Age: 14-year old female
History: Proptosis & pain
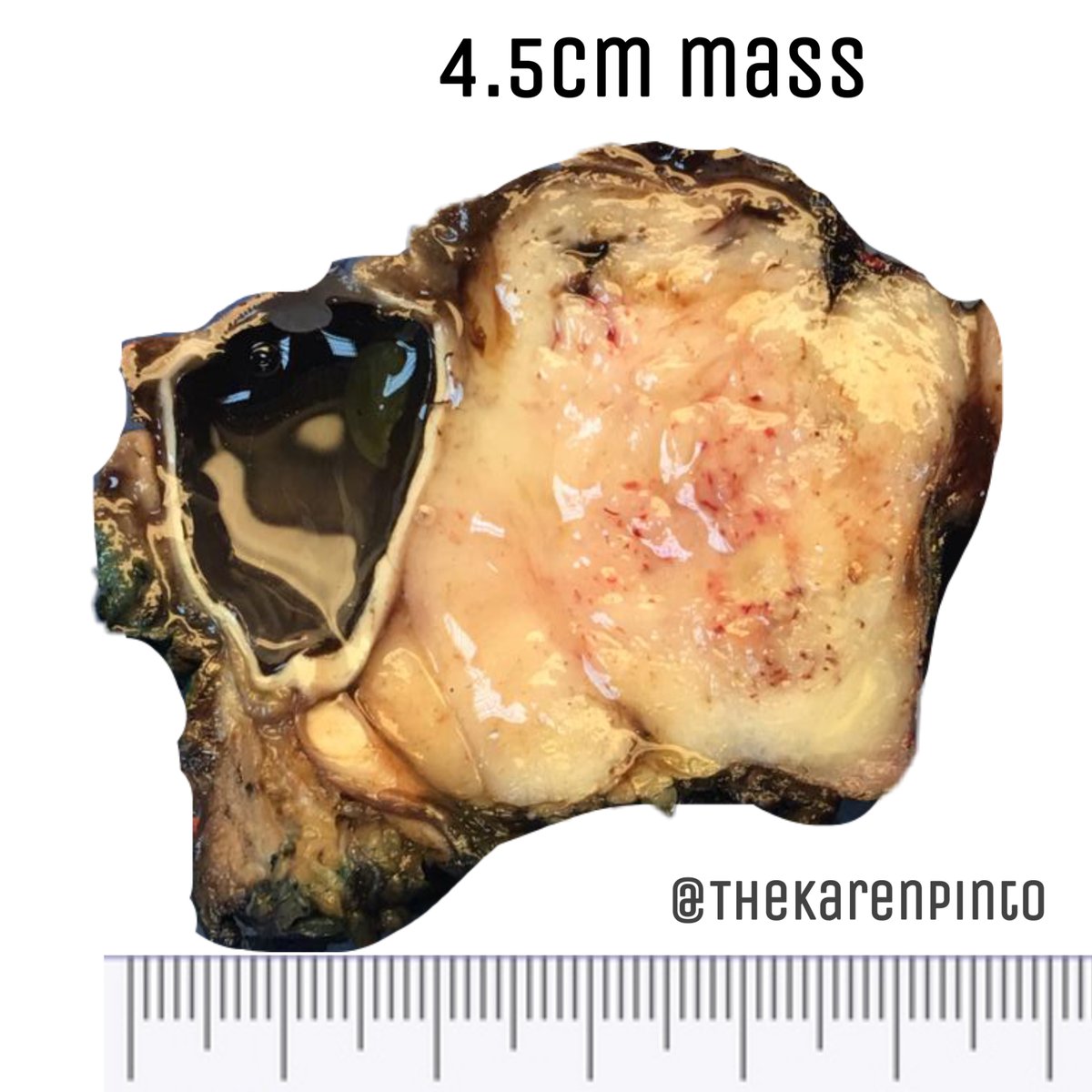
Specimen: Exenteration
#pathology #PediPath #BSTPath #orbit
(*Image courtesy: Dr. Sayed Hashim)
History: Proptosis & pain
Specimen: Exenteration
#pathology #PediPath #BSTPath #orbit
(*Image courtesy: Dr. Sayed Hashim)

3 main questions:
Q1. Is it benign or malignant?
Q1. Is it benign or malignant?
Q2. If malignant - differentials?
DDx of orbital tumors in children:
1. Rhabdomyosarcoma (RMS)
2. Neuroblastoma
3. Synovial sarcoma
4. Chloroma
& so on
DDx of orbital tumors in children:
1. Rhabdomyosarcoma (RMS)
2. Neuroblastoma
3. Synovial sarcoma
4. Chloroma
& so on
Q3. Has it been excised completely / margin status?
A3. Tumor reaches the inked margin
(there is probably microscopic residual disease)
(*Important for assigning the correct RMS Clinical Group- explained later on)
A3. Tumor reaches the inked margin
(there is probably microscopic residual disease)
(*Important for assigning the correct RMS Clinical Group- explained later on)

What is the distance for adequate resections margins in such tumors?
