1. A 36 y/o male with no known past medical history presents to the emergency department with excruciating lower back and leg pain and difficulty passing urine. He reports the pain started this morning after lifting some heavy boxes. #BBCES
2. Based on the history, what are your thoughts on a differential diagnosis? #BBCES
3. Let's take a look at some answers: prolapsed disc, cauda equina syndrome, spinal stenosis, discitis, osteomyelitis, pathological compression fracture, spondylolisthesis, epidural haematoma! #BBCES
4. Now that you have a few differentials in mind, you go onto try and obtain some more information. What questions would you like to ask? 🔍⁉️ #BBCES
5. SOCRATES! 1⃣ Site- where is the back pain? Onset- did it come on suddenly or gradually? Character- what type of pain is it, is it continuous or intermittent? Radiation- does it spread anywhere?
6. 2⃣ Associated symptoms- are there any other symptoms that seem associated? (e.g. weakness / numbness / saddle anaesthesia / urinary or faecal incontinence? / weight loss? / fevers? / sweats? Timing- when did it start?
7. 3⃣ Exacerbating / relieving factors – Does anything make it better or worse? Is it worse when you walk, sit down or lay flat? Severity- on a scale of 1-10 how bad is the pain, has it got better or worse?
8. SOCRATES can help differentiate between a number of causes of back pain. It’s also useful to enquire about any previous back problems, analgesia taken, family history and social history. #BBCES
9. Typical causes of back pain can also vary according to age therefore it’s important to consider the age of the patient as this may point more towards one diagnosis over the other and can help you with your history. Some typical causes are listed below! #BBCES 
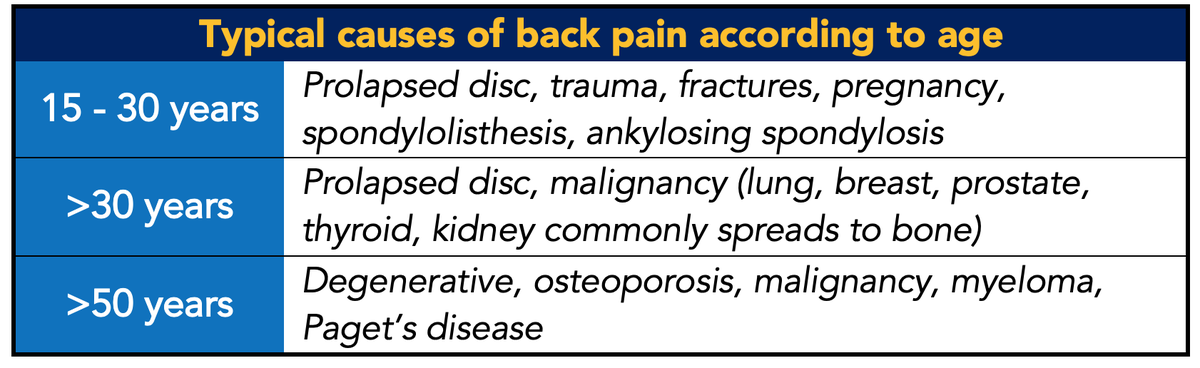
