2/
Data limitations
- most lab confirmed cases were from hospital deaths - most severe cases?
- the case definition/testing of COVID-19 changed through the pandemic
- ethnicity matched from 2011 census
- lack of data on vulnerable groups: migrants, sex workers, homelessness
Data limitations
- most lab confirmed cases were from hospital deaths - most severe cases?
- the case definition/testing of COVID-19 changed through the pandemic
- ethnicity matched from 2011 census
- lack of data on vulnerable groups: migrants, sex workers, homelessness
3/
Appraisal
- no discussion/action plan
- lessons learnt due to led by Equalities Minister (@KemiBadenoch) who had never heard of @MichaelMarmot's @TheMarmotReview until mentioned in Parliament yesterday:
- I’m worried very little will change
Appraisal
- no discussion/action plan
- lessons learnt due to led by Equalities Minister (@KemiBadenoch) who had never heard of @MichaelMarmot's @TheMarmotReview until mentioned in Parliament yesterday:
- I’m worried very little will change
4/
@TheMarmotReview found that UK life expectancy is slowing down with widening inequalities in societies between rich and poor. This was associated with cuts to public spending over the last 2 decades.
🔗:
@TheMarmotReview found that UK life expectancy is slowing down with widening inequalities in societies between rich and poor. This was associated with cuts to public spending over the last 2 decades.
🔗:
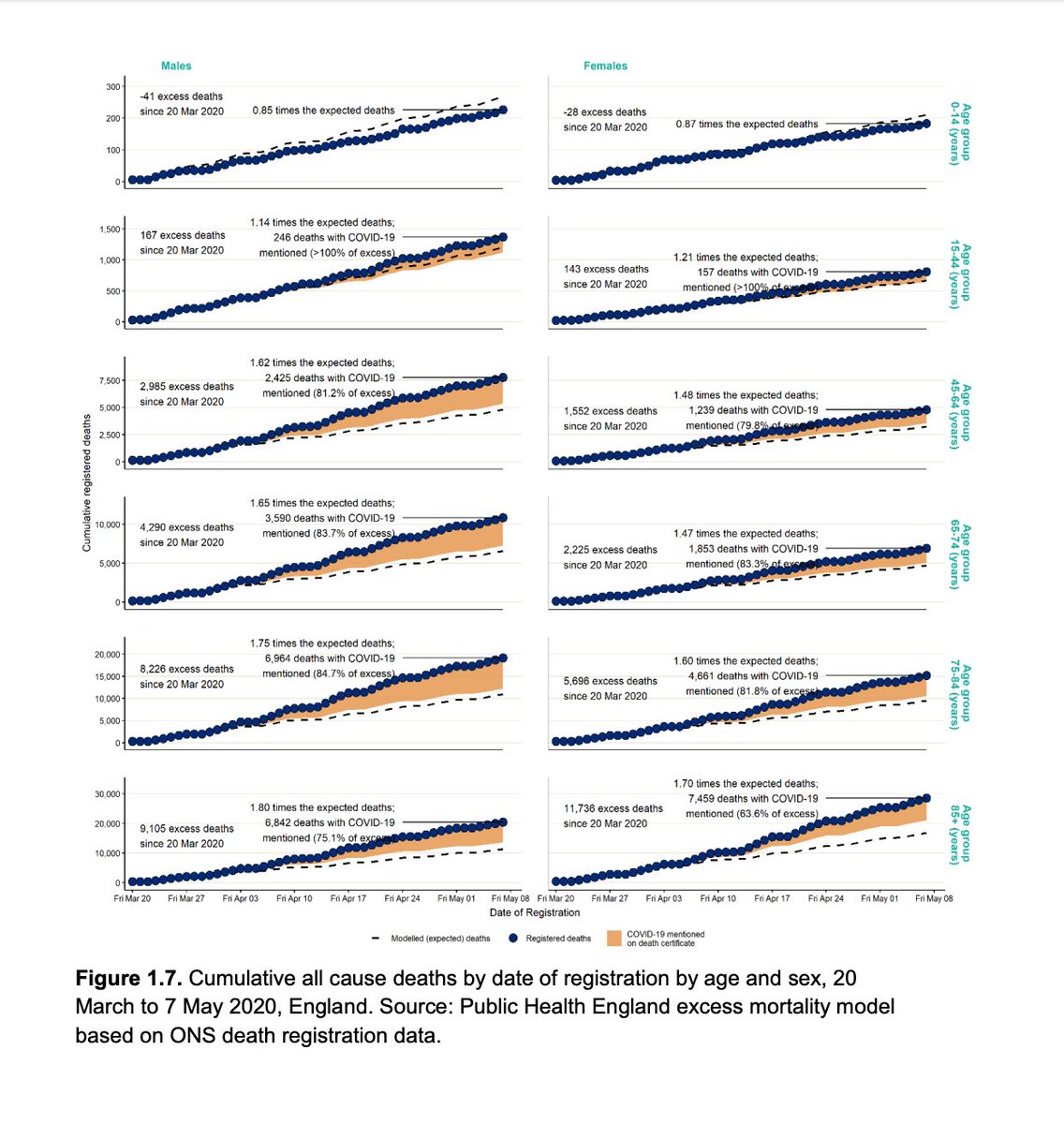
5/ Age
Women < age 60, Men > age 60 more likely to die. Why use 60 years?
≥ 80 year old, 70x increased likelihood of death compared to those < 40 years old
Most excess deaths (75%) in ≥ 75 years
Fewer deaths than expected in children under 15 years of age
Women < age 60, Men > age 60 more likely to die. Why use 60 years?
≥ 80 year old, 70x increased likelihood of death compared to those < 40 years old
Most excess deaths (75%) in ≥ 75 years
Fewer deaths than expected in children under 15 years of age

