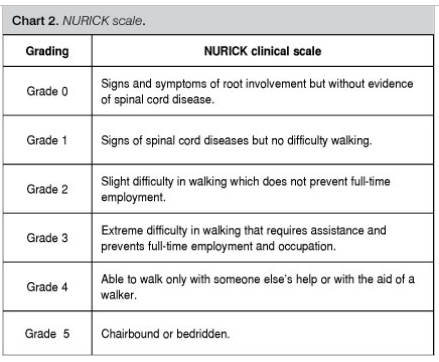
41. Right, BACK TO QUESTIONS. Are you aware of any grading systems we can use to assess the severity of cervical myelopathy? #bbcm
42. One of the most commonly used grading systems is the Japanese Orthopaedic Association scale. It's a valid and reliable grading system but is nonspecific. This grades dysfunction based on upper and lower limb motor dysfunction, sensory deficit and sphincter dysfunction #bbcm

43. Another grading system which is frequently used is the Nurick disability scale. On the other hand, this scale grades cervical myelopathy based on progressive gait disability. #bbcm
44. Now that we have confirmed the diagnosis, who can tell us any treatments for cervical myelopathy? #bbcm
45. Non-operative & operative. Non-operative management includes NSAIDS, muscles relaxant, epidural steroid injections and aggressive physiotherapy. This is mainly used in poor surgical candidates or in mild myelopathy. #bbcm
46. Operative management consists of decompressive surgery via an anterior or posterior approach. This is the mainstay treatment for cervical myelopathy. The prinary aim of surgery is to prevent the progression of spinal cord injury #bbcm
47. The timing of surgery is very important. This is because any spinal damage may be permanent so early intervention may reverse/ prevent worsening of any damage. Early treatment offers the best chance of maintaining current function. #bbcm
48. The anterior approach involves an anterior decompression and fixation (ACDF) procedure. Here, the extruded disc is removed along with osteophytes. Graft and plates are then inserted to fuse bones. Indications for this include anterior compression of 3 or less levels. #bbcm
49. Can you think of any possible complications of this approach? #bbcm
50. Many structures are at risk in the neck. One such structure is the recurrent laryngeal nerve. Damage leads to vocal cord paralysis. Other structures are the sympathetic nerves (causing Horner’s syndrome: ptosis, miosis and anhidrosis) & carotid sheath and its contents #bbcm
51. It’s also important to be aware of a post-operative retropharyngeal haematoma. This leads to airway comprise and can be fatal. The treatment is emergent decompression. Haemostasis during the procedure is therefore of the upmost importance. #bbcm
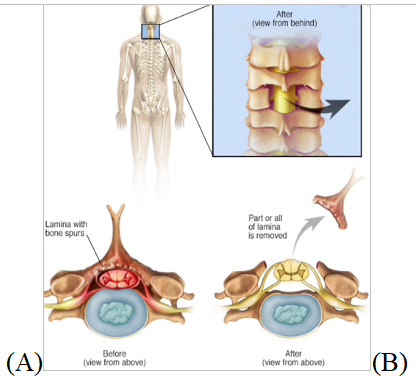
52. Posterior approaches involve a laminectomy with or without fixation. A laminectomy involves removing the lamina of the vertebrae (A). #bbcm
53. Our patient is taken to theatre where a posterior decompression is performed. Decompression is successful and she is returned to the ward for observations. She is discharged on post-op day 3 with no neurological deficits with a view to be followed up in clinic. #bbcm
54. During this time physiotherapy should continue if required. #bbcm
And with that we've reached the end of this CBD! Thanks so much for participating, please do us a favour and fill out the feedback form here: cambridge.eu.qualtrics.com/jfe/form/SV_br… Will help us improve our CBD process for next time and we hope you'll join us again! #bbcm
Huge thanks to @AlexAlamri for moderating and thank you all for joining us - see you all next time!