2.0-3.0cm of normal tissue is considered an adequate margin
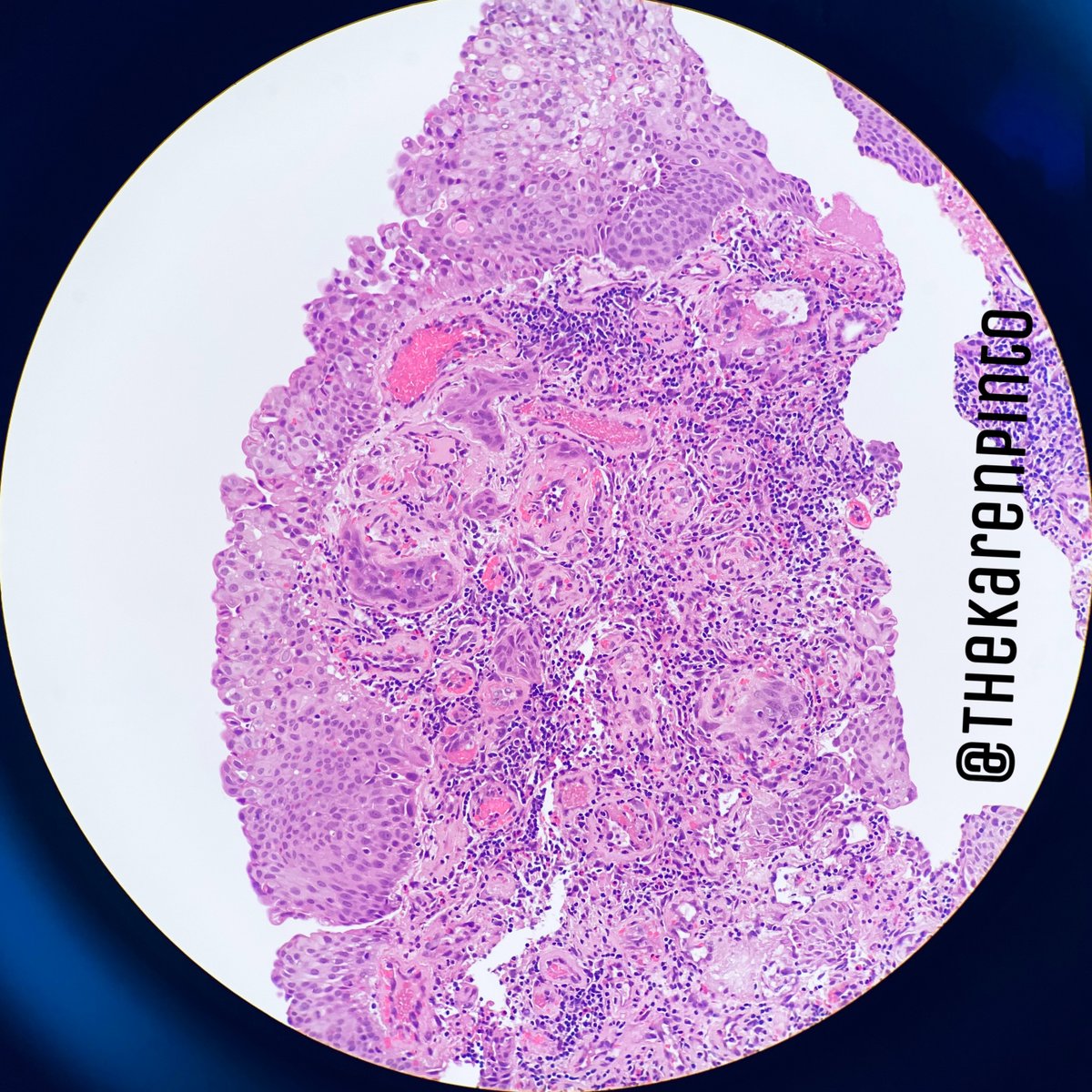
Microscopy (low power):
1. Hyper & hypocellular areas
2. Myxoid stroma
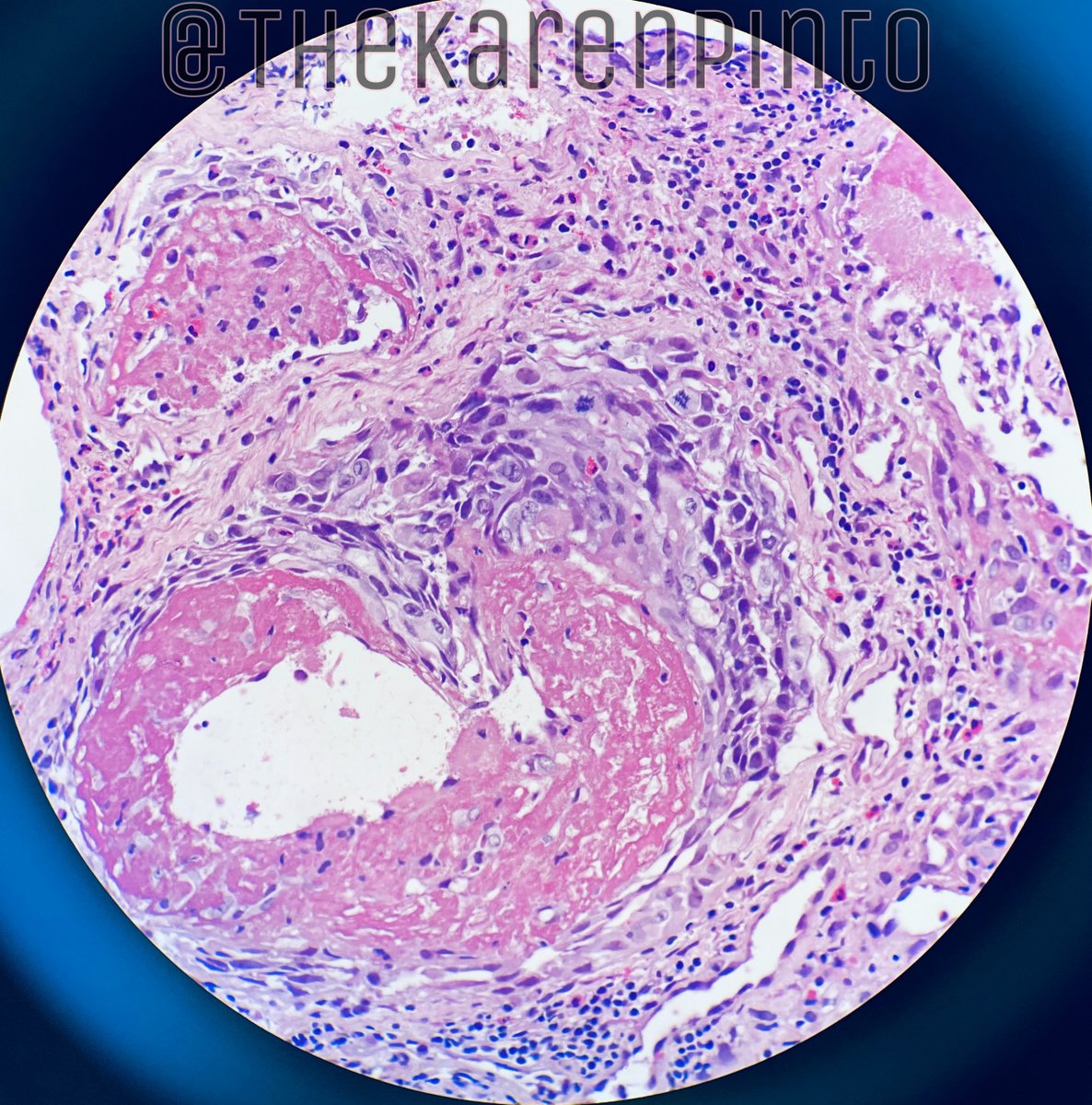
3. Lots of necrosis
4. Primitive looking cells of varying sizes (so unlikely to be a translocation related tumor)
1. Hyper & hypocellular areas
2. Myxoid stroma
3. Lots of necrosis
4. Primitive looking cells of varying sizes (so unlikely to be a translocation related tumor)




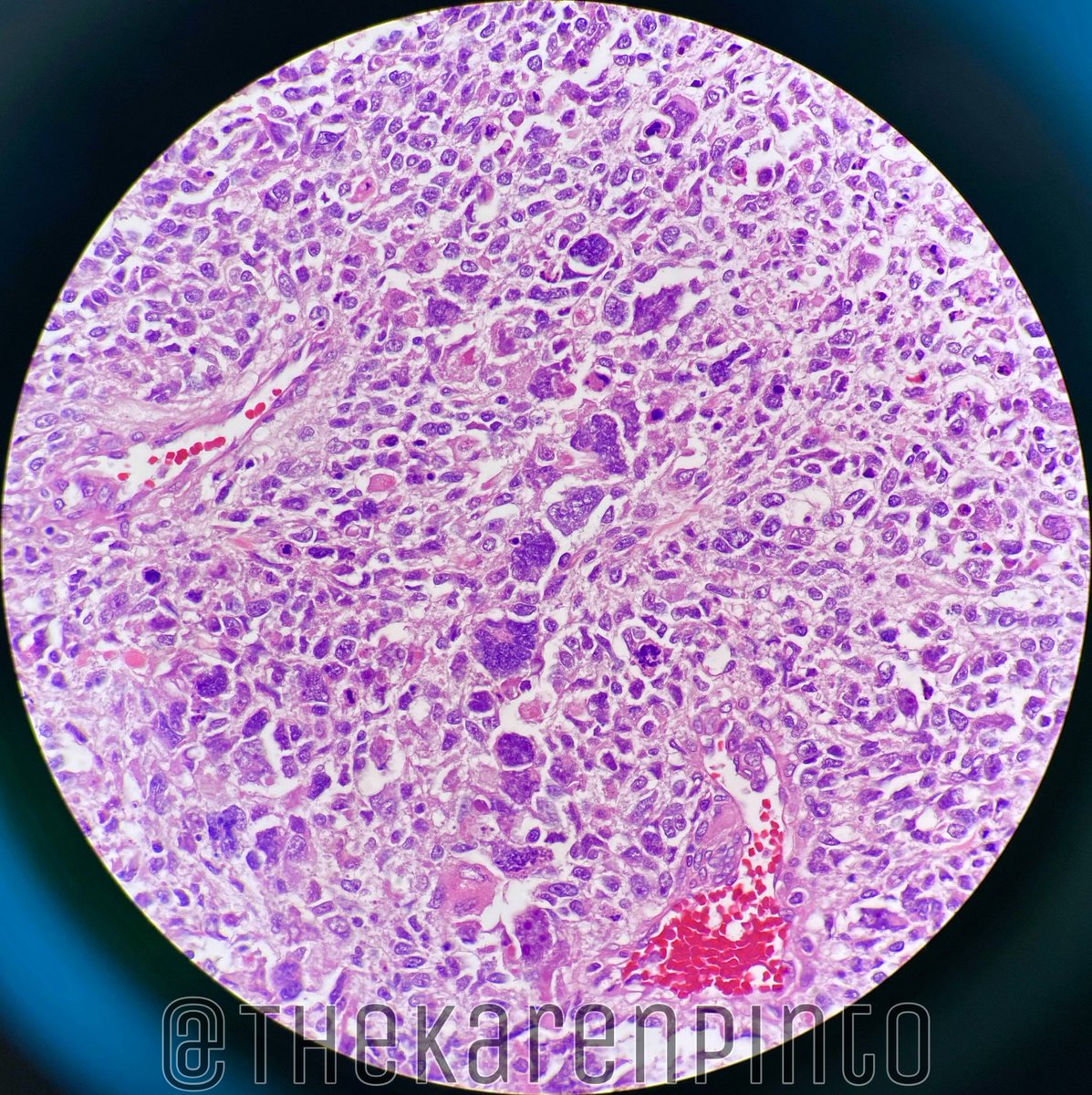
Other things I notice:
1. It’s not a blue tumor (neuroblastoma & synovial sarcoma not DDx any more)
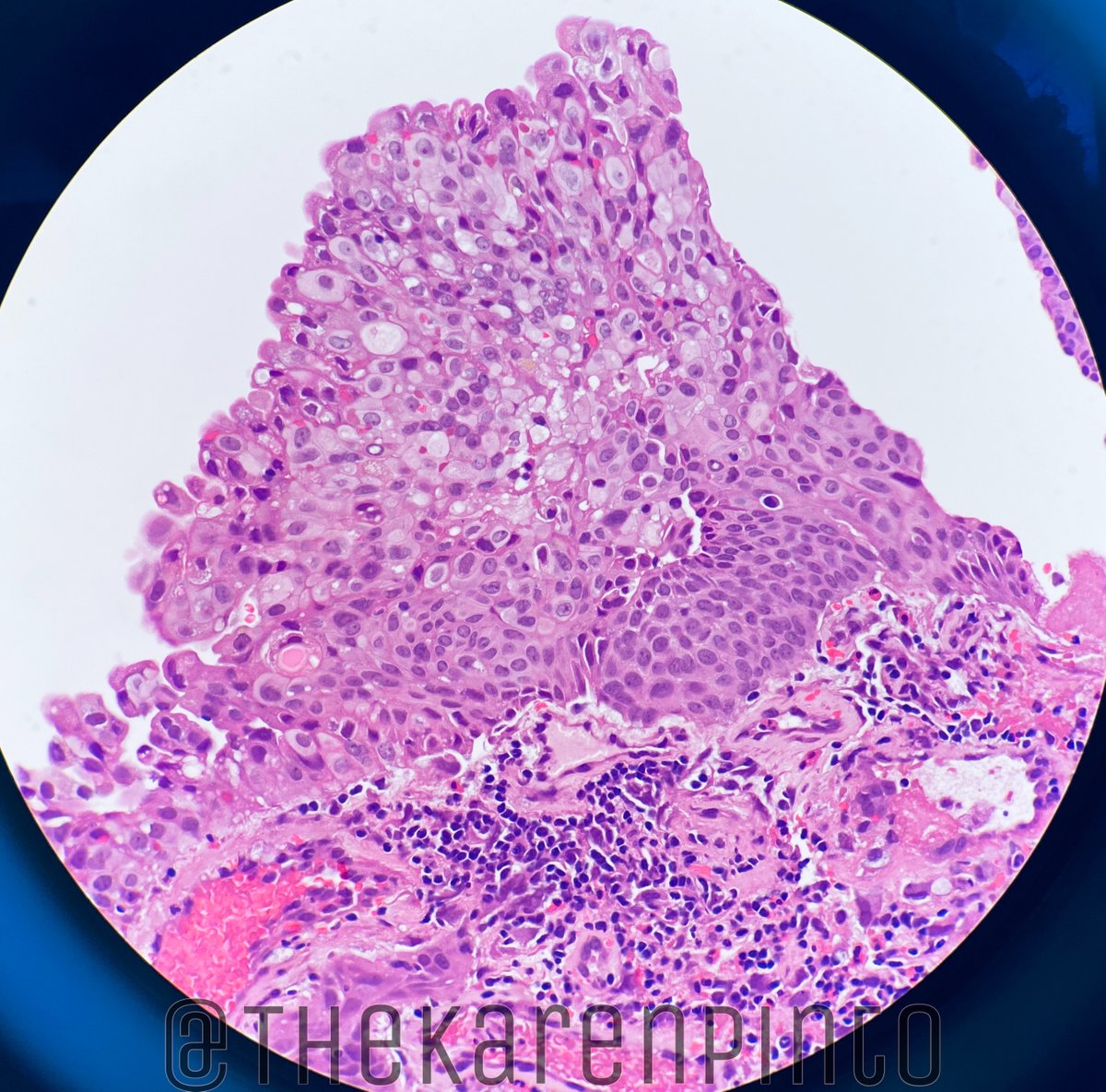
2. Cells with pink cytoplasm are seen (rhabdomyoblastic cells/differentiation)
1. It’s not a blue tumor (neuroblastoma & synovial sarcoma not DDx any more)
2. Cells with pink cytoplasm are seen (rhabdomyoblastic cells/differentiation)




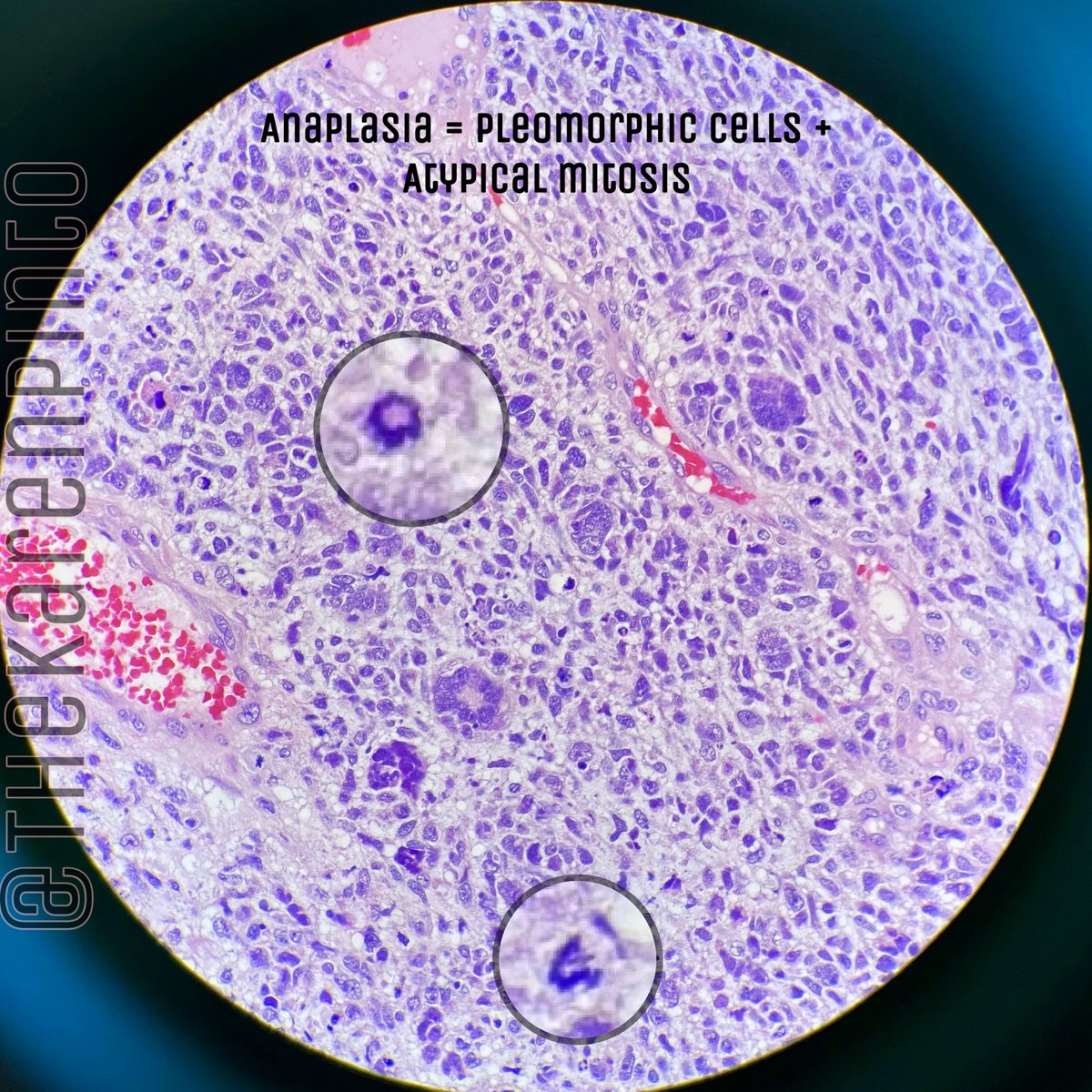