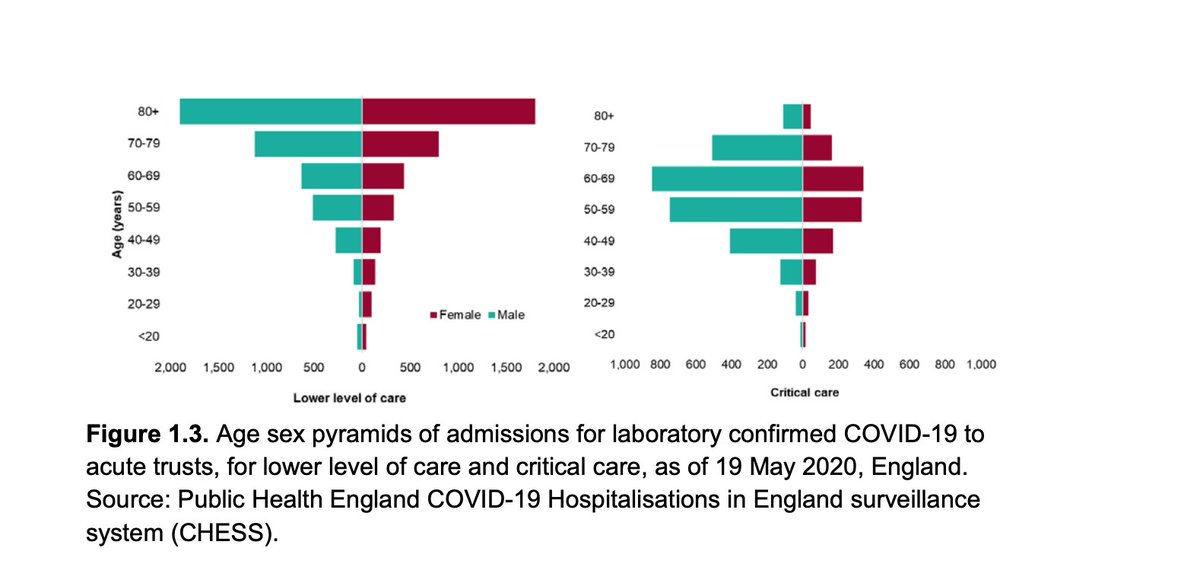
6a/ Sex/Age
Men more at risk 46% cases, 60% deaths, 70% ITU admissions.
More female cases compared to male cases.
Men - higher clinical (not testing) diagnosis rates > age 60
Men more at risk 46% cases, 60% deaths, 70% ITU admissions.
More female cases compared to male cases.
Men - higher clinical (not testing) diagnosis rates > age 60

6b/ Sex/Age
Women - higher testing diagnosis rate for many age groups 0-59 and >80
Women - higher testing diagnosis rate for many age groups 0-59 and >80

6c/ Sex/Age
Men more likely to be admitted to hospital and critical care.
Men more likely to be admitted to hospital and critical care.
6d/ Sex/Age
Men more likely to die 1.3-2.1 x compared to women over all age groups.
Men more likely to die 1.3-2.1 x compared to women over all age groups.

6e/ Age/Sex
More excess deaths in all age groups except in < 15 years age group
#COVIDー19 pushed the age standardised mortality rate up for men > women
More excess deaths in all age groups except in < 15 years age group
#COVIDー19 pushed the age standardised mortality rate up for men > women
6f/ Age/Sex
Is the data valid?
Similar to Chinese data: thelancet.com/journals/lance…
Similar to other international data but 90% Chinese studies (systematic review): medrxiv.org/content/10.110…
Is the data valid?
Similar to Chinese data: thelancet.com/journals/lance…
Similar to other international data but 90% Chinese studies (systematic review): medrxiv.org/content/10.110…
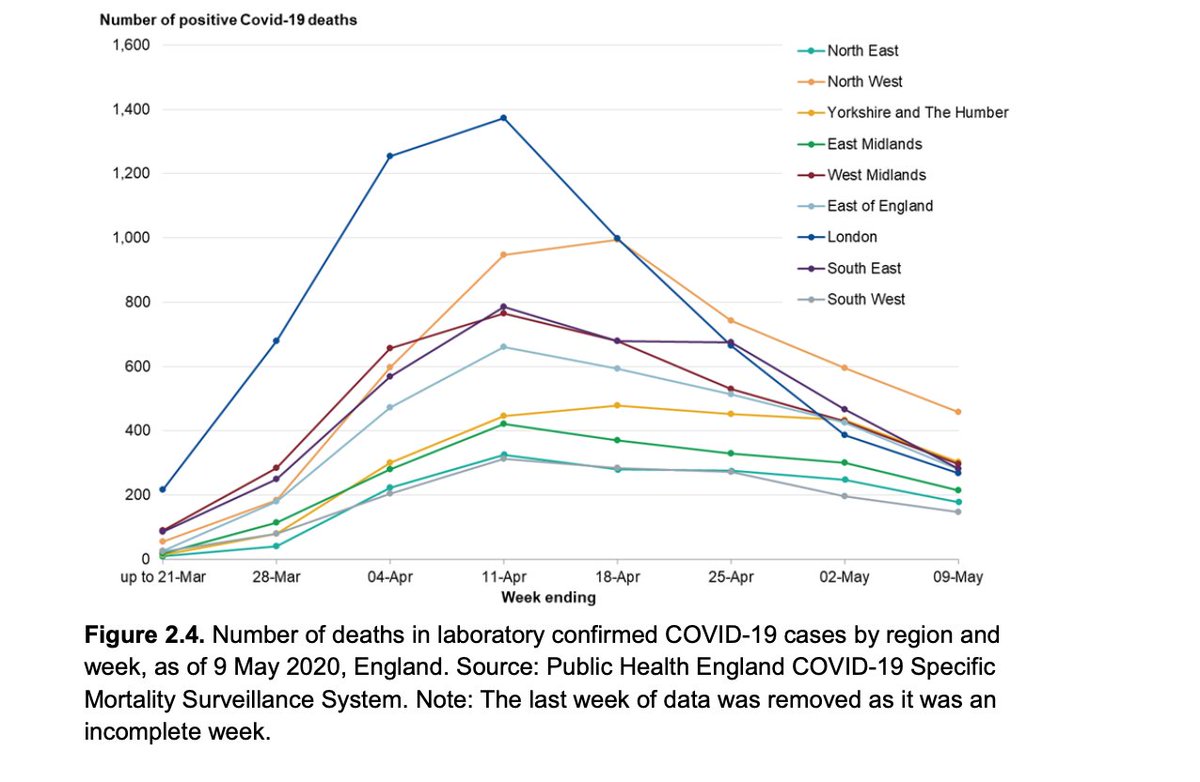
7a/ Geography
Highest death rates in London then NorthWest, NorthEast then West Midlands.
London death rate 3x than the lowest rates in SW
Urban > rural positive case rates
Number of positive cases decreasing but NW have highest number of positive cases on 9th May
Highest death rates in London then NorthWest, NorthEast then West Midlands.
London death rate 3x than the lowest rates in SW
Urban > rural positive case rates
Number of positive cases decreasing but NW have highest number of positive cases on 9th May

