
1. A 54 year old female with a history of breast cancer presents with a 3 week hx of worsening headache, trouble walking and visual impairment. Her breast cancer was treated 2 years ago with wide local excision followed by radiotherapy. #BBHCP
2. Based on the history so far what are your thoughts on a differential diagnosis? #BBHCP
3. Neoplastic: metastasis, meningioma, primary glial tumour. Infectious: abscess. Vascular: intracerebral haemorrhage, AVM. Other: hydrocephalus secondary to neoplasm..
4. You begin to take a further history from the patient. She’s become increasingly drowsy and seems to be deteriorating rapidly since being in the emergency department. #BBHCP
5. What approach would you like to do to access the patient? #BBHCP
6. Of course - ABCDE! An ABCDE approach is the most appropriate in this situation. #BBHCP
7. On assessment: A: Airway is patent. B:RR is 18/min. Equal breath sounds bilaterally with no added noises. C: HR is 64 beats per minute and regular. BP is 136/86 mmHg. Capillary refill is <2 seconds. FBC, U+E, clotting screen and group and save taken 💉🔍 #BBHCP
8. D: Capillary glucose is 5.2mmol/l.
She opens her eyes to pain; she flexes to pain and she mutters incomprehensible sounds in response to your questions.
Based on your assessment what is her GCS? #BBHCP
She opens her eyes to pain; she flexes to pain and she mutters incomprehensible sounds in response to your questions.
Based on your assessment what is her GCS? #BBHCP
9. 👉8️⃣ This can be written as E2V2M4. #BBHCP
10. What does this make you worry about? 👀😲#BBHCP
11. Who do you need to call for help? ☎️📣#BBHCP
12. Totally right! The anaesthetists come and review the patient with a plan to intubate and mechanically ventilate 🌬️ #BBHCP
13. How would you like to investigate the cause of our patients deteriorating condition further? ❔#BBHCP
14. Call Radiology! An *urgent* CT head → The results of the CT head are shown below. What do you notice? 📸💀 #BBHCP 
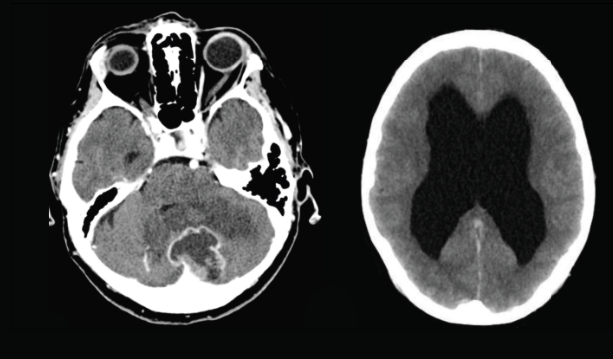
15. The CT demonstrates a solitary cerebellar metastasis (likely from our patients history of breast cancer) and hydrocephalus.. #BBHCP
16. What features from a history or examination would make you consider the lesion is in the cerebellum?🏥🩺#BBHCP
17. DANISH is a great way to remember the signs. D-Disdiadochikinesis... A-Ataxia... N-nystagmus... I-intentional tremor... S-slurred speech... H-hypotonia... 🇩🇰🥐#BBHCP
18. Signs and symptoms may vary depending on the location of the lesion in the cerebellum. If the lesion involves the cerebellar vermis there may be truncal ataxia with a broad-based gait.. 🚶🚶♂️🚶♀️#BBHCP
19. A cerebellar hemispheric lesion causes loss of co-ordination ipsilaterally, intentional tremor, past pointing, disdiadochokinesis and nystagmus. 👀👏👉#BBHCP
20. Before we consider the cause of hydrocephalus lets firstly go through the circulation and absorption of CSF 💧 This will help us understand what happens when the circulation or the absorption is disrupted in some way 🚧 #BBHCP
21. CSF is a clear, proteinaceous fluid that bathes the CNS. CSF has a number of functions. It protects the brain from damage by "buffering" the brain, it excretes waste products e.g. harmful metabolites or drugs and it transports hormones to areas of the brain🧠 #BBHCP
22. How much CSF is circulating at any given moment? 💧💧#BBHCP
23. There is around 150ml of CSF circulating at any given moment. 👍~17% of this volume is located in the ventricles and the remaining in the cisterns and subarachnoid space #BBHCP
