Thanks @UTMBFamilyMed for inviting me to present Grand Rounds today! I'm going to share a few pearls for other interested folks in #FamilyMedicine, #TwitteRx, & beyond.
A long but extremely visual🧵🧵🧵
A long but extremely visual🧵🧵🧵
To understand the "opioid crisis", you have to accept that the first wave was driven by excessive prescribing. BUT you also have to accept that reactionary supply reduction interventions drove a totally preventable second wave of deaths due to heroin.

In order to help the people who are actually dying today, you must recognize that deaths to Rx opioids accounted for fewer than ⅓ of all opioid overdose deaths, and that proportion is shrinking every year.

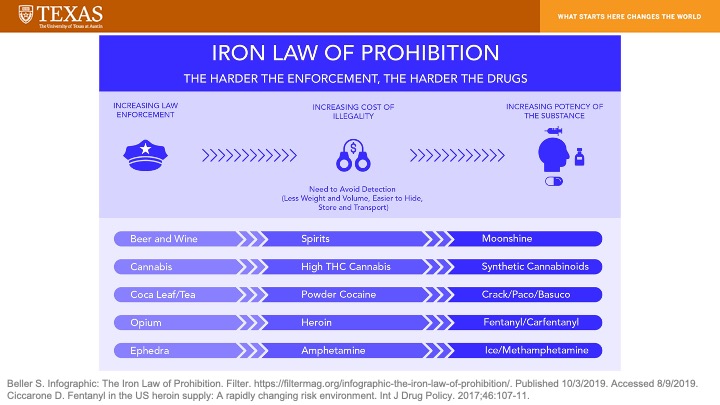
The explosion in deaths due to ultra-potent synthetic opioids (e.g. illicitly-manufactured #fentanyl) was predicted by many drug policy experts. However, government regulators and law enforcement did not heed their warnings.
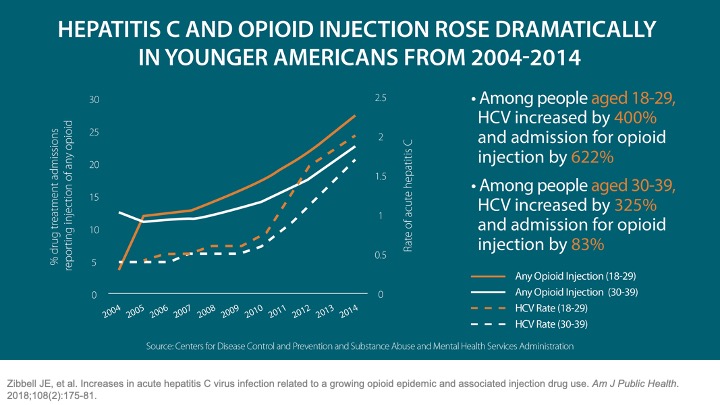
The broad transition from Rx opioids to illegal opioids in the U.S. has broader implications than just increasing overdose death rates. It has also been correlated with increased risk for injection-related complications, such as hepatitis C virus. #HCV
Despite a pharmacokinetic profile that would indicate a delayed onset and prolonged duration of action, the user experience with #fentanyl is actually quite the opposite when compared to heroin.
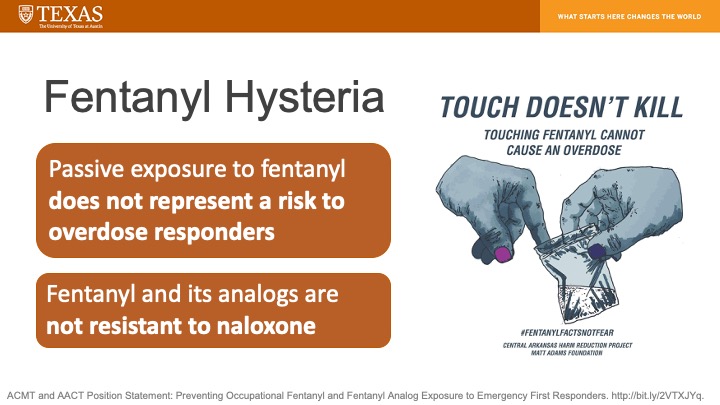
So, there are clearly some unique concerns related to illicitly-manufactured #fentanyl. There is also a lot hysteria. Don't buy into these myths!
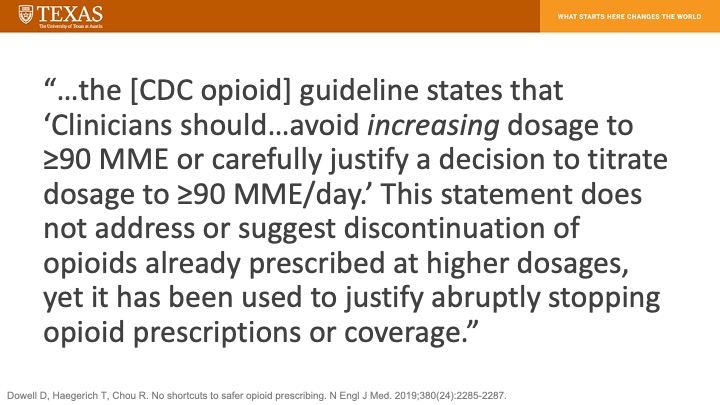
Too many healthcare professionals are still focused on tapering the daily opioid dose (#MME) of patients with chronic pain. Authors of the CDC guideline have issued a public clarification to discontinue this misapplication of their recommendations.
The clarification was important. Observational studies have shown opioid tapers are often far too rapid, leading to hospitalizations and ED visits...