10. The goal of the history is to rule out any serious pathology. When taking the history it’s also important to rule out any red flag or concerning symptoms. Does anyone know what we mean by red flag symptoms, and can you tell us any red flags for back pain?🚩 #BBCES
11. Red flags are possible indicators of serious spinal pathology. These include: thoracic pain, fever and unexplained weight loss, bladder or bowel dysfunction, history of carcinoma... #BBCES
12. ...ill health or presence of other medical illness, progressive neurological deficit, disturbed gait, saddle anaesthesia, urinary retention or incontinence! 🏥 #BBCES
13. And how about those yellow flags? Can you name some? #BBCES
14. Yellow flags tend to be psychosocial factors, such as reduced activity levels and 'fear avoidance behaviour', social or financial problems, social withdrawal and a tendency to depression. #BBCES
15. Now, the patient reports the pain came on suddenly this morning - the pain is sharp and shooting in nature and spreads down the back of both legs into the foot. The pain is slightly worse when sitting or standing. It is not relieved by over-the-counter analgesia. #BBCES
16. Does anyone know what we call this type of pain? #BBCES
17. Some excellent answers folks - it is Radicular pain! Radicular pain is a type of pain that radiates along the course of a spinal nerve root. Radicular pain can be caused by inflammation, compression or injury to a spinal nerve root. #BBCES
18. The patient also reports his legs feel weaker than usual and he’s had some difficulty passing urine and can’t feel it when he does. He reports no weight loss, night sweats nor fever. #BBCES
19. Can you identify any red flag symptoms here?❓ #BBCES
20. Saddle anaesthesia, neurological deficit, bladder dysfunction #BBCES
