
If we want to control this outbreak, we need to strengthen the connection between health care providers, labs and public health agencies
There are lots of problems, but some real low-hanging fruit too
We assembled an A+ team to find them and make a plan
healthpolicy.duke.edu/sites/default/…
There are lots of problems, but some real low-hanging fruit too
We assembled an A+ team to find them and make a plan
healthpolicy.duke.edu/sites/default/…
2/ We had 2 principles:
*Focus on the next 30-90 days: Immediate needs call for immediate solutions.
*Use existing systems rather than building new systems: There's been more progress in #healthIT than people realize. Let's use it.
Building new systems in a pandemic won't work
*Focus on the next 30-90 days: Immediate needs call for immediate solutions.
*Use existing systems rather than building new systems: There's been more progress in #healthIT than people realize. Let's use it.
Building new systems in a pandemic won't work
3/ The team was truly phenomenal.
epidemiologists @CSTEnews
public health officials @ASTHO
privacy experts @HealthPrivacy
public health lawyers @networkforphl
standards gurus @amalec
health information exchange @paul_wilder
..and many more informal advisers
No one said no
epidemiologists @CSTEnews
public health officials @ASTHO
privacy experts @HealthPrivacy
public health lawyers @networkforphl
standards gurus @amalec
health information exchange @paul_wilder