...and that opioid discontinuation is associated with increased risk for death by overdose and suicide. Note: There are substantial limitations to these study designs, but their findings are still alarming.


While it's debatable whether medications for OUD (#MOUD) should be considered #HarmReduction rather than simply "treatment", the philosophy behind them fits.
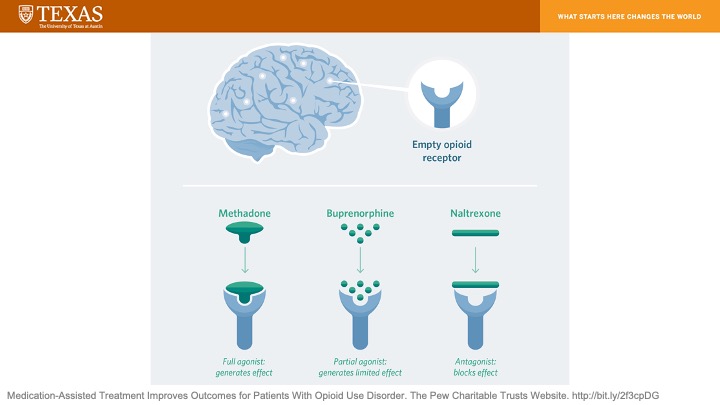
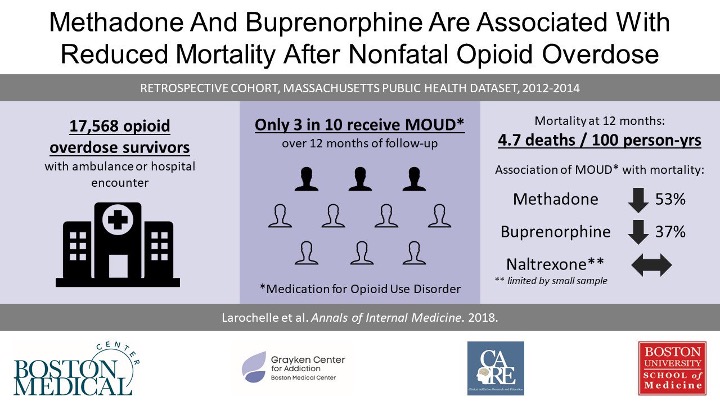
#Methadone & #buprenorphine appear to be the most effective MOUD (at least of those approved for use in the U.S.). Despite being proven to save lives, very few patients who need these medications are prescribed them...even after experiencing a non-fatal overdose.
The majority of inpatient "addiction treatment centers" DON'T OFFER ANY MOUD. These facilities are death traps that should be shuttered by the federal government.