21. At this point, are there any examinations you’d like to perform? #BBCES
22. A thorough neurological examination (including an assessment of perineal sensation and anal sphincter tone) should be performed early to rule out any serious spinal pathology! #BBCES
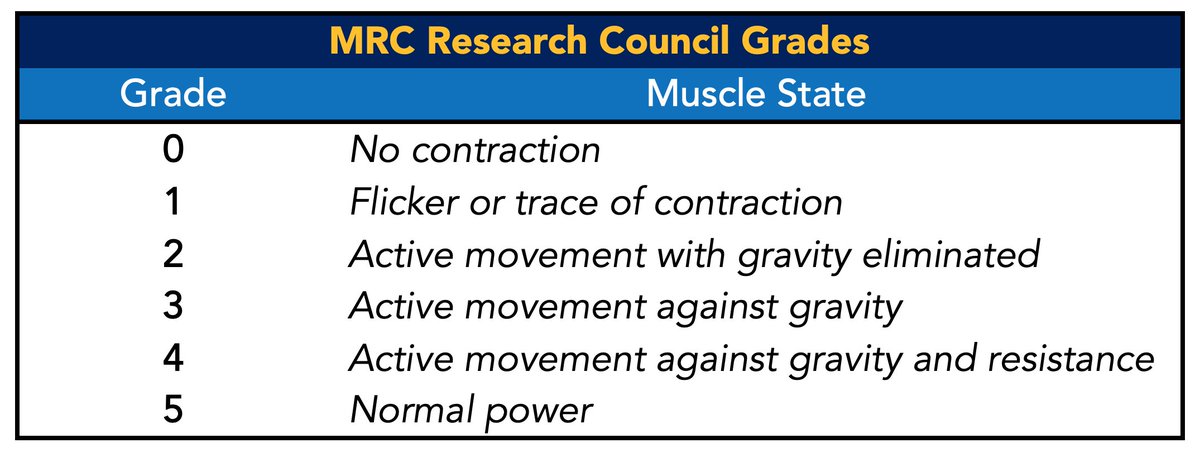
23. You begin your neurological examination. You examine power, and report he has 4/5 power in dorsiflexion, 4/5 power in plantar flexion bilaterally, and 3/5 power in extensor hallucis longus (EHL) bilaterally. #BBCES
24. Does anyone know how we grade power and what the above power grading means? #BBCES
25. The Medical Research Council (MRC) power scale is used. Muscle power is rated on a scale of 0 to 5 in relation to the maximum expected for that muscle. This table below illustrates what each grade means! #BBCES
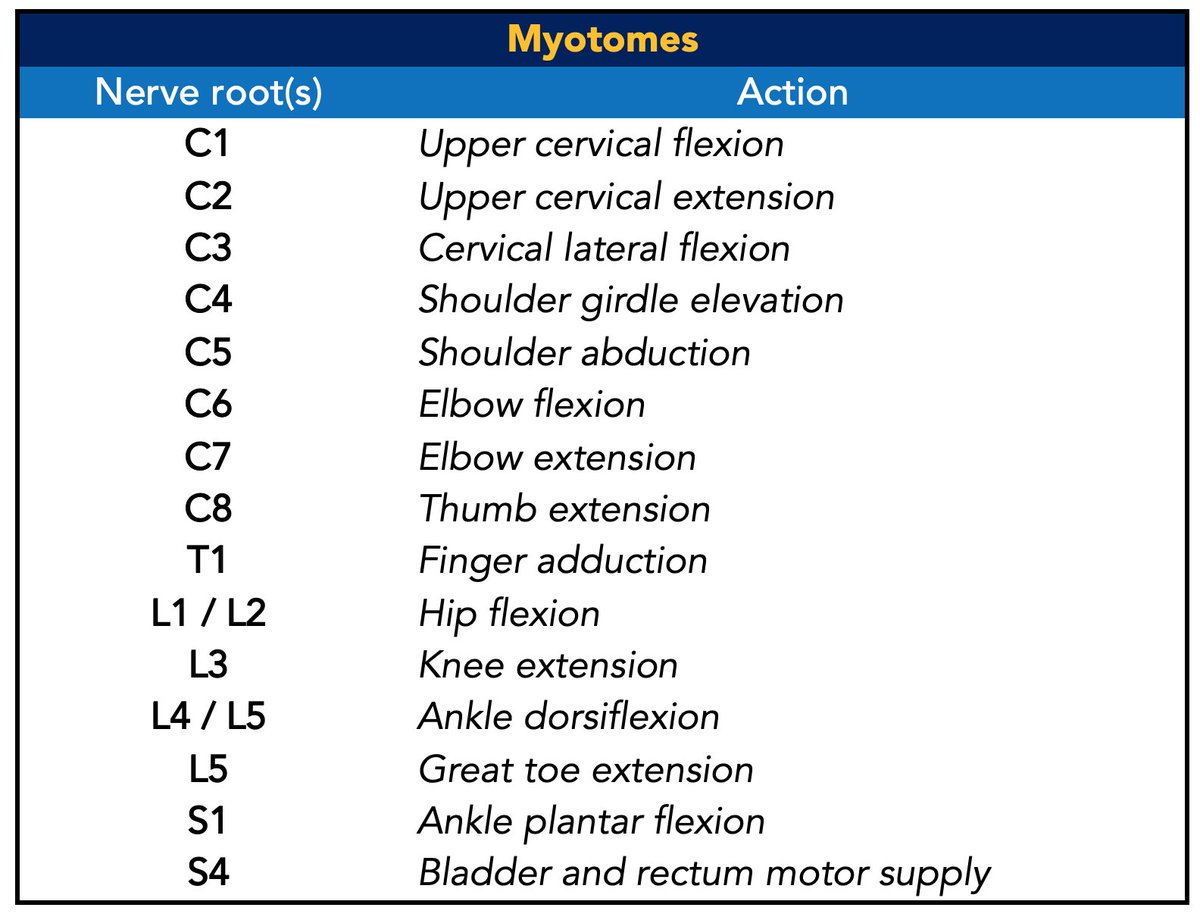
26. When examining power it’s important to understand myotomes. By systematically examining specific myotomes, we can determine the cord segments that have been injured.
Tell me, what's a myotome?👀 #BBCES
Tell me, what's a myotome?👀 #BBCES
27. A myotome is a group of muscles innervated by a single spinal nerve. Below are myotomes of the upper and lower limb! #BBCES
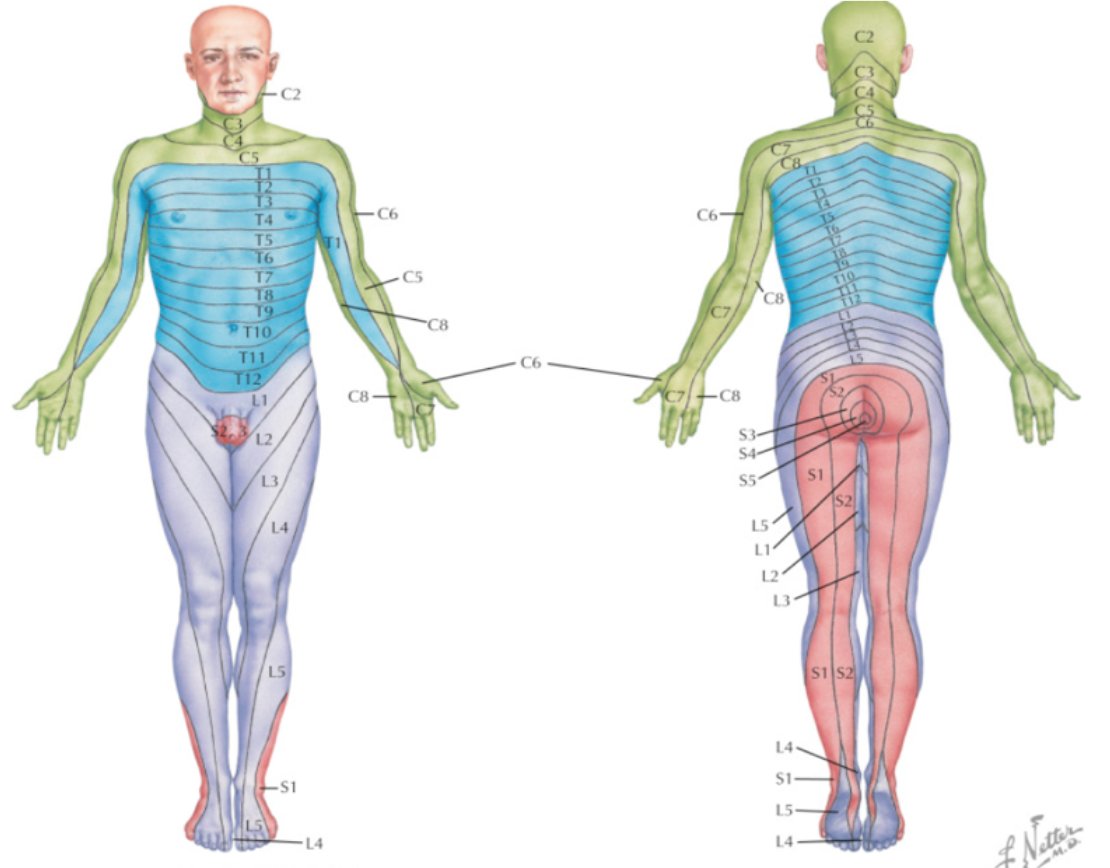
28. You move onto examining sensation and note he has sensory loss to pin prick in the perineal region. Does anyone what we’re testing here? #BBCES
29. Sacral dermatomes S2-S5! These nerves provide sensory innervation to the perineum, rectum and inner thigh. Sensory loss in the perineal region is referred to as saddle anaesthesia. #BBCES
Image: bit.ly/2wHETfS
Image: bit.ly/2wHETfS
30. You move onto examining reflexes. Reflexes can be graded according to the scale below. You report bilateral loss of ankle reflex..
