
1/ Live Read Through Thread
1st... a setup:
A while ago I guested on @NutritionDanny's podcast #SigmaNutritionRadio. Alan Flanagan and I discussed #Lipids, #LDL #Cholesterol, #Atherosclerosis, etc. If you haven't already listened, I highly recommend it sigmanutrition.com/episode321/
1st... a setup:
A while ago I guested on @NutritionDanny's podcast #SigmaNutritionRadio. Alan Flanagan and I discussed #Lipids, #LDL #Cholesterol, #Atherosclerosis, etc. If you haven't already listened, I highly recommend it sigmanutrition.com/episode321/
2/ Today @NutritionDanny let me know they have an article out rebutting my points found here: sigmanutrition.com/lipid-triad/
As always, I encourage you to read their article with an open mind. Then feel free to come back here for my first impressions.
Let's get started...
As always, I encourage you to read their article with an open mind. Then feel free to come back here for my first impressions.
Let's get started...
3/ Oh -- the beginning of the article includes a tweet from a #ListenThread I did when the podcast was dropped. That can be found here:
4/ I'll concede I'm a little confused on the beginning of this first section, "The ‘Lipid Profile-Centric Model'"
The article rightly zeroes on on my statement regarding a comparison of lipoprotein-centric view vs lipid profile view, but then heads into it from one side...
The article rightly zeroes on on my statement regarding a comparison of lipoprotein-centric view vs lipid profile view, but then heads into it from one side...
5/ "Dave's hypothesis of "whether the disease drives the lipid profile…” (i.e., reverse causality)"
To be sure, I wasn't suggesting this is reverse causality -- as in, atherosclerosis categorically causes high LDL.
To be sure, I wasn't suggesting this is reverse causality -- as in, atherosclerosis categorically causes high LDL.
6/ I was discussing whether diseases can drive lipid profiles that in turn create the association regarding concentration.
Let's look at T2 Diabetes as an example...
Let's look at T2 Diabetes as an example...
7/ T2 Diabetes (a disease) can have a higher association of
(1) atherogenic dyslipidemia + higher preponderance of small dense LDL, and
(2) greater risk of atherosclerosis.
Does T2D caused (1), which then cause (2)?
... or is it possible T2D causes both (1) and (2)?
(1) atherogenic dyslipidemia + higher preponderance of small dense LDL, and
(2) greater risk of atherosclerosis.
Does T2D caused (1), which then cause (2)?
... or is it possible T2D causes both (1) and (2)?
8/ Of course, the above is a rhetorical question, but is important to unpack if we discussing claims of causality given it is easily removed.
Take away other risk factors associated with higher CVD and you can better look at the one of interest (LDL) to confirm profile relevance
Take away other risk factors associated with higher CVD and you can better look at the one of interest (LDL) to confirm profile relevance
9/ The article also brings up Bradford Hill, which I definitely welcome. But to be sure, there's not three criteria, there are nine. In fact, the second (and many would argue, most important) is "Consistency".
It's worth taking a moment to read sciencebasedmedicine.org/causation-and-…
It's worth taking a moment to read sciencebasedmedicine.org/causation-and-…
10/
"2) Consistency. Almost every study should support the association for there to be causation."
"2) Consistency. Almost every study should support the association for there to be causation."
11/ At the end of the first section and I'm still unsure of the disagreement specifically. I state later in the podcast that I believe ApoB containing Lps are a participant in atherogenesis (but make the point that so are many other things, like macrophages)...
12/ Per my quote, I'm advocating for looking at LDL in context of high HDL and low TG to determine if it is still associated with a high rate of atherosclerosis as the lipid hypothesis would lead us to assume. It's why I wanted to kick off the podcast in that context...
13/ I appreciate the work put into this article, but this first section is answering a question outside the proposition I'm putting forward.
Or to put it another way, I'm not surprised we'd find this association with CVD when we make no distinction of the context I'm pointing to
Or to put it another way, I'm not surprised we'd find this association with CVD when we make no distinction of the context I'm pointing to
14/ On to "Atherogenic Dyslipidemia and the ‘Lipid Triad’" section...
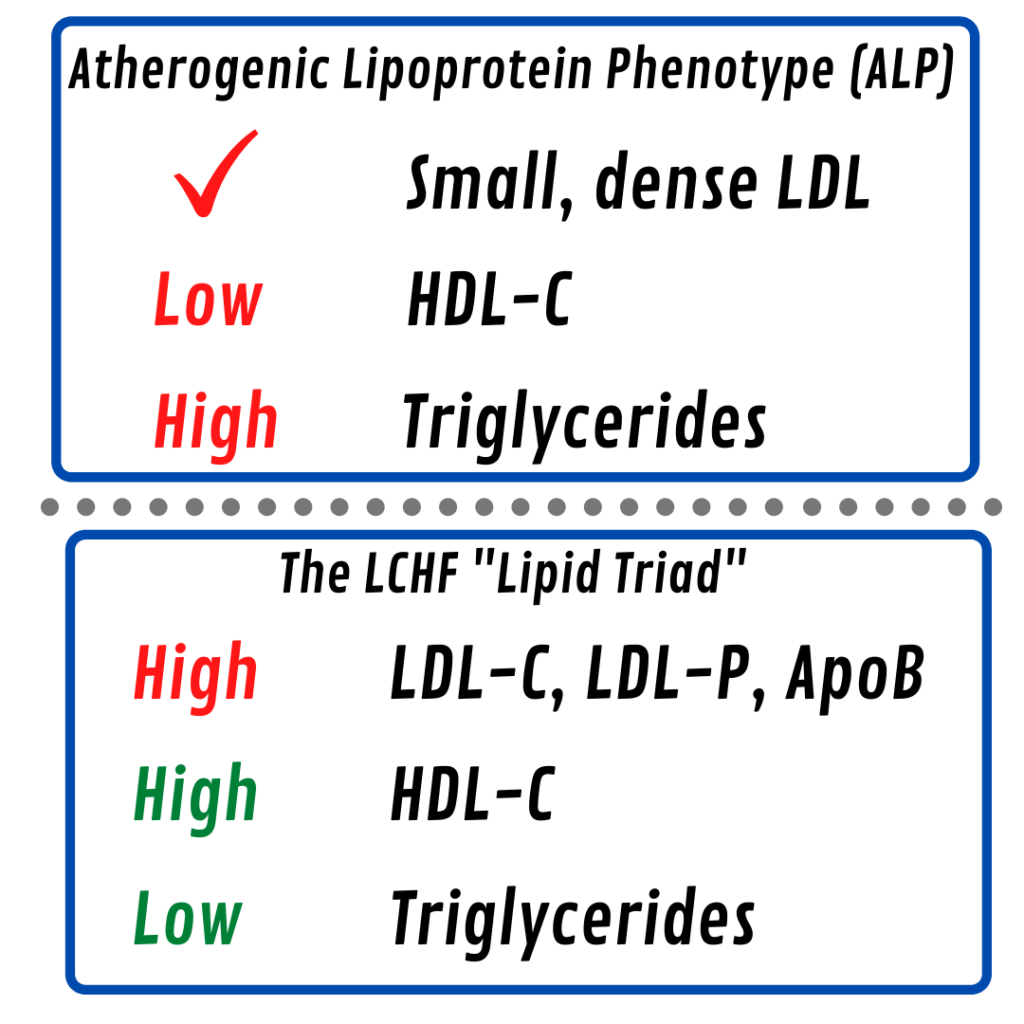
15/ "
The contention Feldman seems to offer in support of the "Lipid Triad" is that, as the ALP is known to be atherogenic, if the reverse is the case (i.e. high-HDL and low-TGs), then perhaps this is protective or at least a much less risk:
"
The contention Feldman seems to offer in support of the "Lipid Triad" is that, as the ALP is known to be atherogenic, if the reverse is the case (i.e. high-HDL and low-TGs), then perhaps this is protective or at least a much less risk:
"
16/ I'm quoted from the podcast: 