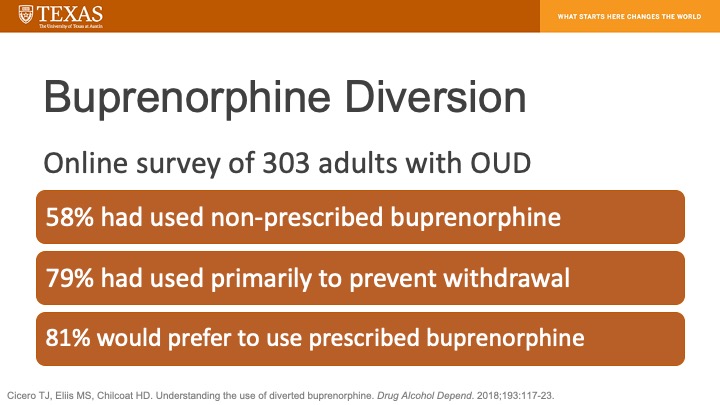
If you're worried about #buprenorphine diversion...don't be. A substantial majority of non-prescribed buprenorphine use appears to be therapeutic...
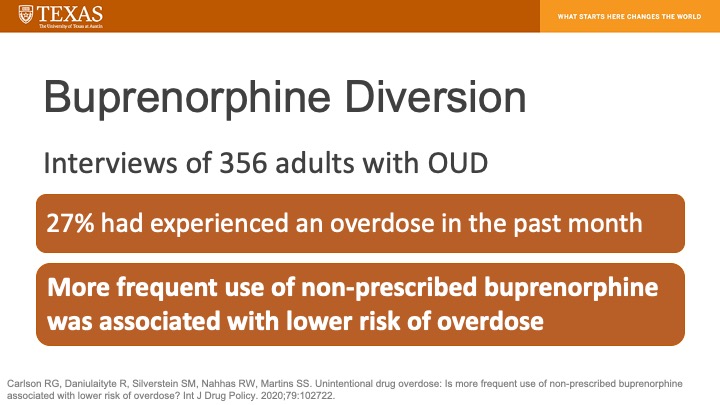
...and more frequent use of non-prescribed #buprenorphine is associated with a lower risk of overdose.
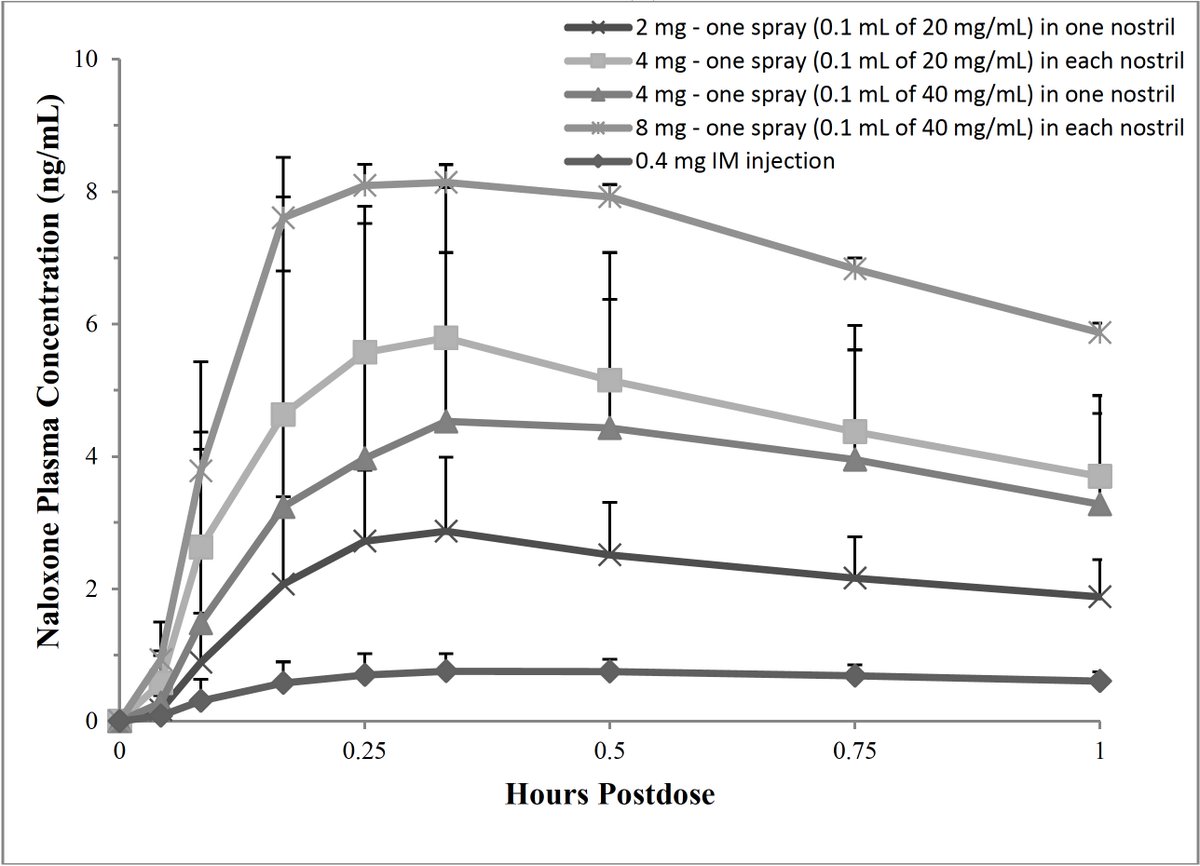
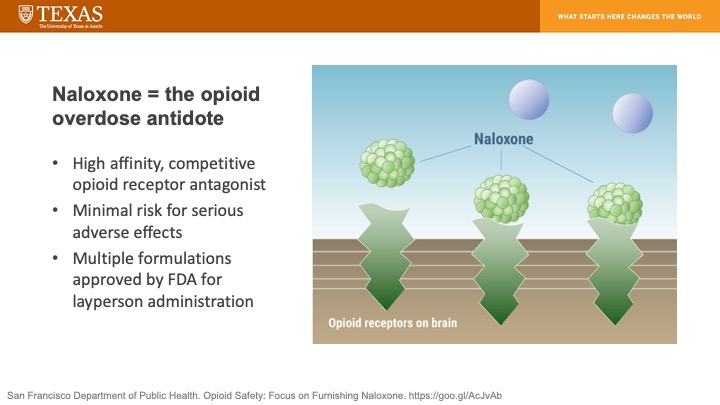
Anyone at risk for experiencing an opioid-related overdose should be prescribed #naloxone. Naloxone is an opioid receptor antagonist (blocker) that can quickly reverse the effects of an overdose regardless of whether it is due to fentanyl, heroin, or an Rx opioid.
Every U.S. state has enacted a naloxone access law with the goal of increasing access to this life-saving medication.