Do you know what root mediates the Ankle jerk reflex?
#BBCES
Do you know what root mediates the Ankle jerk reflex?
#BBCES
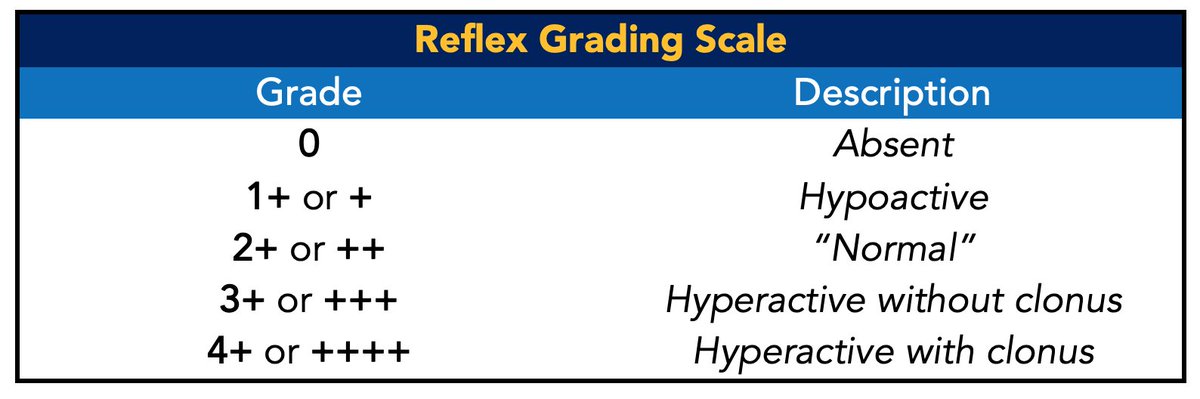
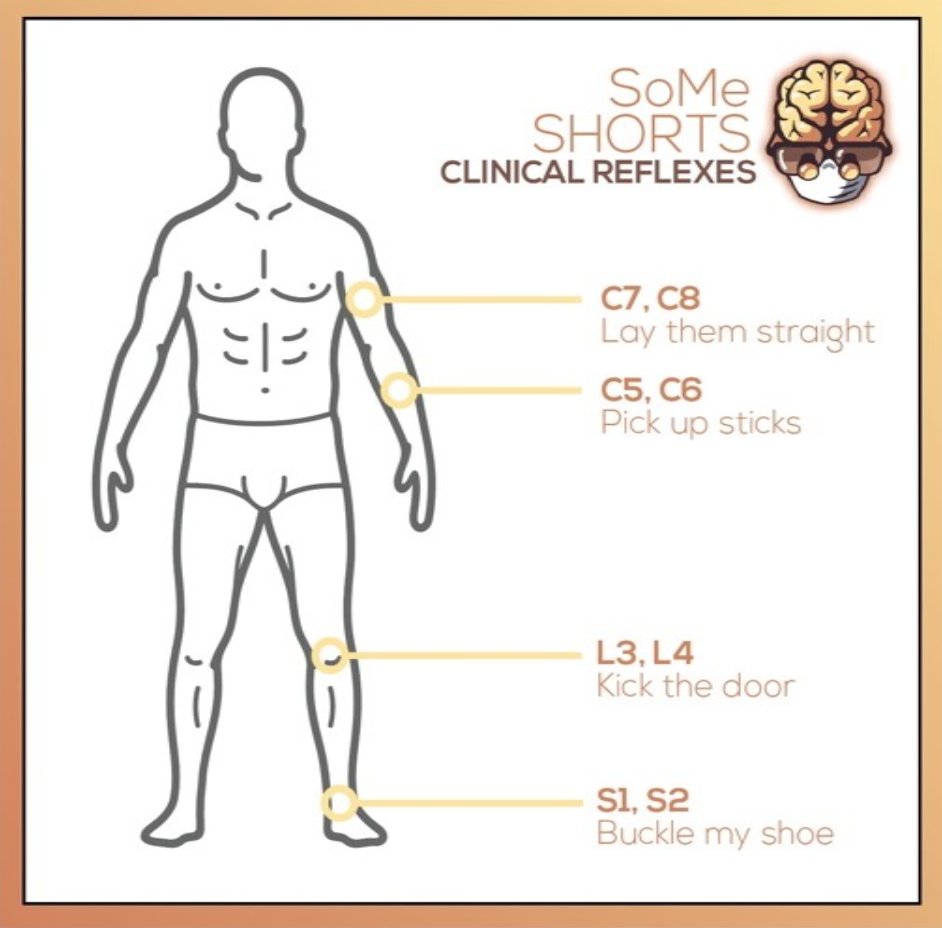
31. S1/S2! Understanding the nerve roots responsible for mediating specific reflexes are useful in localising spinal pathology. Here is a useful diagram of mnemonics to help you remember some of the common reflexes we test! 🗣️ #BBCES
32. You continue your neurological exam. There is no loss of proprioception or vibration sense. Co-ordination is normal. You perform a PR exam and report decreased rectal tone.
Are there any other tests you’d like to perform? #BBCES
Are there any other tests you’d like to perform? #BBCES
33. Bladder scan. Patients with back pain and urinary incontinence should have a urinary post-void residual volume measured: >100–200ml indicates urinary retention. The scan shows a post-void residual volume of 450ml. Painless urinary retention important thing to identify. #BBCES