..and many more informal advisers
No one said no
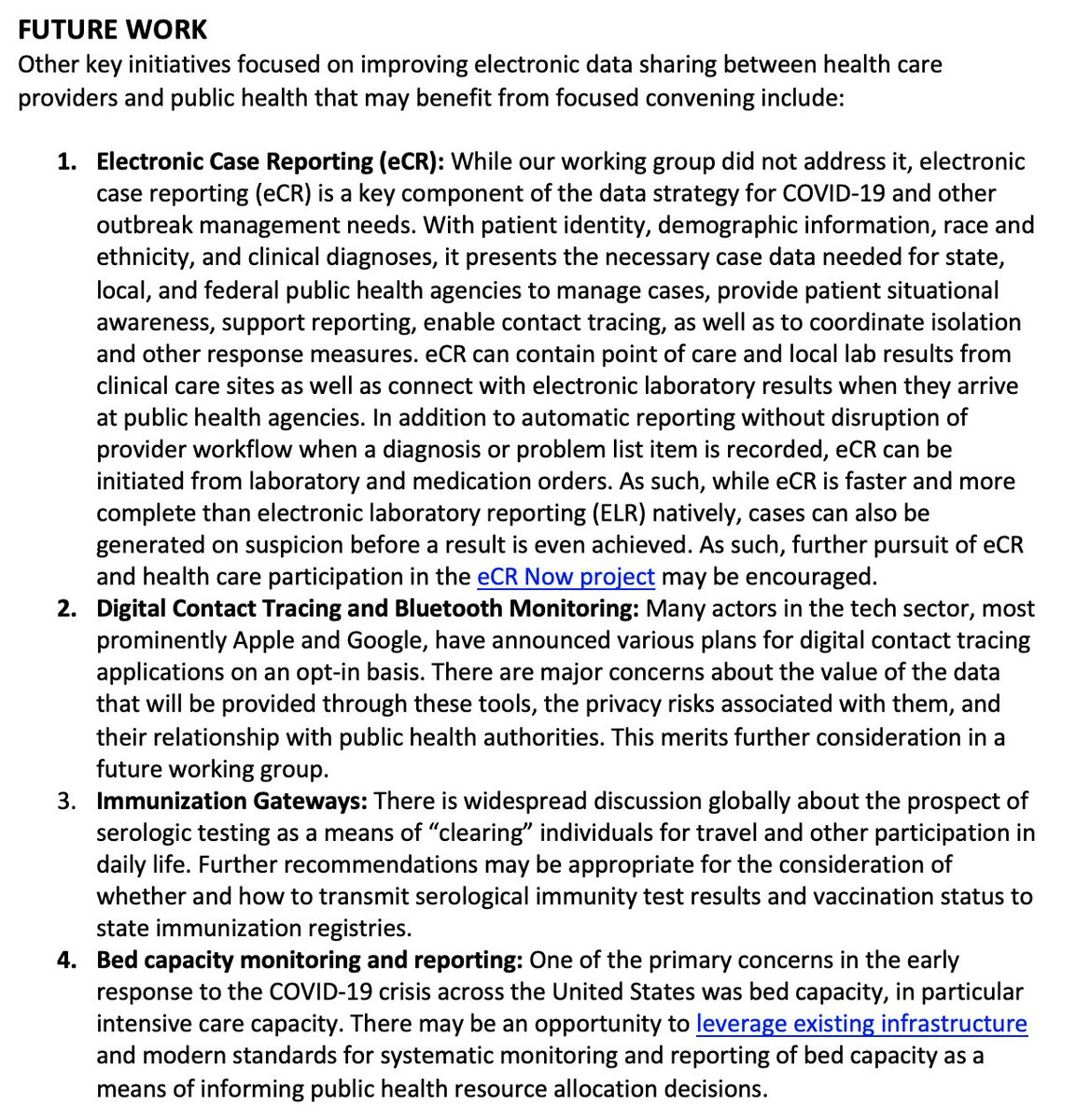
4/ There are lots of connections that are important, including some we didn't tackle b/c not clear they need help
*Case Reporting (eCR Now)
*Digital Contact Tracing
*Immunization Gateways
*Bed capacity monitoring and reporting
ecr.aimsplatform.org/ecr-for-covid-…
ainq.com/thesanerprojec…
*Case Reporting (eCR Now)
*Digital Contact Tracing
*Immunization Gateways
*Bed capacity monitoring and reporting
ecr.aimsplatform.org/ecr-for-covid-…
ainq.com/thesanerprojec…
5/ There are 3 things we believe could be tackled quickly, where targeted action could make a big difference
*Lab report completeness (demographic, contact information)
*Enabling Public Health to query Clinical Data Exchanges
*Enhancing National Syndromic Surveillance
#COVID19
*Lab report completeness (demographic, contact information)
*Enabling Public Health to query Clinical Data Exchanges
*Enhancing National Syndromic Surveillance
#COVID19
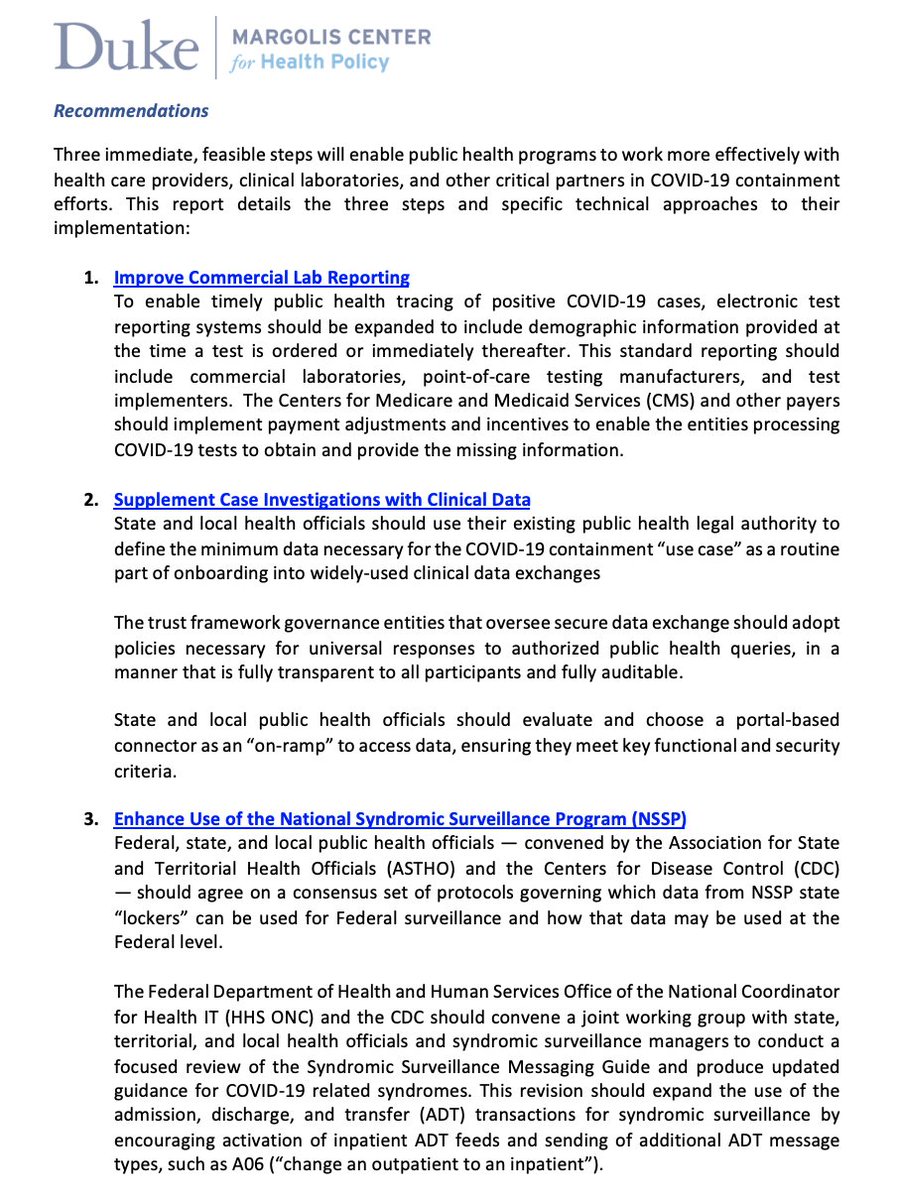
6/ First, Lab Reporting.
Up to 50% of lab reports submitted to public health lack patient address or zip code (!)
That's a big problem for identifying infection clusters, localizing disease hotspots, contacting cases
to complete investigations, and matching patient information
Up to 50% of lab reports submitted to public health lack patient address or zip code (!)