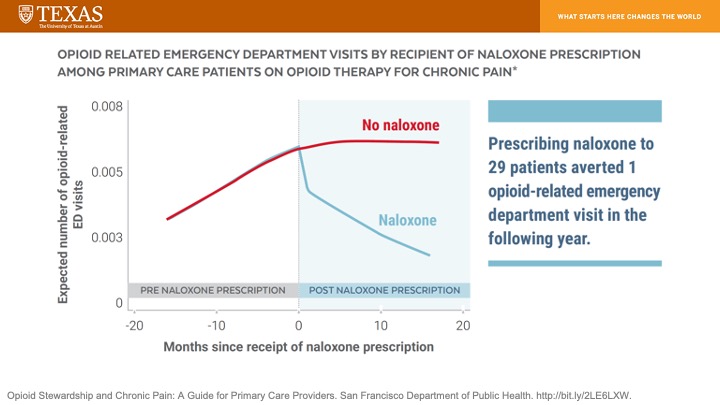
#Naloxone isn't just for people with OUD. Co-prescribing it to patients who take opioids for chronic pain is proven to dramatically reduce their risk for opioid-related ED visits.
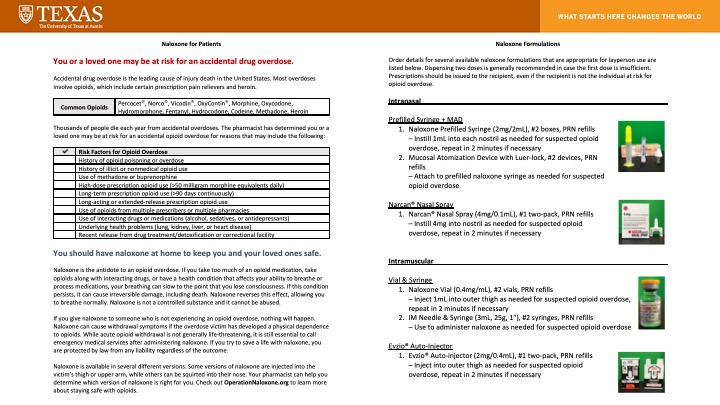
However, patients with chronic pain tend not to relate to the term "overdose" & may even find it offensive. Approach them thoughtfully while recognizing that they live in fear of a prescriber suddenly taking away their medication and plunging them into withdrawal + severe pain.