7b/ Geography
Highest infection rate for men in London and highest for women in NorthWest as of 13 May.
Highest infection rate for men in London and highest for women in NorthWest as of 13 May.

7c/ Geography
Hospitalisations for all regions are down but a recent up tick in some regions
Hospitalisations for all regions are down but a recent up tick in some regions

7d/ Geography
Number of #COVIDー19 positive deaths are decreasing but currently highest in Yorkshire and Humber where London was highest at peak
Number of #COVIDー19 positive deaths are decreasing but currently highest in Yorkshire and Humber where London was highest at peak
7e/ Geography
"death rates were highly clustered. Authorities, which are largely urban areas, in London, the NW, the W Midlands and the NE had the highest death rates.
For males, the eight authorities with the highest death rates among confirmed cases are in London.
"death rates were highly clustered. Authorities, which are largely urban areas, in London, the NW, the W Midlands and the NE had the highest death rates.
For males, the eight authorities with the highest death rates among confirmed cases are in London.

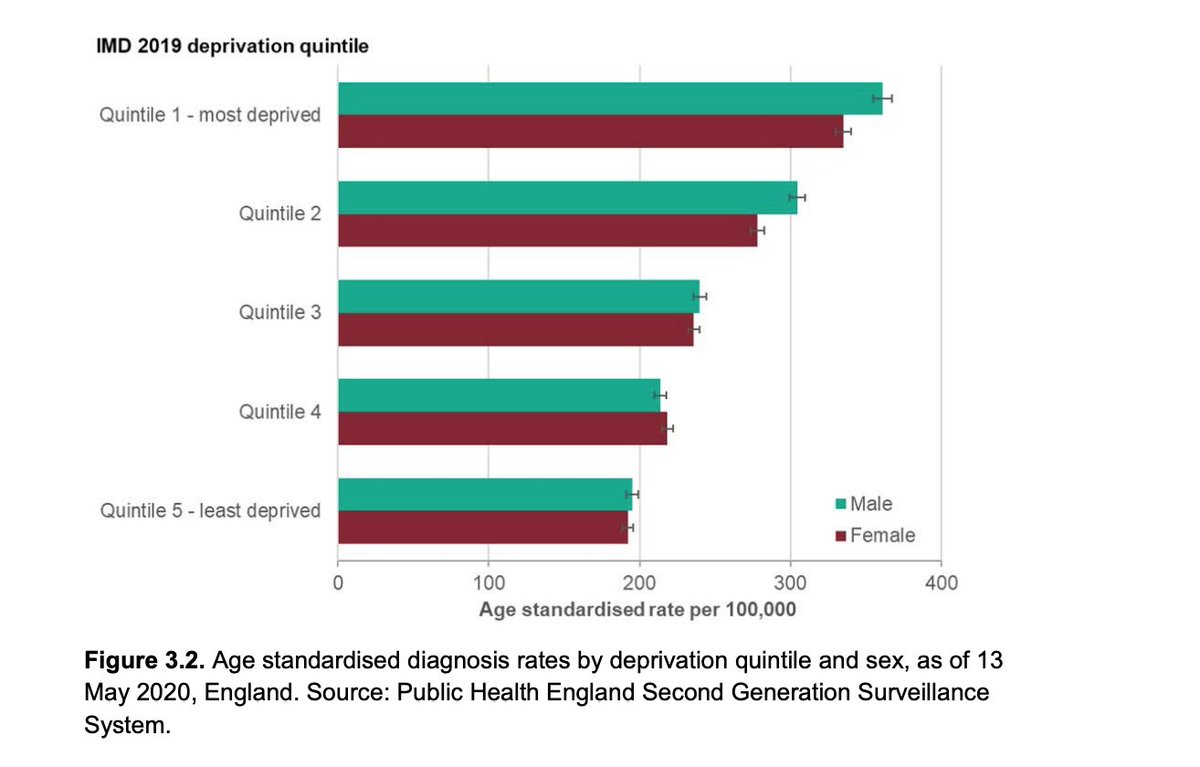
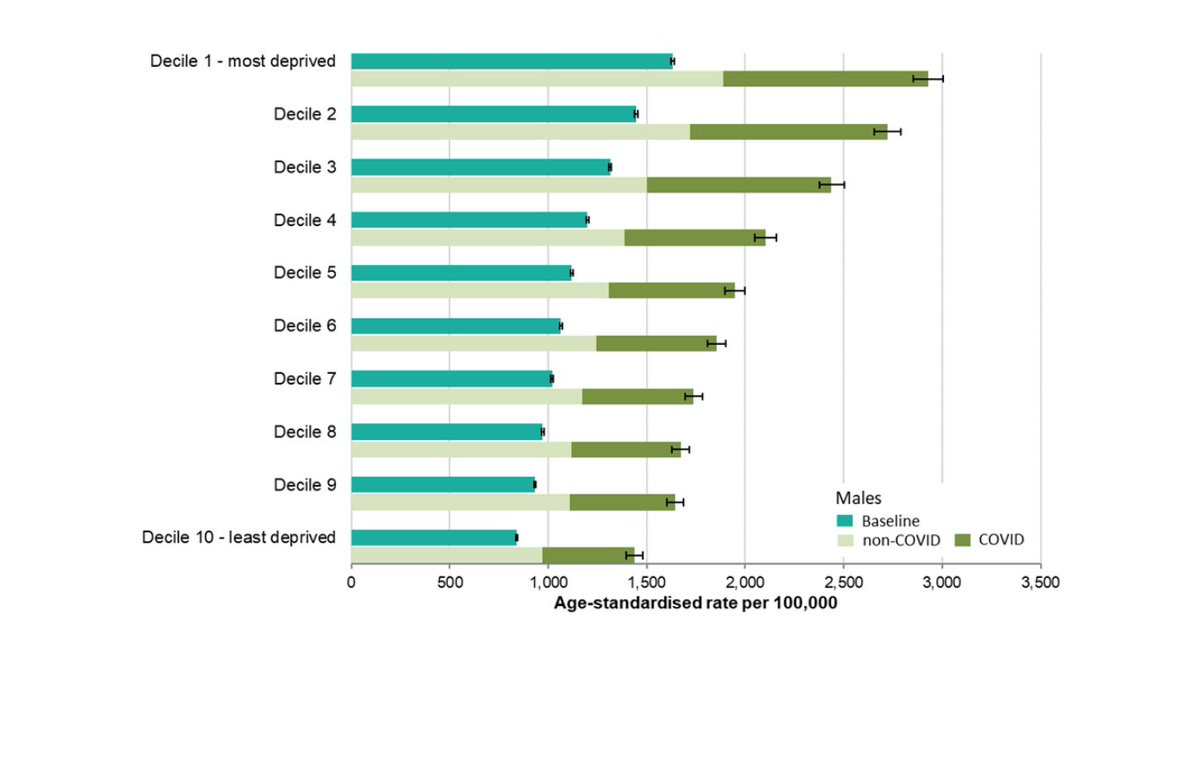
8a/ Deprivation
2x mortality rates in men and women comparing most deprived vs least deprived areas even when controlling for ethnicity
Unable to comment on underlying health conditions
2x mortality rates in men and women comparing most deprived vs least deprived areas even when controlling for ethnicity
Unable to comment on underlying health conditions
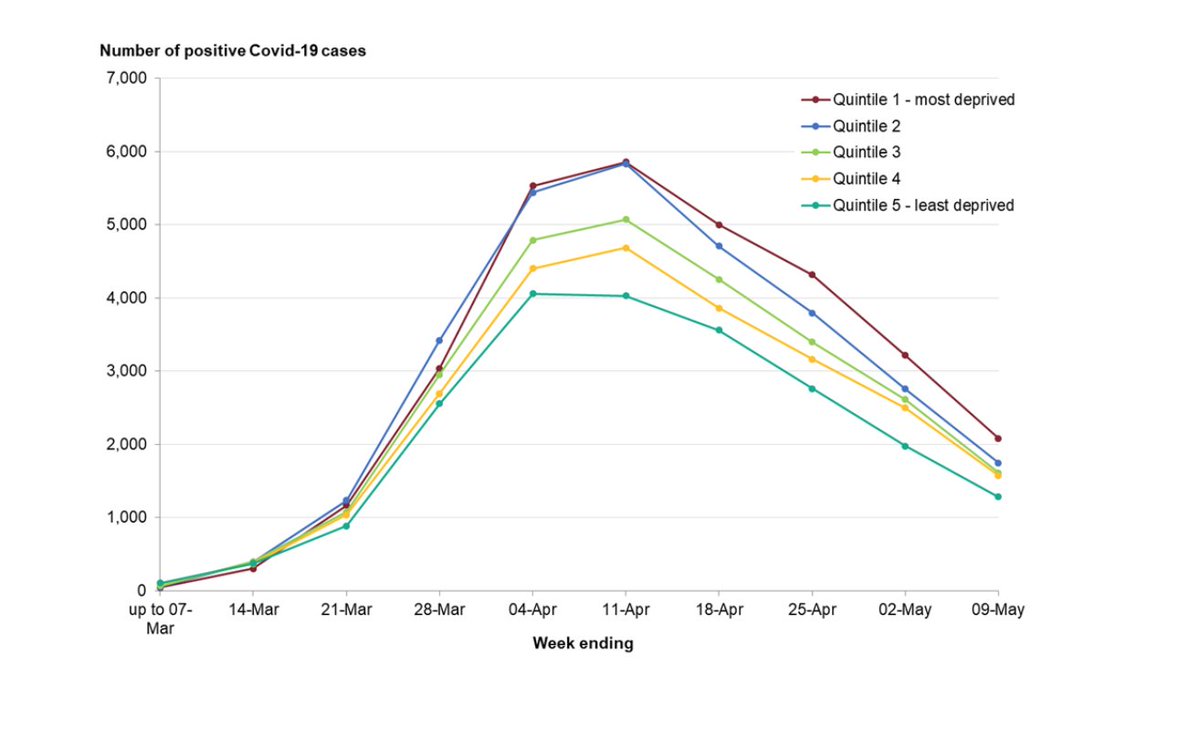
8b/ Deprivation
High diagnosis rates may be due to geographic proximity to infections/high proportion of workers in occupations that are more likely to be exposed.
#COVIDー19 is NOT the great equaliser.
More cases overall/both sexes in more deprived vs less deprived
High diagnosis rates may be due to geographic proximity to infections/high proportion of workers in occupations that are more likely to be exposed.
#COVIDー19 is NOT the great equaliser.
More cases overall/both sexes in more deprived vs less deprived