That's a big problem for identifying infection clusters, localizing disease hotspots, contacting cases
to complete investigations, and matching patient information
7/ There are lots of failure points, but this is higher than public health usually sees
An intriguing theory is that labs need (& get) pt address if they're going to bill the patient; the lack of address may be an unintended consequence of "no copays for COVID testing" by law 👀
An intriguing theory is that labs need (& get) pt address if they're going to bill the patient; the lack of address may be an unintended consequence of "no copays for COVID testing" by law 👀
8/ How can labs get the missing info, to pass on to public health? Lots of ideas, the most intriguing of which was to enable queries for contact information based not on the usual 5 matching fields:
FNAME LNAME DOB GENDER + ZIP
but rather with:
MRN +DOB
Payer + Subscriber #
💡
FNAME LNAME DOB GENDER + ZIP
but rather with:
MRN +DOB
Payer + Subscriber #
💡

9/ Our privacy experts confirmed that labs would be allowed to make these queries under HIPAA Payment, Treatment, Operations provision
Who might step up to create such an information service?
@CommonWell @Verato_Software @LexisNexis @Experian @Surescripts
verato.com/blog/accelerat…
Who might step up to create such an information service?
@CommonWell @Verato_Software @LexisNexis @Experian @Surescripts
verato.com/blog/accelerat…
10/ But here's the beauty of people experienced in policy.
We didn't try to hardwire the solution.
We said, let's give labs the incentive to get--and send--timely and complete information. They will figure it out.
..and Mark McClellan knows how to craft financial incentives
We didn't try to hardwire the solution.
We said, let's give labs the incentive to get--and send--timely and complete information. They will figure it out.
..and Mark McClellan knows how to craft financial incentives

11/ On the same day we released these interoperability recommendations, we also released a companion set of recommendations for "Health Care Payment to Support
COVID-19 Detection and Containment"
(which deserve their own thread)
w Mark, me, and Tom Barker
healthpolicy.duke.edu/sites/default/…
COVID-19 Detection and Containment"
(which deserve their own thread)
w Mark, me, and Tom Barker
healthpolicy.duke.edu/sites/default/…
12/ The second problem we tackled was how to help public health case investigators gain access to hospital records quickly and efficiently.
Right now, it's still often "call and fax" which is what I did 20 years ago.
But hospital IT and interoperability have changed enormously.
Right now, it's still often "call and fax" which is what I did 20 years ago.
But hospital IT and interoperability have changed enormously.

13/ Despite the jeremiads of critics, the $30B spent on the HITECH Act (part of the last stimulus, which now seems quaint, what with $175B in "immediate relief") made health records electronic, and portable.
I'm proud to have been a part of it @ONC_HealthIT from 2009-2014
I'm proud to have been a part of it @ONC_HealthIT from 2009-2014
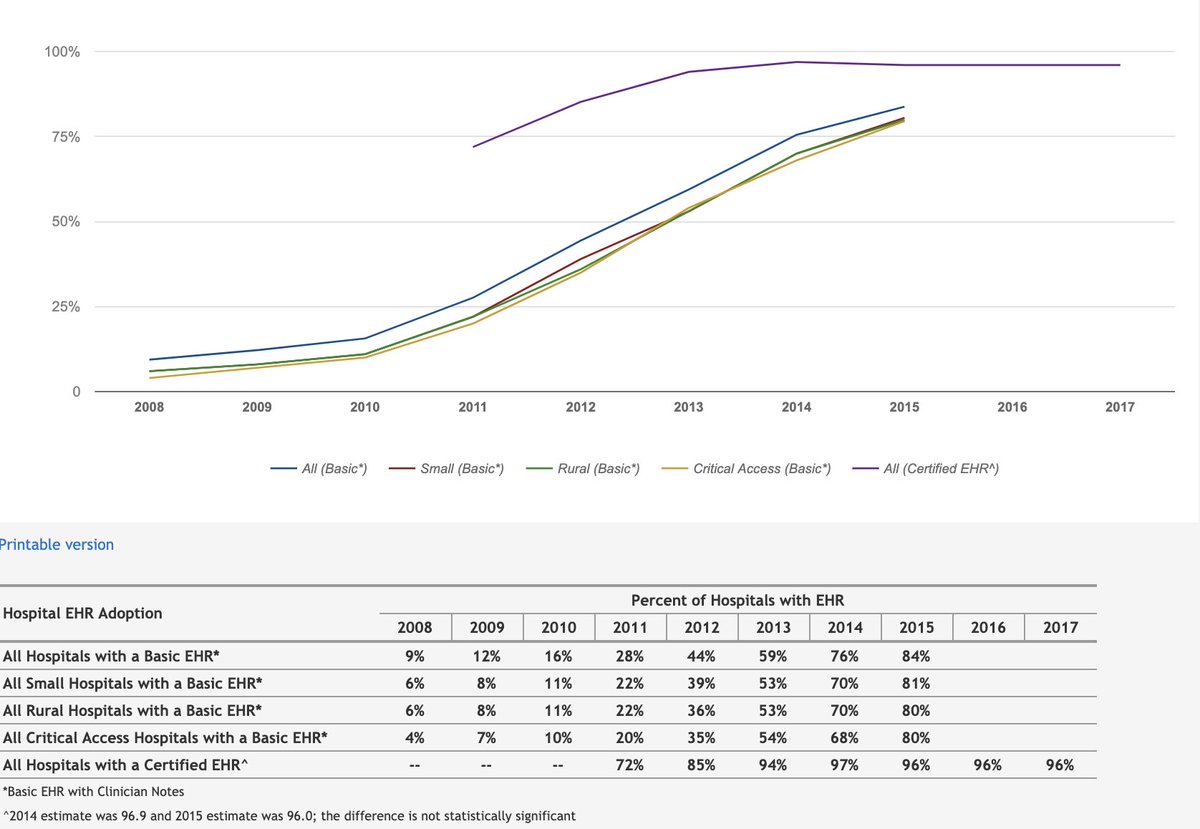

14/ The enormous amount of work in the field by #HealthIT workers in the past decade to update EHRs, adopt standards, establish data clinical exchanges, work through the millions of connection problems have taken us far past the "Connectathons" of yore
Most people don't know it
Most people don't know it
15/ In particular, three clinical data exchange networks now serve different chunks of the hospital EHR ecosystems.