3. There are prominent bizarre large cells seen scattered throughout with atypical mitosis (anaplasia present)



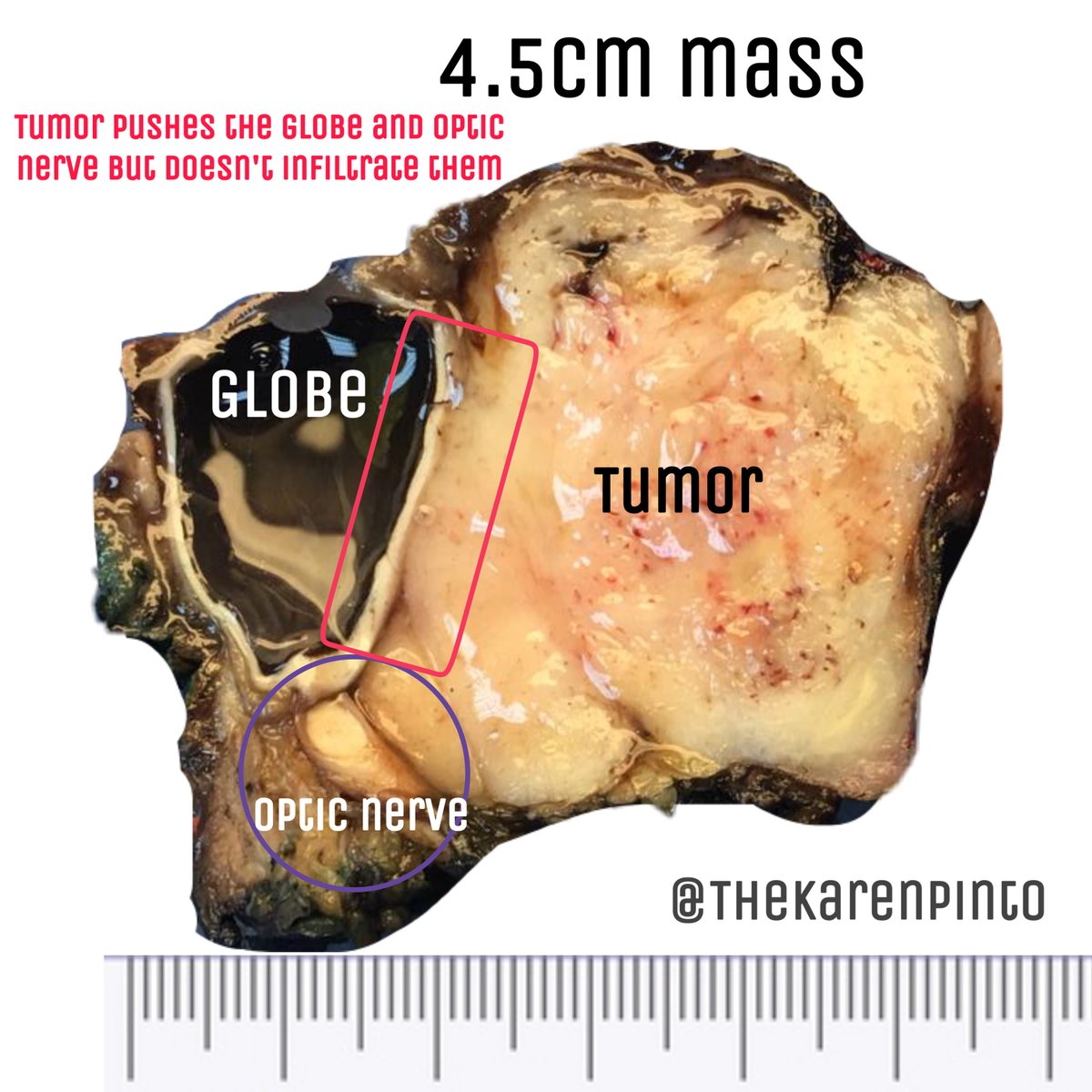
4. As seen on the gross, the tumor appears to be “organ confined / localized” without infiltration of the adjacent muscle or nerve



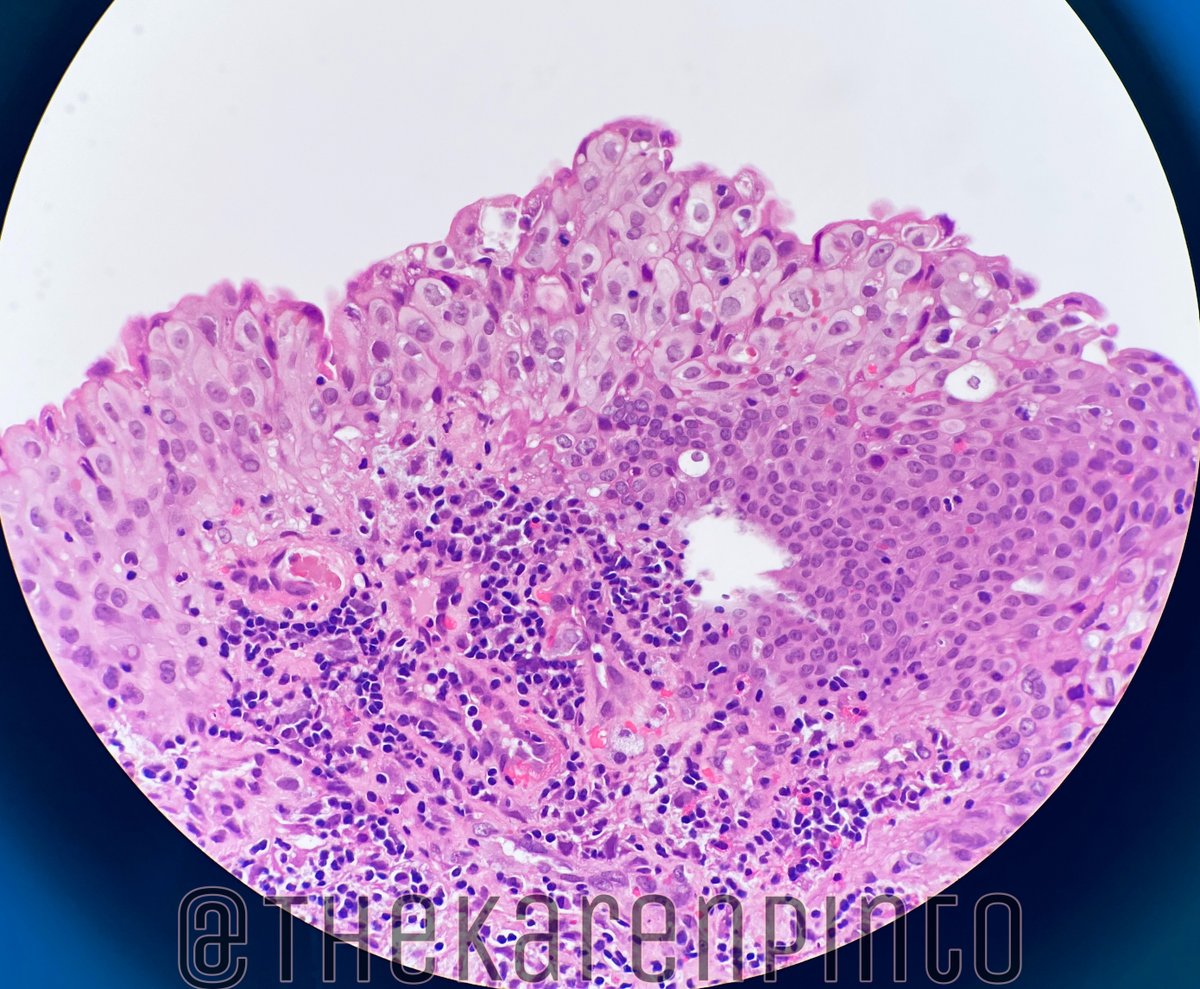
Age+orbit+micro= Rhabdomyosarcoma (RMS), embryonal type
Most common orbital malignancy in children
(*Also seen as a second malignancy, post-radiation, for treated cases of
-squamous cell carcinoma (eyelid)
-retinoblastoma)
Most common orbital malignancy in children
(*Also seen as a second malignancy, post-radiation, for treated cases of
-squamous cell carcinoma (eyelid)
-retinoblastoma)
HISTO:
A. Mosiac pattern (alternating cellular and myxoid areas)
B. Types of cells seen:
1. “Spider” / rhabdomyoblastic
2. Strap
3. Tadpole
A. Mosiac pattern (alternating cellular and myxoid areas)
