
Tonight's #CBD will be moderated by @aswinchari, neurosurgery trainee & PhD student at UCL/GOSH!
A quick reminder of the rules before we begin... and let's get started! #BBGBM
A quick reminder of the rules before we begin... and let's get started! #BBGBM

1. A 65-year-old male presents to the emergency department with a 3-week history of generalized headaches, and new weakness of right arm and leg and nausea and vomiting. He has no past medical history. #bbgbm
2. Based on the history above what are your thoughts on a differential diagnosis? #bbgbm
3. We can think about three main domains! Neoplastic: primary brain tumour, metastatic brain tumour, Vascular: intracranial haemorrhage, arteriovenous malformation, Infectious: brain abscess, encephalitis. #bbgbm
4. Now that you have a few differentials in mind, you go on to obtain a further history. What questions would you like to ask? 📋 #bbgbm
5. SOCRATES, comprehensive neurological history, specifically signs of raised ICP, signs of infection/fever, hand dominance, drug history, family history, social history (remember occupation), ICE - remember a complete and thorough history! #bbgbm
6. You all correctly identified raised ICP as an important concept - what do we mean by signs of raised ICP, who can name some for us? #bbgbm
7. You guys are on fire this evening! Signs of raised ICP include: headache, vomiting 🤮 , visual disturbances, confusion, drowsiness, unconsciousness, seizures. #bbgbm
8. So, what questions are you going to ask specifically about the headache? #bbgbm
9. Site: unilateral/bilateral frontal, occipital Onset: acute or gradual Character: aching/throbbing/pulsating/pressure/pins and needles/stabbing Radiation: neck, face, eye Associated symptoms: nausea, vomiting, photophobia, rash, fever, neurological deficits, weight loss #bbgbm
10. Timing: is there a pattern to the headache, how long does it last, any diurnal variation, is it episodic? Exacerbating factors: anything improves the headache, any triggers? Severity: how is this impacting their life, is the pain getting worse, pain scale 1-10. #bbgbm
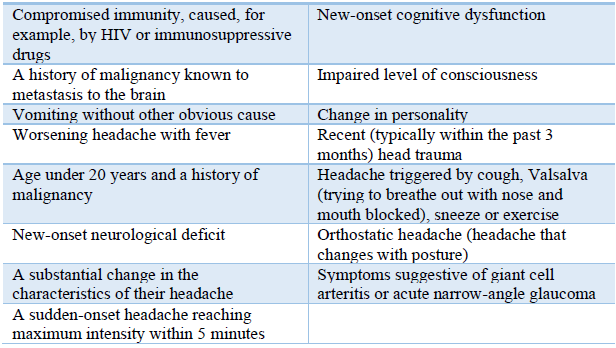
11. It’s essential to take a comprehensive headache history and be able to identify red flag symptoms that indicate the need for further investigation. Who can tell us the red flag symptoms for headache? #bbgbm
12. Red flag symptoms are possible indicators of serious pathology. Listed below are some red flag symptoms: #bbgbm
13. The patient states his headaches are now daily. They are worse first thing in the AM and when he bends over or coughs. The headache eases as he stands. It’s throbbing in nature. The pain has got worse over the past few weeks and there’s been no relief with paracetamol #bbgbm
14. Does anyone know what type of headache we call this? #bbgbm
15. This is a high-pressure headache. A high-pressure headache can indicate a raised intracranial pressure. Like in our patient, high pressure headaches typically occur first thing in the morning or when coughing/straining/bending over. #bbgbm
16. You go onto ask some further questions. The patient reports he hasn’t noticed any weight loss or fever. He says the vision in both eyes has got progressively worse over the past few weeks. #bbgbm
17. The weakness in his right arm and leg began 2 days ago. He hasn’t noticed weakness elsewhere. He denies numbness and tingling. Are there any examinations you’d like to perform at this stage? #bbgbm
18. Comprehensive upper and lower limb neurological examination, cranial nerve examination (including visual fields, pupillary response, visual acuity, fundoscopy, eye movements) and gait examination. #bbgbm
19. On examination of the cranial nerves, he has diplopia on lateral gaze bilaterally and incomplete abduction bilaterally. On fundoscopy examination, this is what you see (below). #bbgbm
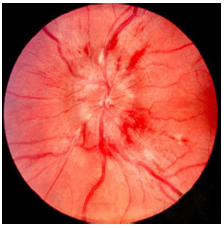
20. Does anyone know what this shows and why it occurs? #bbgbm
21. Papilloedema. This is swelling of the optic disc that is caused by increased intracranial pressure. It presents with visual disturbances (blurring, double vision, flashes, visual loss), headaches and nausea. Visual disturbances are commonly bilateral. #bbgbm
22. Can anyone give us any features of papilloedema we might find on fundoscopy examination? #bbgbm
23. Features on fundoscopy include blurring of the optic disc margin, elevation of the optic disc, loss of the optic cup, venous engorgement and loss of venous pulsation. #bbgbm
24. You move onto your neurological examination. Neurological examination reveals 3/5 weakness and mild spasticity in the right upper and lower limbs. The patient also has right hyperreflexia and a +ve Babinski. The headache is reproducible by bending over and coughing. #bbgbm