@CommonWell has @Cerner @MEDITECH @cpsiehr (and others)
@CarequalityNet has Epic
@eHealthExchange has @VeteransHealth @DoD_DHA many HIEs
And they're connecting
@CommonWell has @Cerner @MEDITECH @cpsiehr (and others)
@CarequalityNet has Epic
@eHealthExchange has @VeteransHealth @DoD_DHA many HIEs
And they're connecting
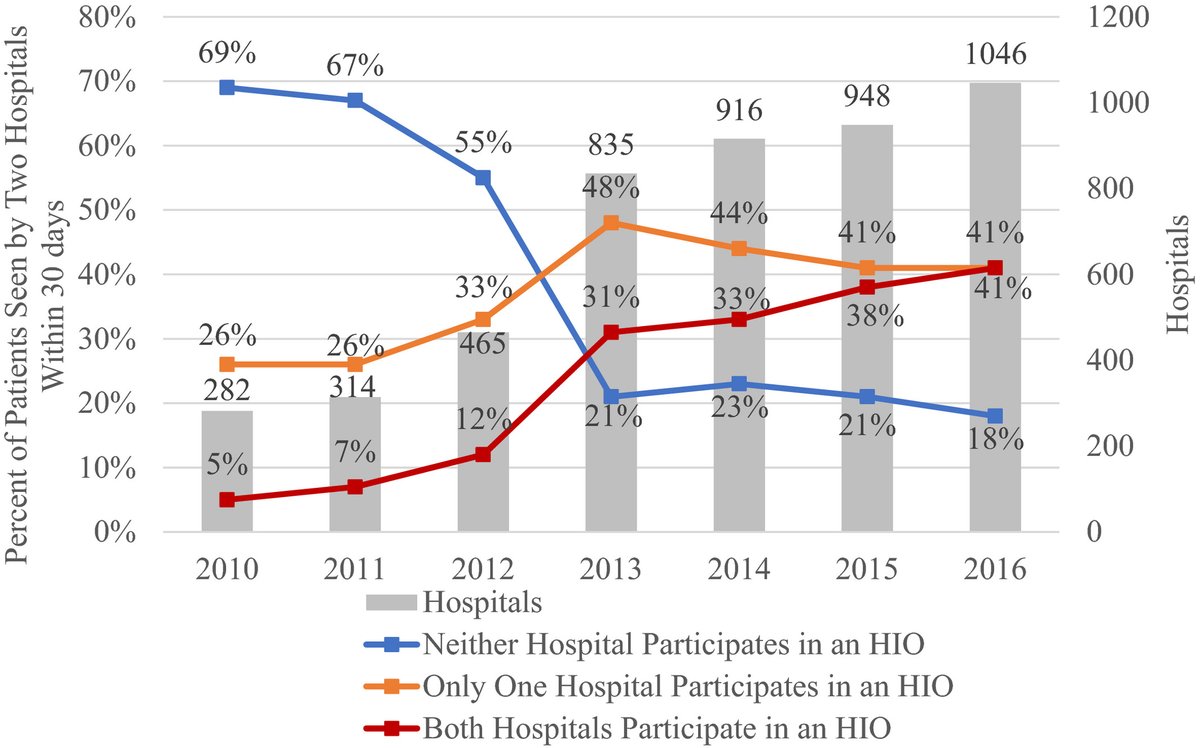
16/ There are literally millions of clinical queries that are being returned by these intermediaries using standardized Common Clinical Data CCD documents
Sadly public health access wasn't prioritized
But we are seeing in COVID19 that healthcare can move,+faster than imaginable
Sadly public health access wasn't prioritized
But we are seeing in COVID19 that healthcare can move,+faster than imaginable
17/ With the volume of positive case reports pouring in- 30,000 a day for the foreseeable future- public health needs more efficient ways of getting clinical data
Is the patient hospitalized or in the ICU?
Risk factors?
Co-morbidities?
Medications?
Labs?
it's all in the CCD
Is the patient hospitalized or in the ICU?
Risk factors?
Co-morbidities?
Medications?
Labs?
it's all in the CCD
18/ We learned that there are only 3 things we need before state/local health departments could get seamless access to these clinical data exchanges.