B. Types of cells seen:
1. “Spider” / rhabdomyoblastic
2. Strap
3. Tadpole




3. Anaplasia present (diffuse - since you can see “clusters” of bizarre cells)


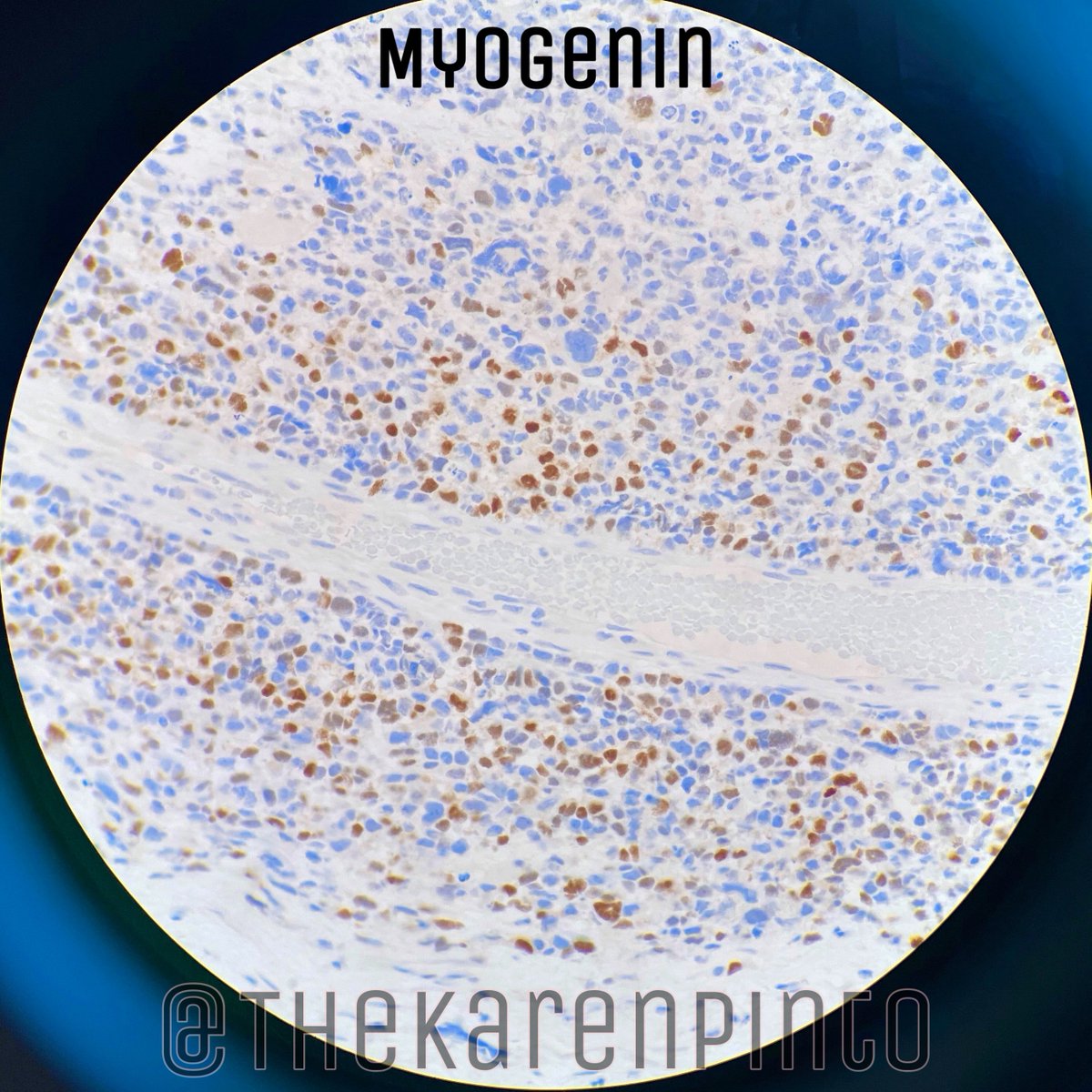
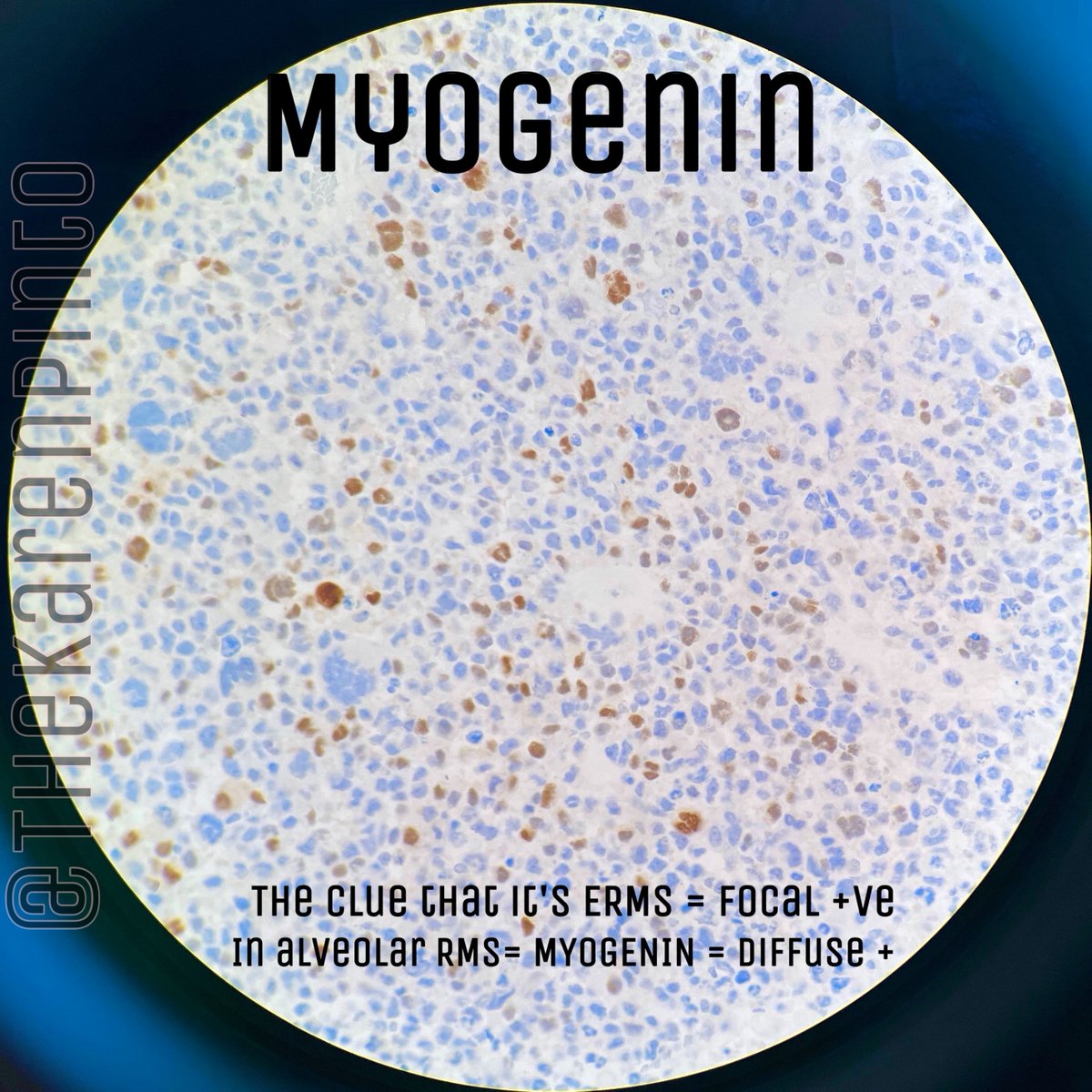
Immunostains:
Q. Myogenin staining helps differentiate embryonal RMS from it’s mimic: solid variant of alveolar RMS
Q. Myogenin staining helps differentiate embryonal RMS from it’s mimic: solid variant of alveolar RMS
True
Myogenin- “focal” / “patchy” staining in ERMS while it is DIFFUSELY positive in alveolar RMS
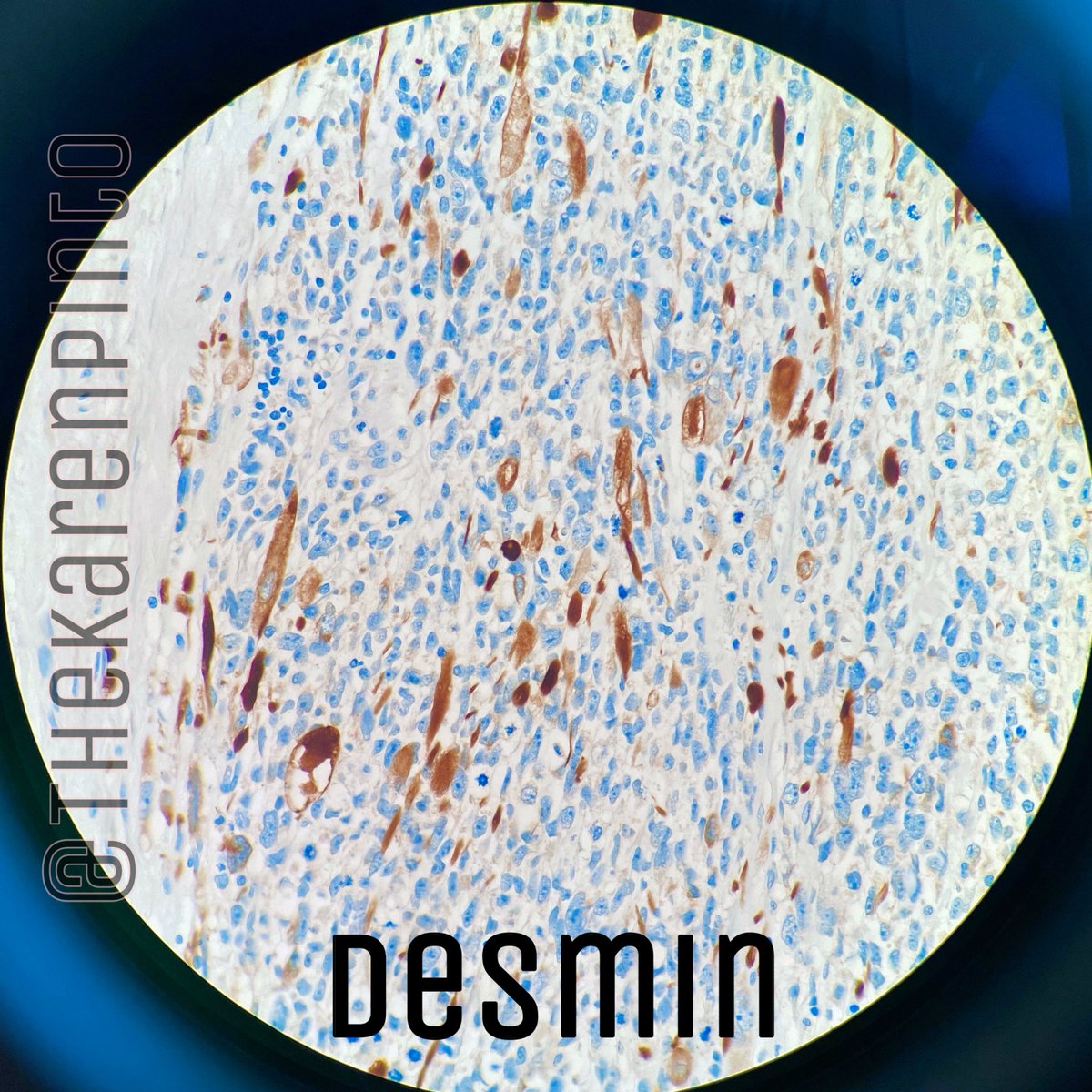
Desmin-positive
#IHCPath
Myogenin- “focal” / “patchy” staining in ERMS while it is DIFFUSELY positive in alveolar RMS
Desmin-positive
#IHCPath
Molecular hallmark of ERMS:
(LOH-loss of heterozygosity)
(LOH-loss of heterozygosity)
LOH 11p15.5
As well as chromosomal aneuploidies with gains of chromosome 8 (seen in 90% of patients)