18/ They make two important distinctions--
"Independent risk factor: biomarker in a causal pathway between the exposure and outcome.
Systems biomarker: biomarker which provides indications of underlying cardio-metabolic processes, but are not causal independently."
"Independent risk factor: biomarker in a causal pathway between the exposure and outcome.
Systems biomarker: biomarker which provides indications of underlying cardio-metabolic processes, but are not causal independently."
19/ "Both HDL and triglycerides are appropriately classed as systems biomarkers; neither are causally associated with CVD in themselves."
I'll concede I had to reread that a couple times...
I'll concede I had to reread that a couple times...
20/ This section is interesting as it seeks to minimize both HDL and TG individually, yet concedes their role as "systems biomarkers".
HDL does have both a tight inverse association with CVD, and its Reverse Cholesterol Transport is highly studied...
HDL does have both a tight inverse association with CVD, and its Reverse Cholesterol Transport is highly studied...
21/ Regardless, I think the term "systems biomarkers" is a perfectly fine roundabout way to bring us back to "lipid profile" anyway.
It puts more focus on the why of their levels rather than assuming the action itself.
It puts more focus on the why of their levels rather than assuming the action itself.
22/ Again -- and with emphasis -- I don't think high HDL is that much "more protective" and TG is that much "more atherogenic" inherently.
Rather, I think many disease states are themselves atherogenic and can *result* in lower HDL and higher TG (atherogenic dyslipidemia)
Rather, I think many disease states are themselves atherogenic and can *result* in lower HDL and higher TG (atherogenic dyslipidemia)
23/ Next section, "Remnant Lipoproteins"
Dave Feldman [19:58]: “... you probably have a higher preponderance of VLDLs, and that does tend to be associated with atherogenic dyslipidemia... And remnants are, as a profile, definitely highly associated with cardiovascular disease…”
Dave Feldman [19:58]: “... you probably have a higher preponderance of VLDLs, and that does tend to be associated with atherogenic dyslipidemia... And remnants are, as a profile, definitely highly associated with cardiovascular disease…”
24/ This section concludes with
"Feldman's Claim: Remnant lipoproteins are "definitely highly associated with cardiovascular disease" but LDL-C is not a risk factor."
It's worth looking at the paragraph this was taken from here:
"Feldman's Claim: Remnant lipoproteins are "definitely highly associated with cardiovascular disease" but LDL-C is not a risk factor."
It's worth looking at the paragraph this was taken from here:

25/ I was discussing remnant lipoproteins in the context of the association with atherogenic dyslipidemia (which I think is agreed on) but in particular, I was pointing to how it is likewise associated with TG levels and how this likewise associates with all cause mortality.
26/ The last section is on inflammation, but isn't as interesting to me given the context of our conversation that my statement is being applied to. Worth reading the transcript to better understand the EAS study we were talking about at that time.
27/ I'm very thankful for both @NutritionDanny and Alan having that podcast and I think we unpacked a lot. I'll concede I was hoping for more with this followup article, such as a more specific rebuttal to the triad as a profile, especially if we had good data for it...
28/ All that said, I'm hopeful this represents more proactive dialog/debate on this important subject.
And without question, I'd love if one or both of you would consider coming on my channel where we could continue this conversation further. :)
And without question, I'd love if one or both of you would consider coming on my channel where we could continue this conversation further. :)




{kind=link}