24. CSF forms at a rate of 0.3-0.4 ml per min, this equates to 18-25ml per hour and 430-530ml per day.
Where is CSF produced? 🤷#BBHCP
Where is CSF produced? 🤷#BBHCP
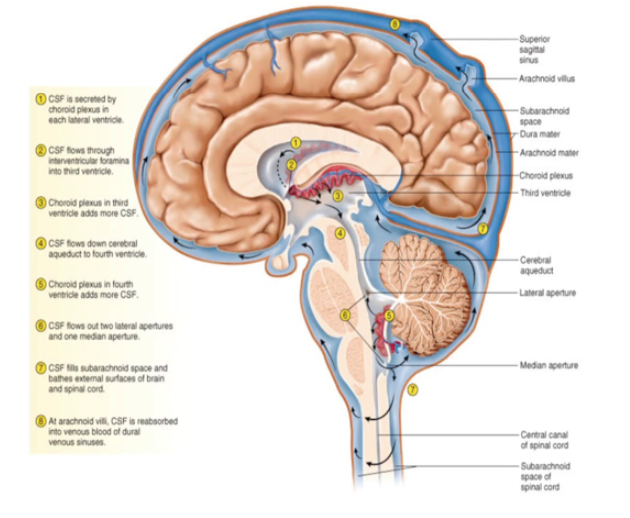
25. You all know your stuff! CSF is produced by specialised vascular tissue called choroid plexuses. The choroid plexuses are located in the lateral ventricles, third ventricle and fourth ventricle 3⃣➕4⃣ #BBHCP
26. From the lateral ventricles, CSF flows through the right and left foramen of Munro (interventricular foramen) into the third ventricle.
👇
Next, it flows through the aqueduct of Sylvius into the fourth ventricle.
The 4th ventricle is anterior to the cerebellum. #BBHCP
👇
Next, it flows through the aqueduct of Sylvius into the fourth ventricle.
The 4th ventricle is anterior to the cerebellum. #BBHCP
27. From the fourth ventricle, where does the CSF exit? #BBHCP
28. CSF may exit the foramen of Luschka laterally or the foramen of Magendie medially into the subarachnoid space.. when CSF passes through the foramen of Magendie this results in filling of the spinal subarachnoid space #BBHCP
29. When CSF passes through the foramen of Luschka this results in filling of the subarachnoid space of the cisterns and the cerebral cortex.. the level at which CSF enters the subarachnoid space is called the cerebellomedullary cistern! #BBHCP
30. CSF flow is largely dependent on the cardiac cycle. During systole, the brain vasculature expands and compresses the lateral and third ventricle. This forces CSF to flow down the cerebral aqueduct. During diastole, flow through the aqueduct reverses ❣️💙#BBHCP
31. Question time.. Does anyone know how CSF is then re-absorbed into our bloodstream? #BBHCP
32. CSF is reabsorbed through outpouchings into the superior sagittal sinus called **arachnoid granulations**. This occurs through a pressure dependent gradient 📈→ when the CSF pressure is greater than the venous pressure, CSF will flow into the superior sagittal sinus #BBHCP
33. However, the arachnoid villi provides a valvular mechanism for flow of CSF into the bloodstream. This means that even if the CSF pressure is lower than the venous pressure, the arachnoid villi will not let blood pass into the venous system.. #BBHCP
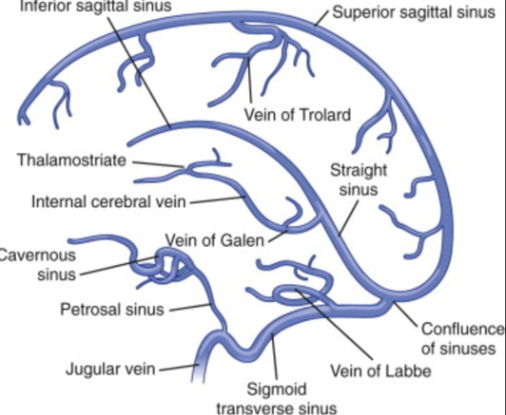
34. From the superior sagittal sinus, CSF flows into the transverse sinus via the confluence of sinus’s. From here, CSF enters the sigmoid sinus followed by the internal jugular vein - refresh your anatomy below 👇#BBHCP
35. Now we understand CSF flow let’s go onto understanding the types of hydrocephalus.
Does anyone know what are the two main types of hydrocephalus are?
#BBHCP
Does anyone know what are the two main types of hydrocephalus are?
#BBHCP
36. Communicating (non-obstructive) vs non-communicating (obstructive).
Who knows the difference between the two? #BBHCP
Who knows the difference between the two? #BBHCP
37. Non-communicating occurs when there is structural blockage within the ventricular system 🛑; whereas communicating (non-obstructive) is due to impaired CSF absorption🔬 #BBHCP
38. Who can give us some examples of the causes of communicating and non-communicating? ☝️📋 #BBHCP
39.
Non-communicating: congenital (congenital aqueduct stenosis), obstructing lesion.