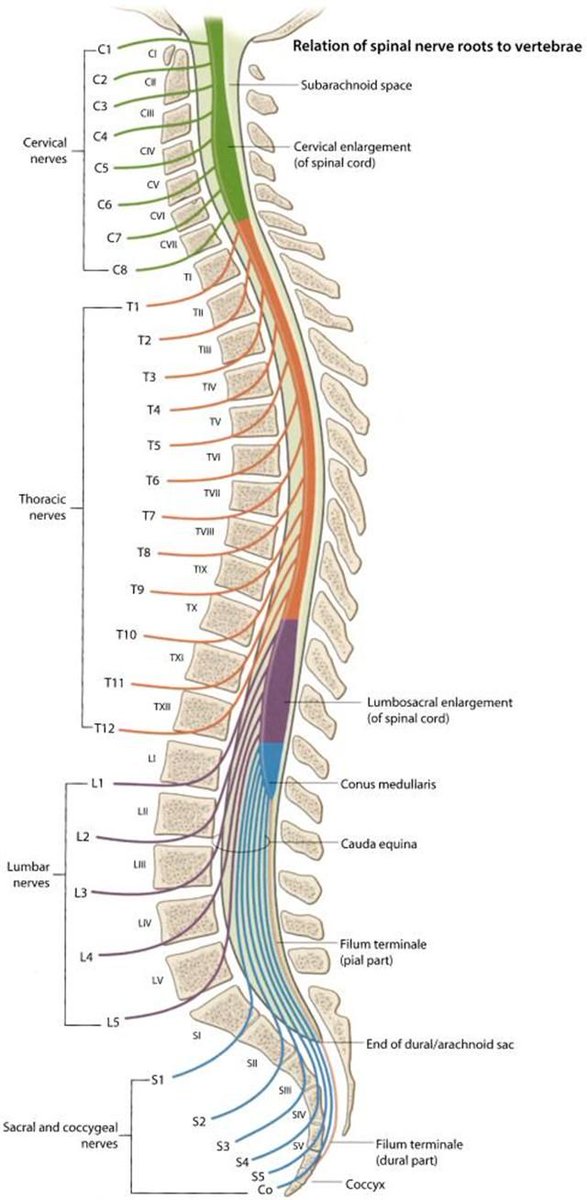
36. Let's look closer into some anatomy..
The adult spinal cord terminates at the level of the L1–L2 vertebrae. The lower distal part of the spinal cord is known as the conus medullaris, and its tapered end forms the filum terminale... #BBCES
The adult spinal cord terminates at the level of the L1–L2 vertebrae. The lower distal part of the spinal cord is known as the conus medullaris, and its tapered end forms the filum terminale... #BBCES
37. ...distal to this area is a gathering of nerve roots forming the cauda equina (the ‘horses tail’). These spinal roots separate in pairs, exiting through the nerve root foramina. #BBCES
38. The cauda equina roots have both a dorsal and ventral root. The ventral root provides motor fibres for the efferent pathway along with sympathetic fibres. The dorsal root is composed of afferent fibres for the transmission of sensation. #BBCES Image: bit.ly/2SYa4MN
39. The functions of these nerves are to provide motor innervation to the lower limb, genitals, internal and external anal sphincter and detrusor muscle of the bladder. These nerves also provide sensory innervation to the lower limb and perineum. #BBCES