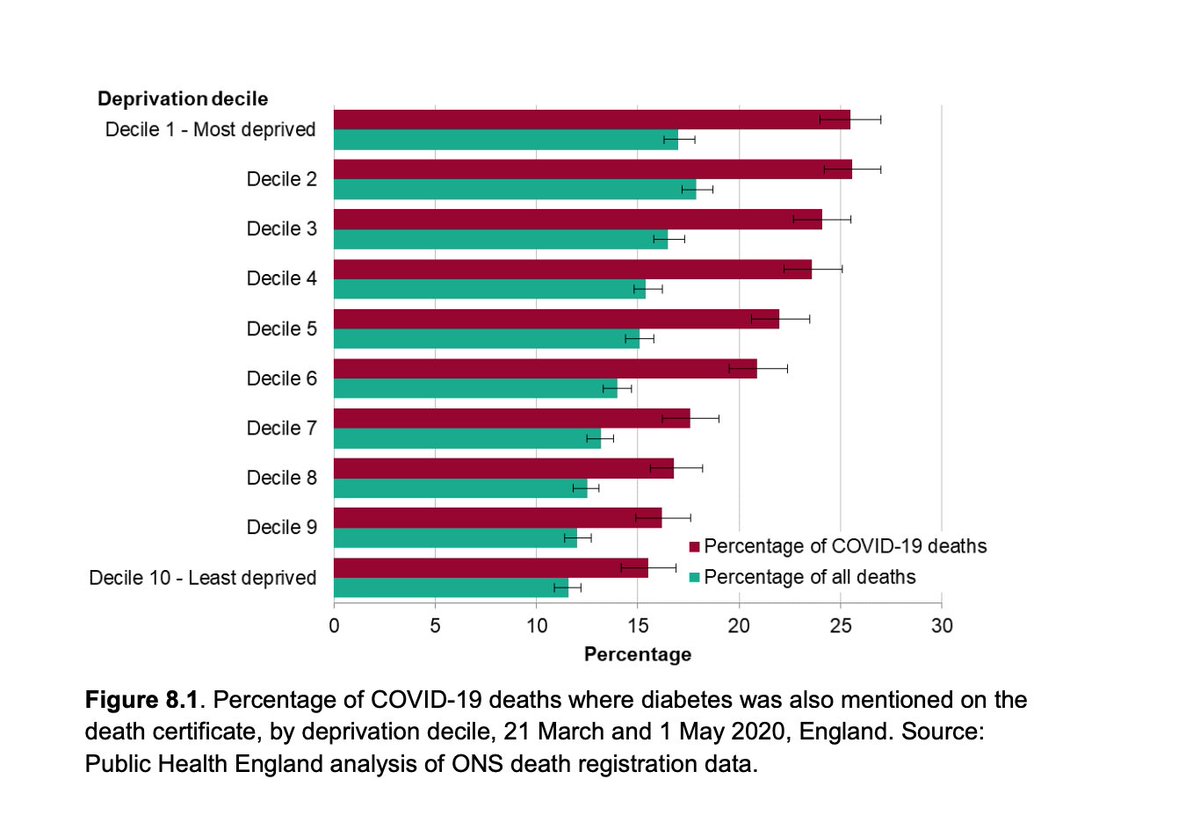
8e/ Deprivation
There are higher #COVIDー19 deaths where diabetes is mentioned on death certificates in people from most deprived backgrounds compared to least deprived backgrounds
There are higher #COVIDー19 deaths where diabetes is mentioned on death certificates in people from most deprived backgrounds compared to least deprived backgrounds
9a/ Ethnicity
People of Bangladeshi ethnicity had 2x mortality risk compared to people of White British ethnicity.
People of Chinese, Indian, Pakistani, Other Asian, Caribbean and Other Black ethnicity had 10-50% higher mortality risk compared to White British.
People of Bangladeshi ethnicity had 2x mortality risk compared to people of White British ethnicity.
People of Chinese, Indian, Pakistani, Other Asian, Caribbean and Other Black ethnicity had 10-50% higher mortality risk compared to White British.
9b/ Ethnicity
No data about occupation.
Suggested causes, more likely to:
➡️ live in overcrowded conditions
➡️ live in urban areas
➡️ live in deprived ares
➡️ have jobs that expose them to higher risk
➡️ be born abroad - culture/language
➡️ have more health conditions
No data about occupation.
Suggested causes, more likely to:
➡️ live in overcrowded conditions
➡️ live in urban areas
➡️ live in deprived ares
➡️ have jobs that expose them to higher risk
➡️ be born abroad - culture/language
➡️ have more health conditions
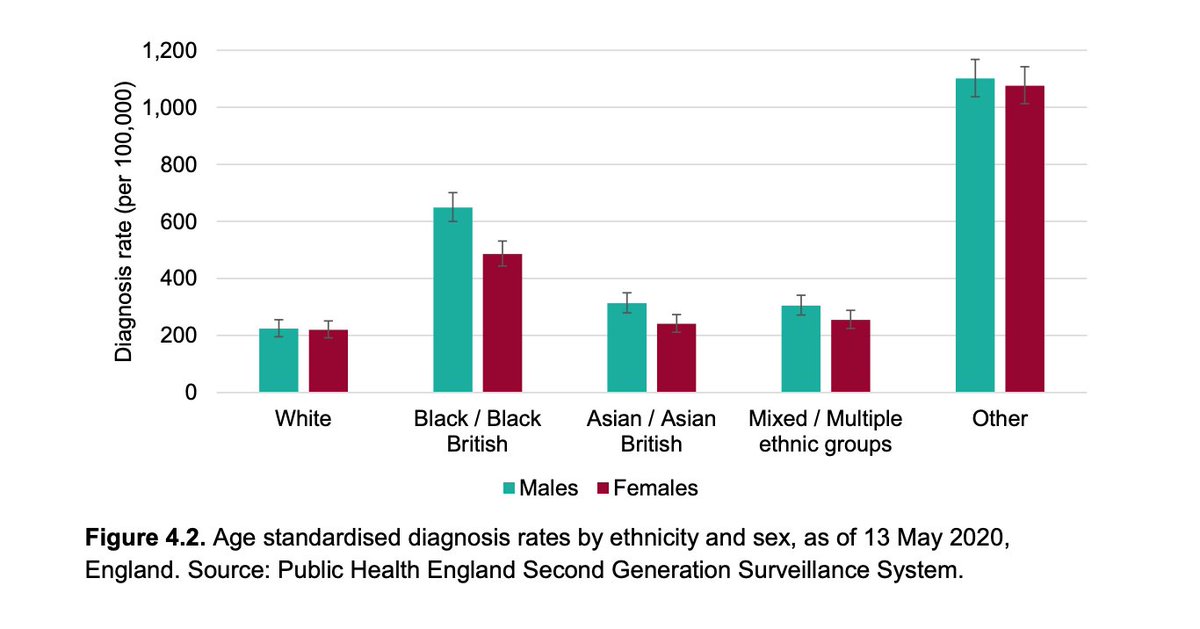
9c/ Ethnicity
People from ethnic minority backgrounds are more likely to be diagnosed with #COVIDー19 compared to white British people.
People from ethnic minority backgrounds are more likely to be diagnosed with #COVIDー19 compared to white British people.
9d/ Ethnicity
People from ethnic minority background (black and minority ethnic, BAME) more likely to be admitted to ITU compared to white British people
People from ethnic minority background (black and minority ethnic, BAME) more likely to be admitted to ITU compared to white British people