We need:
*public health to say they need it (literally)
*the exchanges to agree to respond every time (they want to)
*an on-ramp
We need:
*public health to say they need it (literally)
*the exchanges to agree to respond every time (they want to)
*an on-ramp
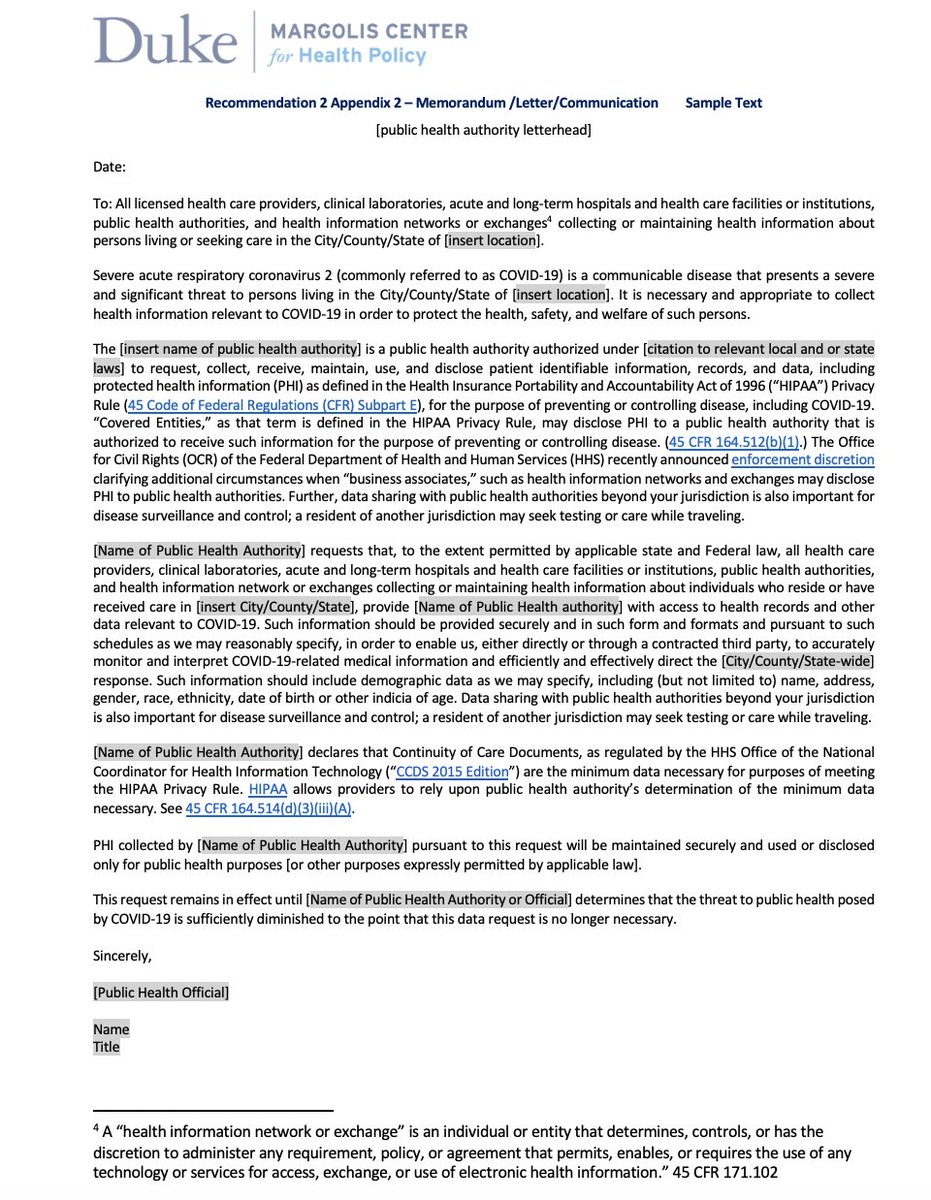
19/ As a legal matter, hospitals as covered entities under HIPAA are allowed to give data to public health- and with @HHSOCR swift action, their business associates can act on their behalf
But some hospitals want public health to assert that authority, and say what they need-OK!
But some hospitals want public health to assert that authority, and say what they need-OK!
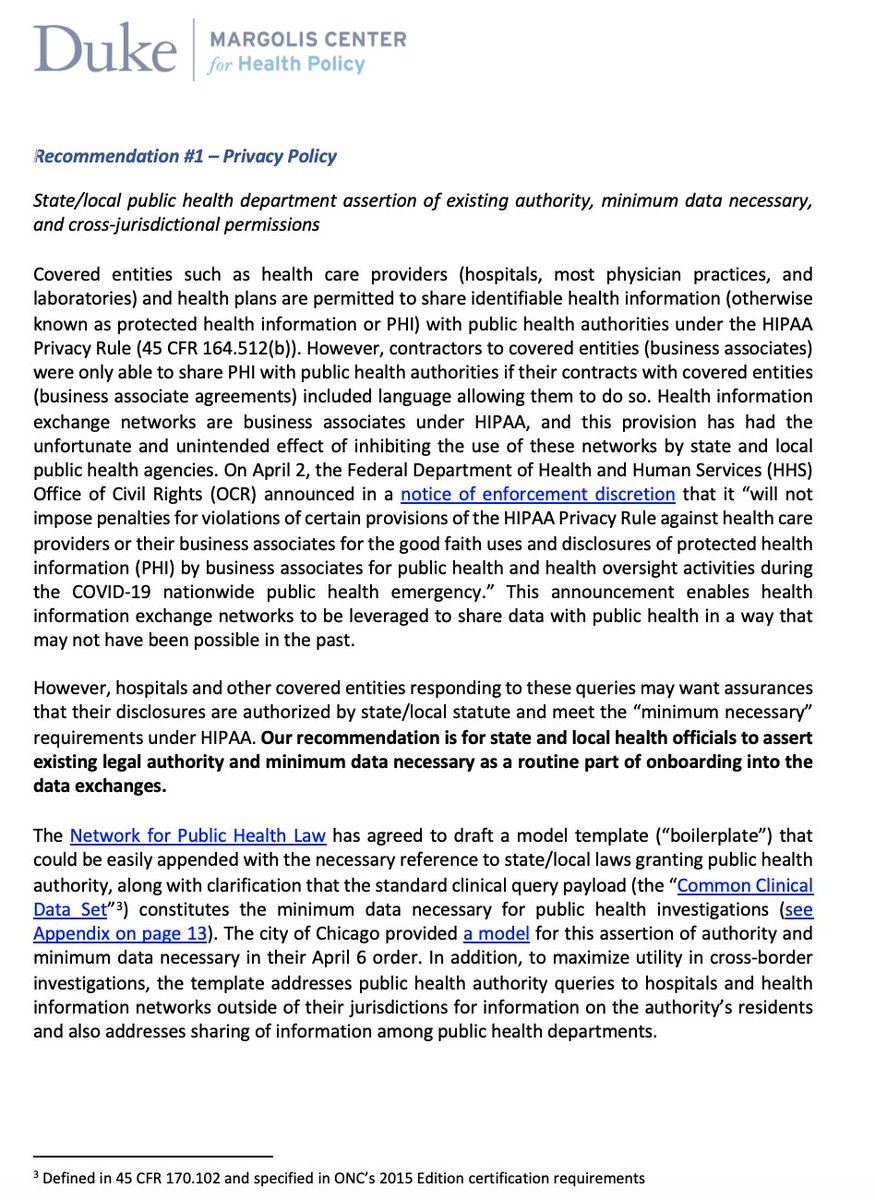
20/ Rather than wait and hope for a national authority to represent all of public health in making this assertion, we recommended that each health department assert this when they are onboarding onto the data exchanges
And @HealthPrivacy @networkforphl went ahead and drafted it!
And @HealthPrivacy @networkforphl went ahead and drafted it!
21/ We talked with the executive directors of the 3 major exchanges
@CommonWell @paul_wilder
@CarequalityNet Dave Cassel
@eHealthExchange Jay Nakashima
..and they all committed to putting public health on an equal footing to treatment queries- ensure universal responses 👏👏