Our team @OperationNLX developed some patient- and clinician-directed handouts to facilitate discussions regarding #naloxone. You can obtain digital copies at OperationNaloxone.org & are free to print + distribute at will.
We also have a free one-hour CE program at OperationNaloxone.org & will be posting many new programs on the website over the next few months!
#MOUD & #naloxone are only the tip of the iceberg when it comes to #HarmReduction. The real work is being done by @PAHarmReduction @TexasHRA @iaharm
@HarmReduction @Devin_Reaves @sarah_ziggy @clairezagorski & countless others who continue to be overlooked & ignored.
@HarmReduction @Devin_Reaves @sarah_ziggy @clairezagorski & countless others who continue to be overlooked & ignored.
Syringe service programs are proven to have numerous benefits & are endorsed by @CDCgov.

However, syringe service programs remain illegal in 12 U.S. states & face substantial barriers to operation in others.

We should be supporting & expanding syringe service programs AND establishing supervised injection facilities throughout the U.S. If you're on the fence, this essay from @jessiegaeta will move you to the correct side.
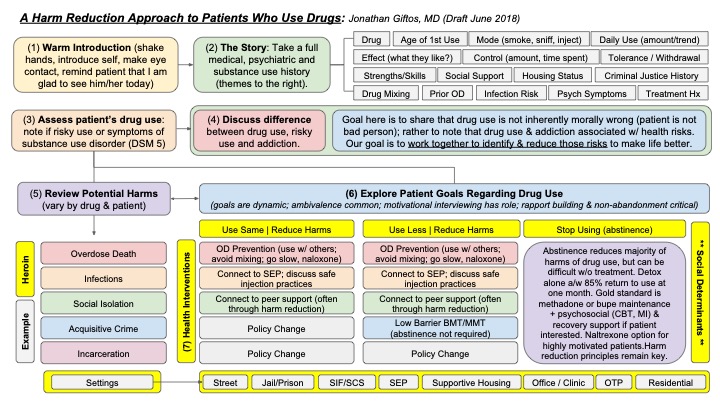
Implementing a harm reduction approach in your practice doesn't have to be complicated, even if this awesome algorithm for doing so is. Shoutout to @JonGiftosMD!
One more thing. Be mindful of the language you use when speaking to and about people who use drugs. You don't have to be perfect, but strive to be better. Correct colleagues who consistently use stigmatizing language.

Here are your key takeaways. Thanks for sticking with me to the bitter end of this extremely long thread, & thanks again to @UTMBFamilyMed for inviting me to present this information to their residents.