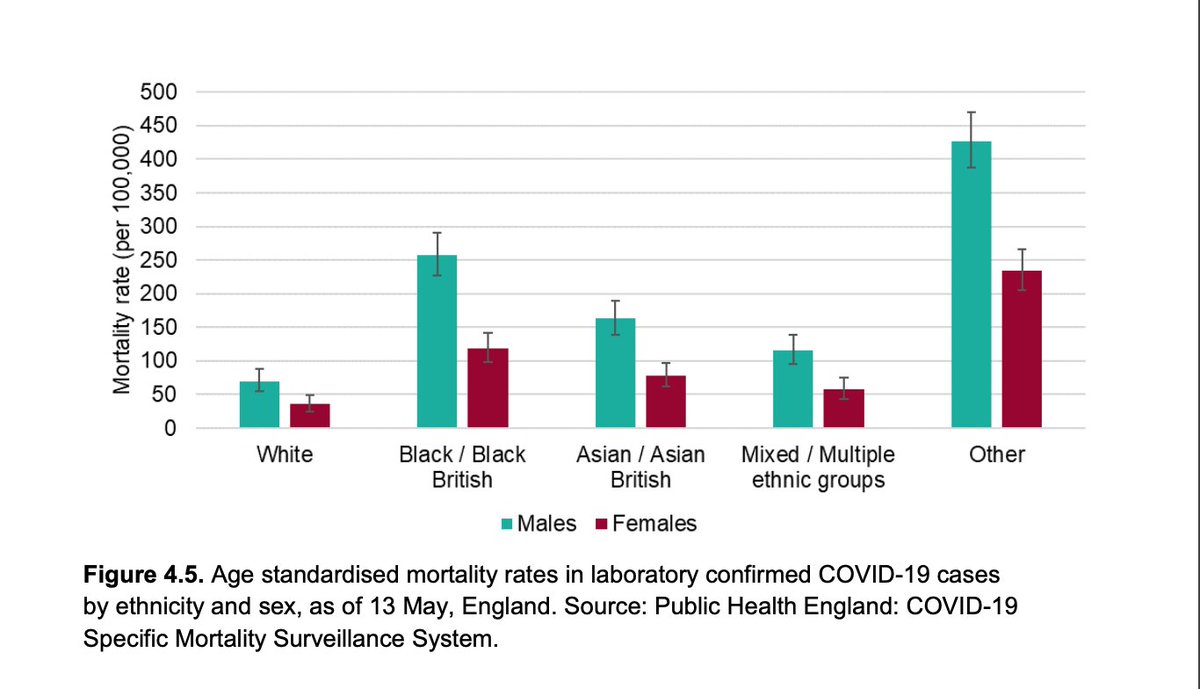
9e/ Ethnicity
People from ethnic minority background (black and minority ethnic, BAME) more likely to die from #COVIDー19 compared to white British People.
People from ethnic minority background (black and minority ethnic, BAME) more likely to die from #COVIDー19 compared to white British People.
9f/ Ethnicity
Higher all cause mortality in BAME compared to white people
All cause mortality was higher in all groups but
Black British people: 3 - 4 times higher
Asian people: 2.4 - 3 times higher
White people: 1.6 - 2 times higher
Higher all cause mortality in BAME compared to white people
All cause mortality was higher in all groups but
Black British people: 3 - 4 times higher
Asian people: 2.4 - 3 times higher
White people: 1.6 - 2 times higher