@CommonWell @paul_wilder
@CarequalityNet Dave Cassel
@eHealthExchange Jay Nakashima
..and they all committed to putting public health on an equal footing to treatment queries- ensure universal responses 👏👏
22/ We needed someone to step up who could provide health departments with the technical means to access these networks right now- security, onboarding, tools, the works.
After investigating we found two great organizations who could do it: @healthgorilla and @A_INQ
For free.
After investigating we found two great organizations who could do it: @healthgorilla and @A_INQ
For free.
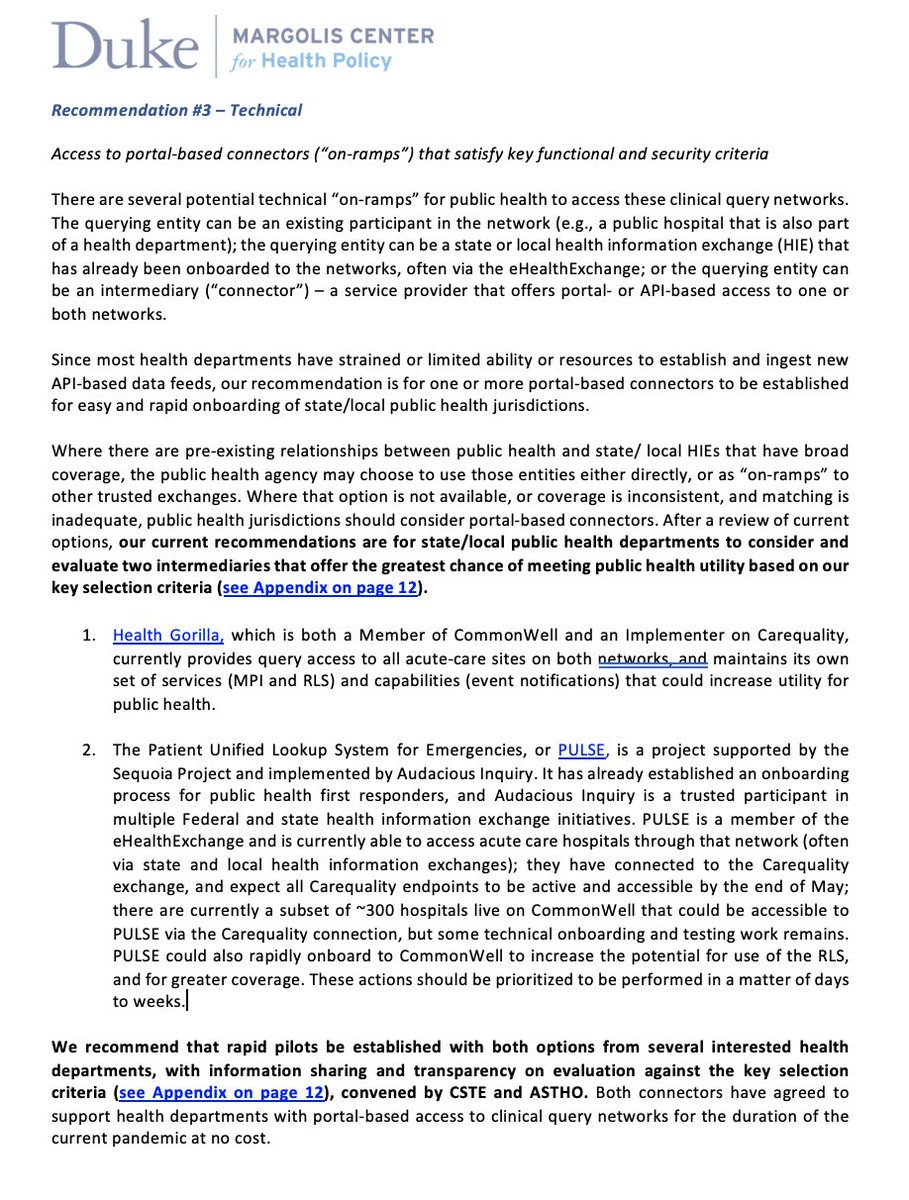
23/ So we will move ahead- with help from @CSTEnews & @ASTHO- testing both options as soon as possible
There are health departments already interested and willing to move ahead
@networkforphl agreed to help draft legal agreements
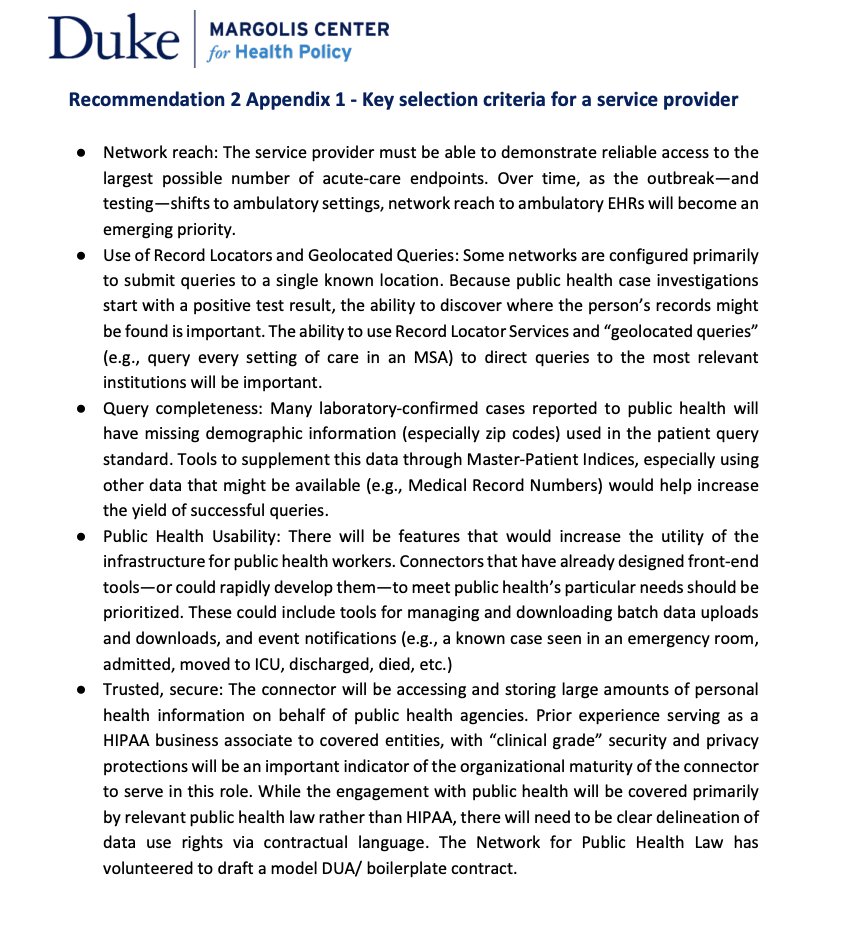
We drafted a useful set of evaluation criteria
There are health departments already interested and willing to move ahead
@networkforphl agreed to help draft legal agreements
We drafted a useful set of evaluation criteria
24/ This is really exciting, guys!
If you are a health department who's struggling to get clinical records as part of your COVID case investigations, this could be a game-changer.
Not 9 months from now.
Next week.
Reach out to @CSTEnews (Association of State Epidemiologists)
If you are a health department who's struggling to get clinical records as part of your COVID case investigations, this could be a game-changer.
Not 9 months from now.
Next week.
Reach out to @CSTEnews (Association of State Epidemiologists)
25/ Could @CDCgov have done this?
Could they make assertion of public health need & minimum data necessary?
Could they use their convening power to get governance entities onboard?
Could they use CARES Act $500M to contract for these services?
I don't know. But we can't wait
Could they make assertion of public health need & minimum data necessary?
Could they use their convening power to get governance entities onboard?
Could they use CARES Act $500M to contract for these services?
I don't know. But we can't wait
26/ The final area of opportunity (phew!) was Syndromic Surveillance of ED visits for COVID-like symptoms.
It's become more central to fighting this outbreak than I could have imagined 20 years ago.
But we aren't using it well enough, or transparently
It's become more central to fighting this outbreak than I could have imagined 20 years ago.