Communicating: Subarachnoid haemorrhage, infective meningitis, normal pressure hydrocephalus, congenital (Dandy Walker syndrome).
#BBHCP
Non-communicating: congenital (congenital aqueduct stenosis), obstructing lesion.
Communicating: Subarachnoid haemorrhage, infective meningitis, normal pressure hydrocephalus, congenital (Dandy Walker syndrome).
#BBHCP
40. Does anyone know any other type of hydrocephalus? 🧠 #BBHCP
42. It's Hakim's/Adam's Triad!
Consisting of..
🧠Dementia, 🚶gait disturbances and 🚽urinary incontinence! #BBHCP
Consisting of..
🧠Dementia, 🚶gait disturbances and 🚽urinary incontinence! #BBHCP
43. So.. back to our patient - what do you think the cause of hydrocephalus is? 🏥 #BBHCP
44. Non-communicating (obstructive hydrocephalus) secondary to cerebellar metastasis.
As we've said, the 4th ventricle is anterior to the cerebellum. This means that lesions in the cerebellum, if large enough, can compress the 4th ventricle and affect the CSF flow ⚠️ #BBHCP
As we've said, the 4th ventricle is anterior to the cerebellum. This means that lesions in the cerebellum, if large enough, can compress the 4th ventricle and affect the CSF flow ⚠️ #BBHCP
45. If left untreated acute hydrocephalus can be fatal so emergency treatment is required.
Do you know of any ways we can treat the hydrocephalus surgically?
#BBHCP
Do you know of any ways we can treat the hydrocephalus surgically?
#BBHCP
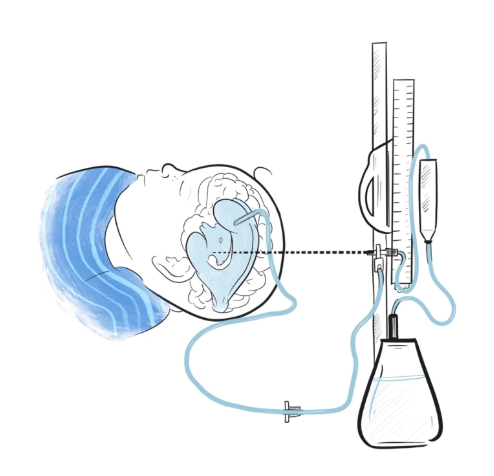
46. An external ventricular drain (EVD). An EVD is a thin drainage tube that sits outside the patient’s head, with its tip in the ventricular system. The end of the drain is connected to a measurement system and can be used to monitor the ICP! 📉#BBHCP
47. The EVD system is comprised of a collection chamber connected to a drainage bag, pressure scale and transducer. The amount of CSF drainage can be controlled by raising or lowering the external drainage system to different pressures on the pressure scale. ☝️👇📏 #BBHCP
48. Here is a beautiful illustration by @Merlin_Draws showing you what an EVD typically looks like. To find out more about what an EVD is after the CBD, or watch an insertion click these links!
Infoℹ️: brainbookcharity.org/external-ventr…
Video📺:
#BBHCP
Infoℹ️: brainbookcharity.org/external-ventr…
Video📺:
#BBHCP
49. Back to it.. they're taken to theatre and an EVD is placed. Then she is proned and undergoes a debulking of the cerebellar metastasis.
She returns to the neuro-observations unit post-operatively. Her GCS is now E3 V4 M5. She remains on the ward and is showing good recovery.
She returns to the neuro-observations unit post-operatively. Her GCS is now E3 V4 M5. She remains on the ward and is showing good recovery.
50. On day 3 the EVD is challenged. This can be done by rapid or gradual weaning. This is done in order to see the effectiveness of the EVD or to see whether any other intervention is required. #BBHCP
51. One way of challenging the EVD rapidly is to clamp the EVD and observe for any signs of raised ICP. 📈
It’s also important to examine for any CSF leak at the dressing site. This may take place over 24 hours! 🤕🕐 #BBHCP
It’s also important to examine for any CSF leak at the dressing site. This may take place over 24 hours! 🤕🕐 #BBHCP
52. Gradual weaning is done by of course by gradually changing the pressures on the EVD followed by clamping.. Again, it’s important to monitor for changes in ICP on the monitor and any clinical signs of raised ICP. #BBHCP
53. Our patients EVD was clamped for 24 hours.. Her ICP was monitored and she showed no clinical signs of raised ICP. A follow-up CT head was performed which showed persistent hydrocpehalus💧👉🧠 #BBHCP
54. Do you know what we could do if there was persisting communicating hydrocephalus and we needed a permanent treatment? ✅#BBHCP
55. Long term, hydrocephalus can be treated by a CSF diversion procedure.
A ••ventriculo-peritoneal (VP) shunt•• is typically the procedure of choice.