25. What type of lesion are these signs indicative of and can you name us any more features of this type of lesion? #bbgbm
26. Upper motor neurone lesion. UMN lesion features include: hyperreflexia, spastic muscle weakness, increased tone, clonus (5 beats or more is considered pathological) and extensor planter response (Babinski positive). #bbgbm
27. So now that you’ve undertaken a comprehensive history and examination, what do you think is now the main differential? #bbgbm
28. Space occupying lesion: brain neoplasm. #bbgbm
29. Are there any imaging investigations you’d like to perform to help confirm this? #bbgbm
30. MRI head is the preferred neuroimaging modality for the identification of brain tumours. MRI has high sensitivity for detecting tumours and evaluating the surrounding area to define the extent. Sometimes the patient will have a contrasted CT scan first. #bbgbm
31. An MRI with and without gadolinium is carried out. Below is the result. Can you comment on anything you see? #bbgbm
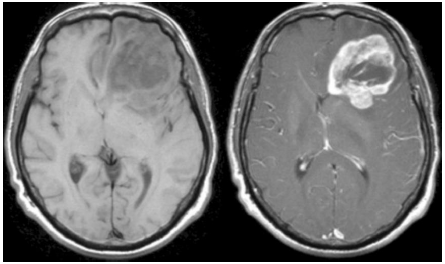
32. MRI with gadolinium (right) and without (left) shows a left sided ring enhancing tumour of the frontal lobe with surrounding oedema and midline shift. #bbgbm
33. What is the important differential for a ring-enhancing lesion on MRI? #bbgbm
34. That’s right, it’s important to rule out an intracerebral abscess. #bbgbm
35. The working diagnosis is a glioblastoma (GBM). GBM’s have characteristic features on neuroimaging. There are typically areas of necrosis, tissue oedema and leaky tumour vessels. #bbgbm
36. The oedema and leaky tumour vessels enhance quite strongly and appear as white, whereas the central necrotic area is non-enhancing and appears dark. This is called heterogenous enhancement. #bbgbm
37. Are you aware of any other tests we can do in the work up of patients with a suspected glioblastoma? #bbgbm
38. Functional MRI. The reason for this is because it can identify areas of eloquent or functionally impaired cortex and their relationship to the tumour. This can guide resection and is important for pre-operative planning. #bbgbm
39. Who can tell us what we mean by the eloquent areas of the brain? #bbgbm
40. The eloquent cortex refers to specific areas of the brain that directly controls function. This means that damage to these areas produces major focal neurological deficits. #bbgbm
41. Let's go through a few of those regions! #bbgbm
42. We have the primary motor cortex (precentral gyrus), primary somatosensory cortex (postcentral gyrus), primary visual cortex, primary auditory cortex, Broca’s area and Wernicke’s area. #bbgbm
43. Now that we have a working diagnosis, is there any test we can perform to confirm the diagnosis? #bbgbm
44. Brain biopsy. This is the only way to definitively diagnose a brain tumour and give a prognosis to guide treatment decisions. It involves obtaining a tissue sample from the tumour. The sample is sent to pathology where it’s examined, and the grade can be determined. #bbgbm
45. So, how do we obtain the sample? The patient’s pre-op imaging along with a neuro-navigation system are used to precisely located the site for biopsy. Burr holes are then created and a biopsy needle is passed into the tumour where biopsies are obtained for analysis. #bbgbm
46. A brain biopsy is performed, and the results indeed come back as a glioblastoma. Can anyone tell us what a glioblastoma multiforme is and what tissue it derives from in the brain? #bbgbm
47. A GBM is a fast-growing, aggressive glioma that develops from star-shaped glial cells called astrocytes. Their function is to support the health of the nerve cells within the brain. A GBM is a high grade astrocytoma. #bbgbm
48. We need to understand the grading systems that are used to classify astrocytomas to grade our GBM #bbgbm
49. WHO classifies astrocytic tumours into Grades I-IV. Grade I: pilocytic astrocytoma, Grade II: diffuse astrocytoma, Grade III: anaplastic astrocytoma, Grade IV: GBM. #bbgbm
50. In addition, GBM can be also classified into primary or secondary. Primary means that the GBM developed de novo; secondary means that the GBM originated from tumours of lower grade. 90% of diagnosed GBM cases are primary; 10% are secondary. #bbgbm
51. So let’s now look at how GBM’s typically present and the reasons for these symptoms. #bbgbm
52. GBM’s are characterized by their rapid, infiltrative growth. They spread across white matter tracts and blood vessels. They can outstrip their blood supply and as a result develop numerous areas of necrosis. This tissue hypoxia stimulates angiogenesis. #bbgbm