40. Because of this, some people will also ask about erectile function, but in the presence of huge amounts of pain, this might not be so relevant at this point.
Now we understand the function of these nerves, lets go onto how cauda equina typically presents. #BBCES
Now we understand the function of these nerves, lets go onto how cauda equina typically presents. #BBCES
41. Compression of the cauda equina will typically present with lower motor neurone symptoms in the legs. This includes areflexia, hypotonia and muscle weakness. In cases of chronic cord compression there may be muscle atrophy. #BBCES
42. Other features of CES include back pain and sciatica, weakness and changes in sensation in the lower extremities, acute urinary retention (followed by incontinence), decreased anal tone and reduced perineal sensation. Faecal incontinence is a very late sign. #BBCES
44. Aetiology: lumbar disc prolapse, tumours, trauma e.g. fracture, infection, iatrogenic (spinal surgery or manipulation, spinal epidural injection). #BBCES
45. Most cases of CES result from disc protrusion. The intervertebral discs are a secondary cartilaginous joint. They have a tough outer layer (the annulus fibrosis) and a gelatinous core (nucleus pulposus). #BBCES
Image: bit.ly/39aw0tT
Image: bit.ly/39aw0tT
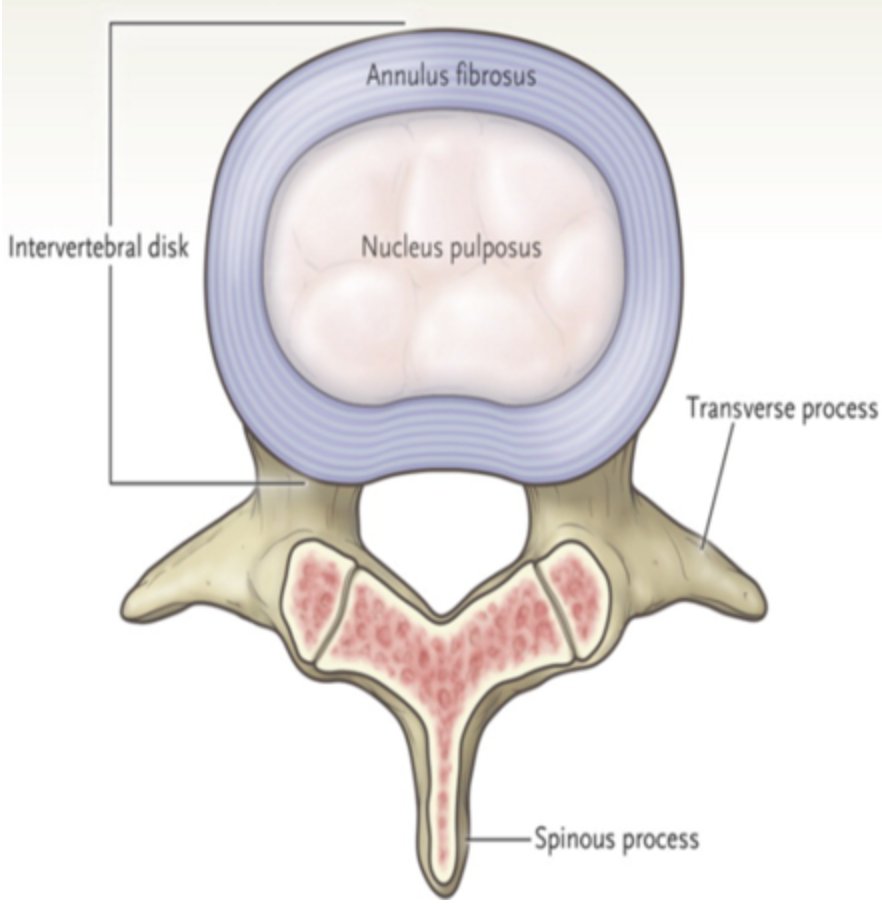
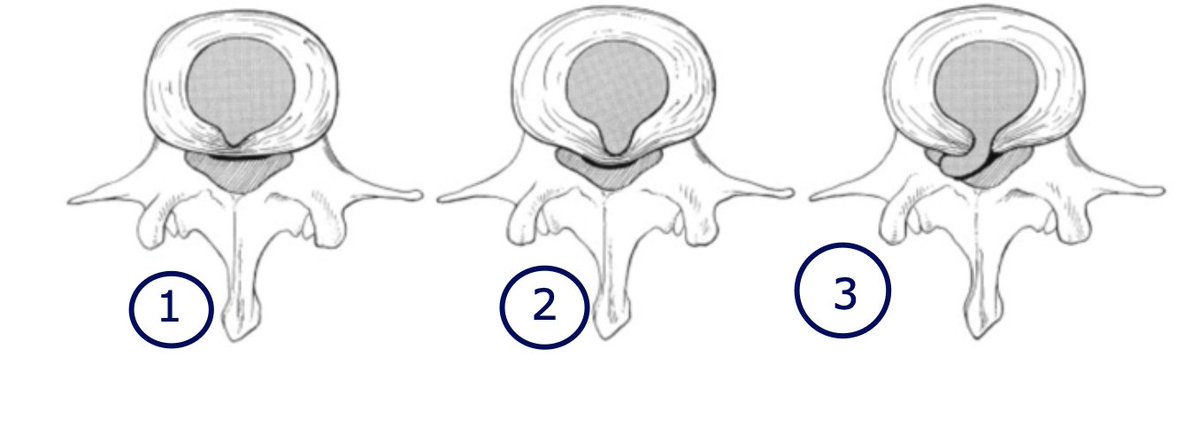
46. In a disc prolapse, the nucleus pulposus is displaced from the intervertebral space. The displacement can be 1⃣ within the disc or 2⃣ bulge without penetration of the annulus fibrosis or 3⃣ it can herniate through the annulus fibrosis into the spinal canal #BBCES
47. Disc prolapse has a variety of causes including ageing, obesity, smoking, repetitive strain, or even certain motions e.g. twisting/ turning to lift an object. CES typically results from central disc herniation. #BBCES Image: bit.ly/391fpZ4
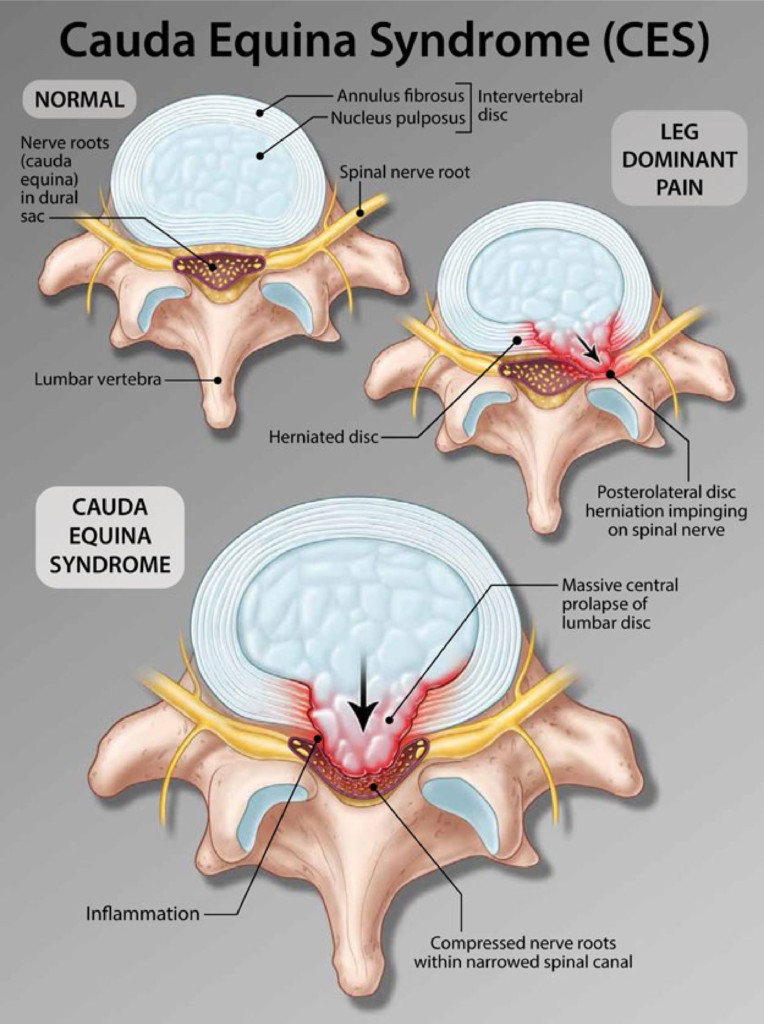
48. This disc herniation leads to compression of the cauda equina producing bilateral symptoms and the symptoms associated with CES. #BBCES
49. Now that you’re considering CES as your main differential, are there any imaging tests you’d like to perform at this stage to confirm your diagnosis and establish the cause?🦴 #BBCES