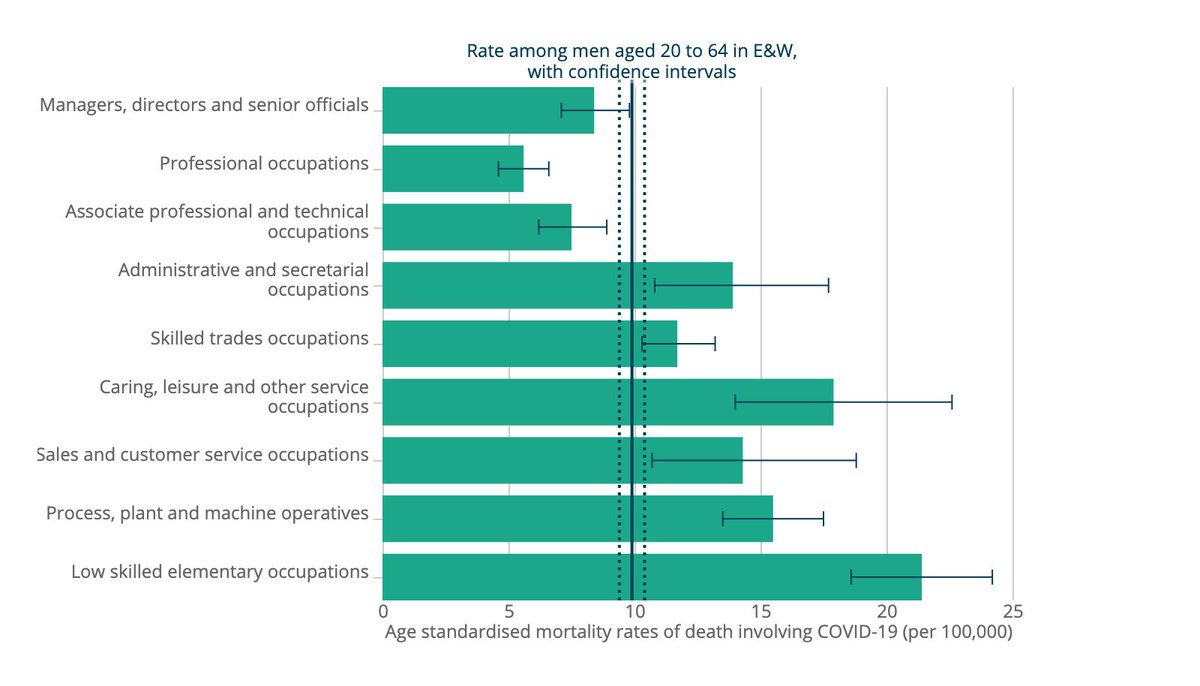
10b/ Occupation
Highest #COVIDー19 mortality rate for men working as:
security guards
taxi drivers and chauffeurs
bus and coach drivers
chefs
sales and retail assistants
lower skilled workers in construction and processing plants
AND men and women working in social care
Highest #COVIDー19 mortality rate for men working as:
security guards
taxi drivers and chauffeurs
bus and coach drivers
chefs
sales and retail assistants
lower skilled workers in construction and processing plants
AND men and women working in social care
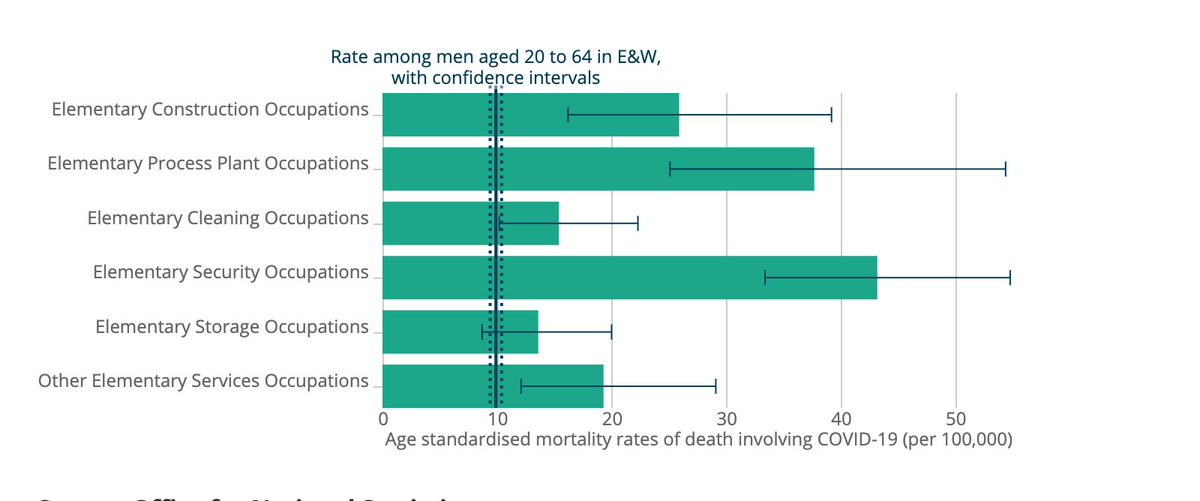
10c/ Occupation
Highest #COVIDー19 mortality rate amongst security workers in 'lower-skilled'* workers group.
*this is the term used in the report. These are the people that allow our countries to run. Should be 'essential'
Highest #COVIDー19 mortality rate amongst security workers in 'lower-skilled'* workers group.
*this is the term used in the report. These are the people that allow our countries to run. Should be 'essential'
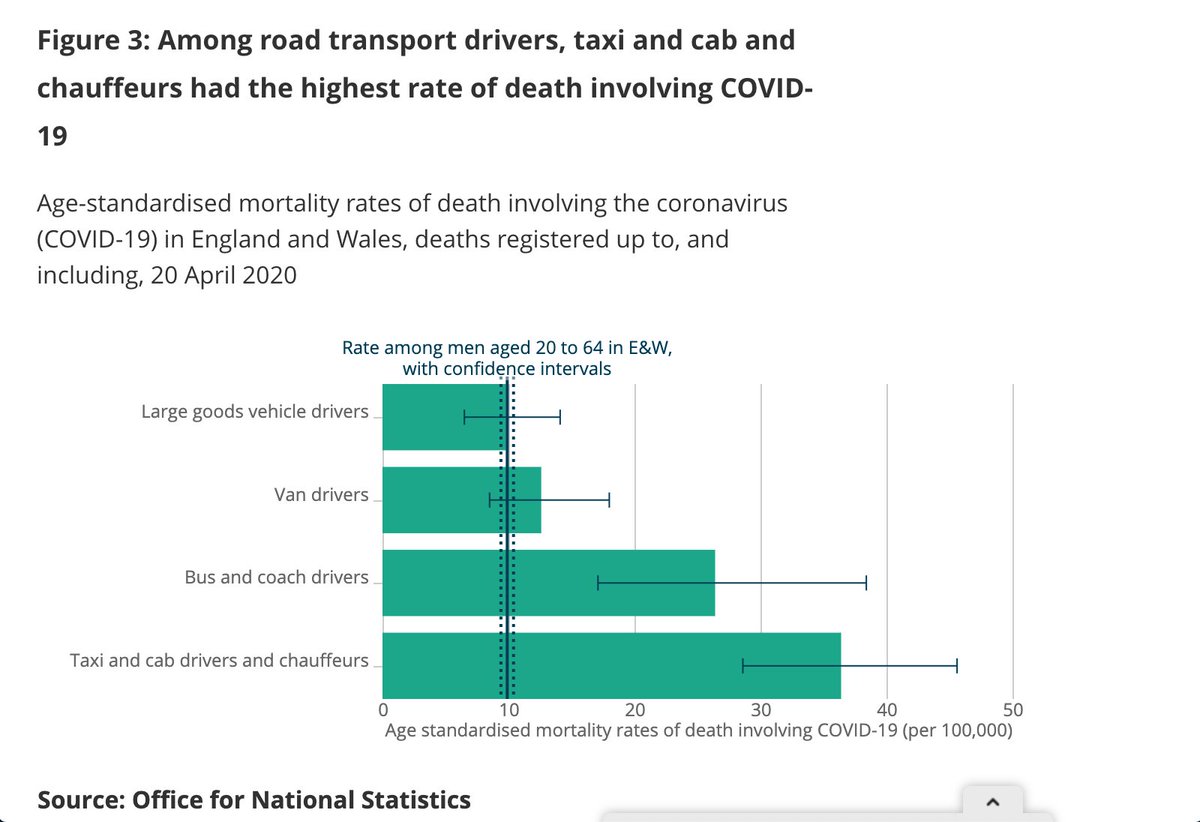
10d/ Occupation
Highest #COVIDー19 mortality rate for taxi drivers compared to all other drivers. This is probably due to the close contact involved in the job.
Highest #COVIDー19 mortality rate for taxi drivers compared to all other drivers. This is probably due to the close contact involved in the job.