All the others are seen with “alveolar” rhabdomyosarcomas
As well as chromosomal aneuploidies with gains of chromosome 8 (seen in 90% of patients)
All the others are seen with “alveolar” rhabdomyosarcomas
STAGING OF PEDIATRIC RMS:
Depends on 3 things:
1. Clinical Stage
2. Clinical Group
3. Clinical Risk group
Unlike other organ systems, there is NO AJCC stage given for head and neck ERMS or ARMS.
All the above staging systems, need clinical information
Depends on 3 things:
1. Clinical Stage
2. Clinical Group
3. Clinical Risk group
Unlike other organ systems, there is NO AJCC stage given for head and neck ERMS or ARMS.
All the above staging systems, need clinical information
(1) CLINICAL STAGE (modified site, size, metastasis staging)
*Based on pre-treatment characteristics
Three steps:
1. Assign path stage (image 1)
2. Check site (image 2)
3. Check radiology (for distant mets + lymph node (LN) involvement)
*Based on pre-treatment characteristics
Three steps:
1. Assign path stage (image 1)
2. Check site (image 2)
3. Check radiology (for distant mets + lymph node (LN) involvement)



(2) CLINICAL GROUP (*IRSG system)
*Based on pre-treatment characteristics
3 aspects:
1. Adequacy of surgery & residual disease (micro or grossly seen)
2. LN status
3. Disease extent (organ-confined / extensive)
(*IRSG-Intergroup RMS study group)
*Based on pre-treatment characteristics
3 aspects:
1. Adequacy of surgery & residual disease (micro or grossly seen)
2. LN status
3. Disease extent (organ-confined / extensive)
(*IRSG-Intergroup RMS study group)

(3) CLINICAL RISK GROUP
Again 3 aspects:
1. Clinical stage
2. Clinical group and
3. Fusion status (PAX/FOXO1) (ERMS-ve but alveolar RMS+ve)
Again 3 aspects:
1. Clinical stage
2. Clinical group and
3. Fusion status (PAX/FOXO1) (ERMS-ve but alveolar RMS+ve)

If you notice, in the clinical risk group, there is an important exception