50. URGENT MRI! ⚠️ MRI is the gold standard imaging modality for the diagnosis of cauda equina syndrome.
An MRI scan is performed. Can you identify anything from the images below?
#BBCES
An MRI scan is performed. Can you identify anything from the images below?
#BBCES
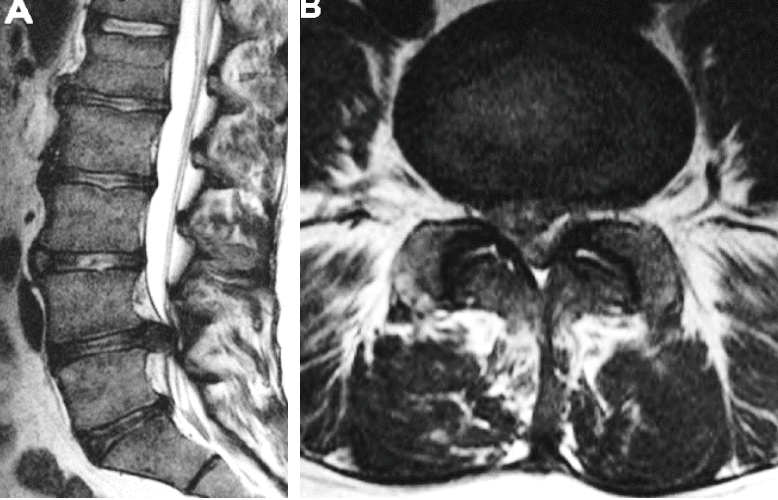
51. A sagittal midline (A) and axial (B) MRI of the lumbar spine shows an L4/5 disc herniation.
What're your next steps in the management of this patient?
#BBCES
What're your next steps in the management of this patient?
#BBCES
52. Surgical decompression! 🖋️Surgical management aims to prevent further neurological deficits by decompression of the spinal cord and/ or nerve roots. Surgery should ideally be performed within 48h of symptoms onset for better chances of stabilisation of deficits. #BBCES
53. Decompression involves a bilateral laminectomy and discectomy. A laminectomy involves removing the lamina of the vertebra. This exposes the herniated disc. The herniated disc and the extruded fragments are then removed (discectomy), decompressing the nerve roots. #BBCES
54. The surgery is a success! The patient is brought to the neurosurgery ward. Postoperatively, the patient has immediate relief of his back and leg pain, with normal power in both legs. Great! One week after, the patient is mobilising independently. #BBCES
55. Neurologically, he has 5/5 graded power in the lower limb myotomes bilaterally. Sensation to pinprick is normal bilaterally in the lower limb dermatomes, with normal reflexes. The patient is discharged from hospital with follow up planned in clinic. #BBCES
56. This patient’s evolving symptoms were caught early and surgery happened quickly. In cases where symptoms and signs have been established for a longer period of time, surgery is not usually performed as a true emergency, but expedited. #BBCES
57. And that's a wrap folks!
We really hope you enjoyed today's CbD, and hope you come back for the next one.
Huge thanks to @aswinchari for moderating!
Keep an eye out for our next Live CbD... feedback form in the next tweet!
We really hope you enjoyed today's CbD, and hope you come back for the next one.
Huge thanks to @aswinchari for moderating!
Keep an eye out for our next Live CbD... feedback form in the next tweet!
@aswinchari 58. We'd love to hear your thoughts about this CbD!
👉👉👉bit.ly/3c8hLYo
Do be sure to enter your e-mail at the end of the survey as we'll be sending out all CbD certificates so far over the next few weeks.
Survey closes tomorrow at midday!
👉👉👉bit.ly/3c8hLYo
Do be sure to enter your e-mail at the end of the survey as we'll be sending out all CbD certificates so far over the next few weeks.
Survey closes tomorrow at midday!