11a/ Inclusion Health Groups
Migrants from Africa, Middle East, Caribbean at higher risk compared to migrants from UK/EU:
- 1-2%: absolute risk increase
- 50-100%: relative risk increase
Migrants from Africa, Middle East, Caribbean at higher risk compared to migrants from UK/EU:
- 1-2%: absolute risk increase
- 50-100%: relative risk increase

11b/ Inclusion Health Groups
No data on deaths in homeless populations
No data on deaths in homeless populations

13a/ Co-morbidities
Looking at death certification, diabetes mentioned on 21% of all death certificates.
This proportion higher in ethnic minority groups vs British white people.
Data awaited on body mass index and other co-morbidities for detailed analysis
Looking at death certification, diabetes mentioned on 21% of all death certificates.
This proportion higher in ethnic minority groups vs British white people.
Data awaited on body mass index and other co-morbidities for detailed analysis
13b/ Co-morbidities
Most at risk:
➡️ Cardiovascular disease: high blood pressure, heart disease
➡️ Chronic Kidney disease
➡️ Respiratory (lung) conditions: COPD
➡️ Diabetes
Most at risk:
➡️ Cardiovascular disease: high blood pressure, heart disease
➡️ Chronic Kidney disease
➡️ Respiratory (lung) conditions: COPD
➡️ Diabetes

<< ENDS >>
@threadreaderapp unroll please
@threadreaderapp unroll please