Who knows any other types of shunts we can use?
#BBHCP
A ••ventriculo-peritoneal (VP) shunt•• is typically the procedure of choice.
Who knows any other types of shunts we can use?
#BBHCP
56. Some include:
• Lumbo-peritoneal (LPS)
• Ventriculo-pleural (VPS) or
• Ventriculo-atrial (VAS).
Often these shunts may be required if the patient has had extensive intraabdominal surgery or high intraperitoneal pressure #BBHCP
• Lumbo-peritoneal (LPS)
• Ventriculo-pleural (VPS) or
• Ventriculo-atrial (VAS).
Often these shunts may be required if the patient has had extensive intraabdominal surgery or high intraperitoneal pressure #BBHCP
57. So what is a shunt? A shunt allows excess CSF to drain to other parts of the body. Shunts generally have 3 parts: (1) An inflow catheter (this drains the CSF from the ventricles. It leaves the brain through a small hole in the skull, which then runs under the skin)..🥤 #BBHCP
58. Secondly, (2) A valve mechanism! This regulates the pressure control through the shunt tubing. It is connected to the catheter and lies between the skin and the skull, usually on top of the head or behind the ear. #BBHCP
59. Finally, (3) An outflow catheter (this runs under the skin and moves the CSF from the valve to the peritoneal cavity, heart or other drainage site) #BBHCP
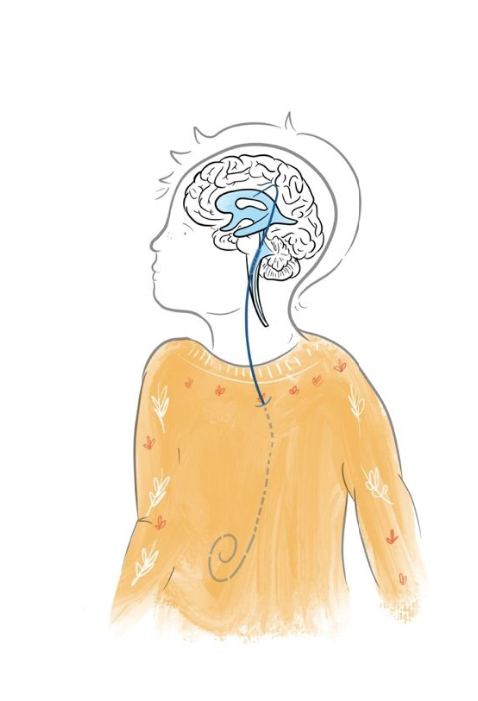
60. And what about a VP shunt? In a VP shunt a catheter is inserted into the ventricle with tubing tunnelled subcutaneously down the thorax and then further tunnelled into the peritoneal cavity where the CSF is absorbed.. another fantastic illustration from @Merlin_Draws below!
61. We've also got a video AND blog post for you for after the CBD describing it further and showing how a VP shunt is inserted.. check them out!
📼Video:
✍️Blog: brainbookcharity.org/ventriculo-per…
#Like #Comment #Subscribe #BBHCP
📼Video:
✍️Blog: brainbookcharity.org/ventriculo-per…
#Like #Comment #Subscribe #BBHCP
62. Getting closer to the end.. do you know any complications of shunting? #BBHCP
63. Over-drainage (low pressure headaches, subdural haematoma)... under-drainage... blockage... infection... disconnection... seizures... distal end problems (abdominal hernias (VPS)... cardiac arrhythmias (VAS)... ! #BBHCP
63. Back to our patient.. Our patient is doing well on the ward! 👍An MRI head is arranged and a CT chest, abdomen, pelvis to exclude any further metastatic disease and aid staging. #BBHCP
64. The MRI head confirms a good debulk of the metastasis but some residual remains. The CT chest, abdomen pelvis shows unfortunately shows reoccurrence of her breast cancer #BBHCP
65. She is commenced on high dose steroids (Dexamethasone) with a PPI 💊 The plan is for her to be discussed at the upcoming MDT to decide on the best management and plan for any further treatment options 👨⚕️👩⚕️#BBHCP
66. And that's it, folks!
Thank you so much again for joining us for another BB CBD!
We'd love your feedback as we'd love to keep making these better & better: bit.ly/2y41Xq0
(Certificates provided 😉)
A huge thank you to our moderator @aswinchari !
#MedEd #BBHCP
Thank you so much again for joining us for another BB CBD!
We'd love your feedback as we'd love to keep making these better & better: bit.ly/2y41Xq0
(Certificates provided 😉)
A huge thank you to our moderator @aswinchari !
#MedEd #BBHCP