But we aren't using it well enough, or transparently
27/ We're using syndromic trends to reopen, and may use them to tighten back up.
But unlike case counts, hospitals, deaths, there's no public daily reporting of what's happening in each state, even though WE HAVE THE DATA ALREADY
We don't need new systems-we can fix this one
But unlike case counts, hospitals, deaths, there's no public daily reporting of what's happening in each state, even though WE HAVE THE DATA ALREADY
We don't need new systems-we can fix this one
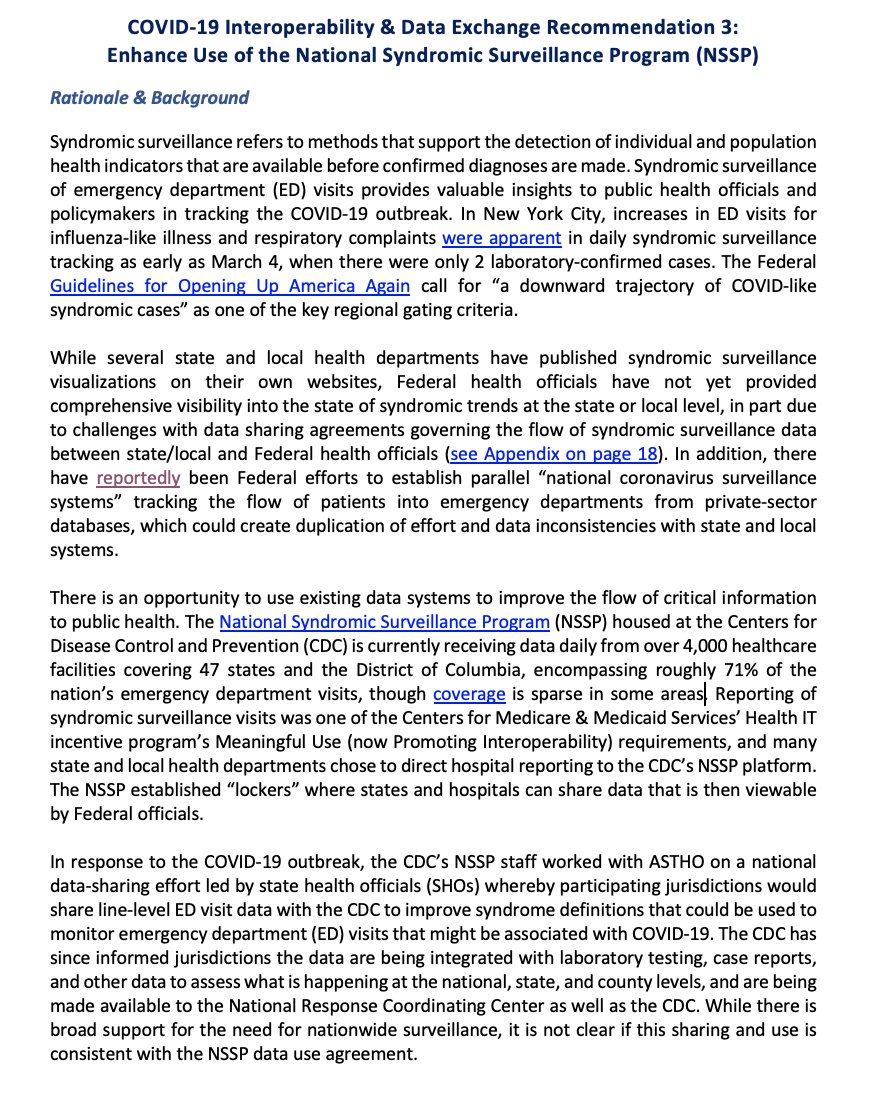
28/ We can make it not just more transparent, but also more complete. There are states that have been reluctant to participate because they aren't sure how the feds will use their data.
Louisiana hadn't seen this slide before it was used in a WH briefing. That can't happen again
Louisiana hadn't seen this slide before it was used in a WH briefing. That can't happen again

29/ We can also make the data more meaningful
Some states are also getting data on whether the ER visit led to a hospitalization. That's incredibly helpful in trying to figure out if the decrease in ED visits is just due to people afraid to go to the ED
See inflection pt in NYC
Some states are also getting data on whether the ER visit led to a hospitalization. That's incredibly helpful in trying to figure out if the decrease in ED visits is just due to people afraid to go to the ED
See inflection pt in NYC

30/ How do we do it?
Do we tell every hospital to go back and fix their data quality within the existing spec?
We talked to some implementers in the field who said, just tell em to turn on the inpatient feed also- much easier and faster- especially in the current environment👍
Do we tell every hospital to go back and fix their data quality within the existing spec?
We talked to some implementers in the field who said, just tell em to turn on the inpatient feed also- much easier and faster- especially in the current environment👍

31/ that's it.
2 dozen experts, 2 weeks, 3 sets of recommendations
This happened in 7.30 pm calls after our regular jobs, giving up weekends, in a busy time for everyone; but no one complained, no one shirked the call to service- and the work continues
we can do things 🇺🇸
2 dozen experts, 2 weeks, 3 sets of recommendations
This happened in 7.30 pm calls after our regular jobs, giving up weekends, in a busy time for everyone; but no one complained, no one shirked the call to service- and the work continues
we can do things 🇺🇸