53. However, the new blood vessels that form are often faulty. These faulty blood vessels are leaky and this results in surrounding oedema, leading to an increase the intracranial pressure. This increase in ICP is what leads to headache, papilloedema, nausea and vomiting. #bbgbm
54. Depending on their location, GBM’s can cause a number of symptoms such as sensory deficits or focal motor deficits e.g. gait impairment, incoordination, apraxia, hemiparesis, hemiplegia. They can also infiltrate eloquent areas of the brain affecting vision and speech. #bbgbm
55. As a consequence of the raised ICP, false localising signs may also be present. False localising neurological signs reflect dysfunction distant from site of pathology. False signs can include cranial nerve palsies, hemiparesis, muscle atrophy and sensory features. #bbgbm
56. Sixth nerve (abducens) palsies are the most common false localising signs. This is due to its long intracranial course and its susceptibility to be compressed against the petrous temporal bone. #bbgbm
57. Quick test - who can tell us what the function of the abducens nerve is? #bbgm
58. The abducens nerve supplies the lateral rectus muscle, which is responsible for lateral gaze. Damage to the nerve will therefore results in diplopia on lateral gaze and incomplete abduction, like how our patient presented. #bbgbm
59. Are you aware of any medical treatment we can use to reduce the swelling and the symptoms associated with the GBM? #bbgbm
60. You guys know it! High dose i.v dexamethasone. Dexamethasone is a steroid drug which reduces the permeability of the tumour capillaries. It also acts as a powerful anti-emetic, reducing the nausea and vomiting associated with the tumour. #bbgbm
61. IMPORTANT! Always prescribe a proton pump inhibitor with high dose dexamethasone. #bbgbm
62. So, what treatment options exist for GBMs? Well, at present there are no curative treatment options for GBM. The survival rate of patients diagnosed remains low with a median overall survival of 15–23 months and 5-year survival is less than 6%. #bbgbm
63. The mainstay of treatment for GBM is surgery. The aim of surgery is maximal safe resection with minimal neurological morbidity, relieve mass effect and obtain adequate tissue for histological and molecular study. #bbgbm
64. The decision to perform surgery is however dependent on a number of factors including the extent of the tumour, tumour location, symptoms and performance status as per the Karnofsky score. Therefore, not all patients are candidates for surgery. #bbgbm
65. It is decided to perform surgery on our patient. At the time of surgery, the resected tumour is sent off to pathology and examined. One marker which is examined for is the MGMT promotor methylation status. This is key because it predicts response to chemotherapy. #bbgbm
66. Does anyone know what MGMT is? #bbgbm
67. MGMT is a DNA repair enzyme. This means that it prevents the tumour cells from becoming damaged by certain types of chemotherapy. Silencing of the MGMT gene by promotor methylation however means that there is reduced DNA repair and increased sensitivity to treatment. #bbgbm
68. Do you know any other treatments which may be beneficial in our patient? #bbgbm
69. After the surgery, radiotherapy can be delivered. Radiotherapy is usually given once a day, 5 days a week and over ~ 6 week period. The goal of radiotherapy is to selectively kill the remaining tumour cells which have infiltrated normal brain tissue. #bbgbm
70. Chemotherapy. The drug temozolomide is the current standard of treatment for GBM. It has been shown to be more effective in those patients who have MGMT promotor methylation. It is given concurrently with radiotherapy and as an adjuvant after completing radiotherapy. #bbgbm
71. Surgery is carried out in our patient and as much of the tumour is debulked as possible. Our patient is transferred to the HDU for close monitoring. Once the patient is stabilised and well enough, a course of radiotherapy and chemotherapy are planned. #bbgbm
72. And that’s the end of the CBD! Thanks so much everyone for your participation, as ever the quality of answers and thought has been nothing short of fantastic. It's been a pleasure discussing the case with you this evening! #bbgbm
Enormous thanks to Aswin @aswinchari for moderating and providing thought-provoking questions! Be sure to keep an eye out for future CBDs, feedback form linked in the next tweet! #bbgbm
Did you enjoy this CBD? We'd love to know your thoughts - you can let us know using the feedback form here! You'll get a shiny certificate of participation in the next few weeks!
👉 bit.ly/2WVSEms
Looking forward to seeing you all again next time! #bbgbm
👉 bit.ly/2WVSEms
Looking forward to seeing you all again next time! #bbgbm