*If the child is LESS THAN 10 years, in spite of having ‘Clinical Stage 4’ disease, they will be assigned ‘INTERMEDIATE’ risk group
*If the child is LESS THAN 10 years, in spite of having ‘Clinical Stage 4’ disease, they will be assigned ‘INTERMEDIATE’ risk group
Sites where RMS occurs in the eye:
-orbit
-eyelid
-conjunctive
-uveal tract
-orbit
-eyelid
-conjunctive
-uveal tract
4 main histological types of RMS:
1. Embryonal (including botyroid)
2. Alveolar (worst prognosis)
3. Spindle/sclerosing
4. Pleomorphic
1. Embryonal (including botyroid)
2. Alveolar (worst prognosis)
3. Spindle/sclerosing
4. Pleomorphic
RMS also has a syndromic association:
-Li-Fraumeni syndrome
-Dicer1 syndrome
-Neurofibromatosis type 1 (NF1)
-Costello syndrome
-Beckwith-Wiedemann syndrome
-Noonan syndrome
-Li-Fraumeni syndrome
-Dicer1 syndrome
-Neurofibromatosis type 1 (NF1)
-Costello syndrome
-Beckwith-Wiedemann syndrome
-Noonan syndrome
How do you treat RMS?
Combined therapy
Chemo-radiation with surgery
Combined therapy
Chemo-radiation with surgery
Newer treatments:
1. Immunotherapy
-vaccine therapy
-immune checkpoint inhibitor - Ipilimumab
-PD-1 inhibitor: Nivolumab / Pembrolizumab
2. Targeted therapy
-mTOR inhibitors (Sirolimus) for recurrent RMS
-tyrosine kinase inhibitors
1. Immunotherapy
-vaccine therapy
-immune checkpoint inhibitor - Ipilimumab
-PD-1 inhibitor: Nivolumab / Pembrolizumab
2. Targeted therapy
-mTOR inhibitors (Sirolimus) for recurrent RMS
-tyrosine kinase inhibitors
End of my very very long #pathtweetorial.
(PS: The patient age, sex and history have been changed to protect the patient's identity & it’s not a recent case)
(Hope most of you survived reading it till then end)
(PS: The patient age, sex and history have been changed to protect the patient's identity & it’s not a recent case)
(Hope most of you survived reading it till then end)