1/Published: “Nonconsensual Dose Reduction Mandates are Not Justified Clinically or Ethically: An Analysis” -In Journal of Law, Medicine & Ethics, with @AjayManhapra @AJ_Gordon. Given the paywall, I’ll offer key points #ChronicPain #opioids
journals.sagepub.com/doi/abs/10.117…
journals.sagepub.com/doi/abs/10.117…

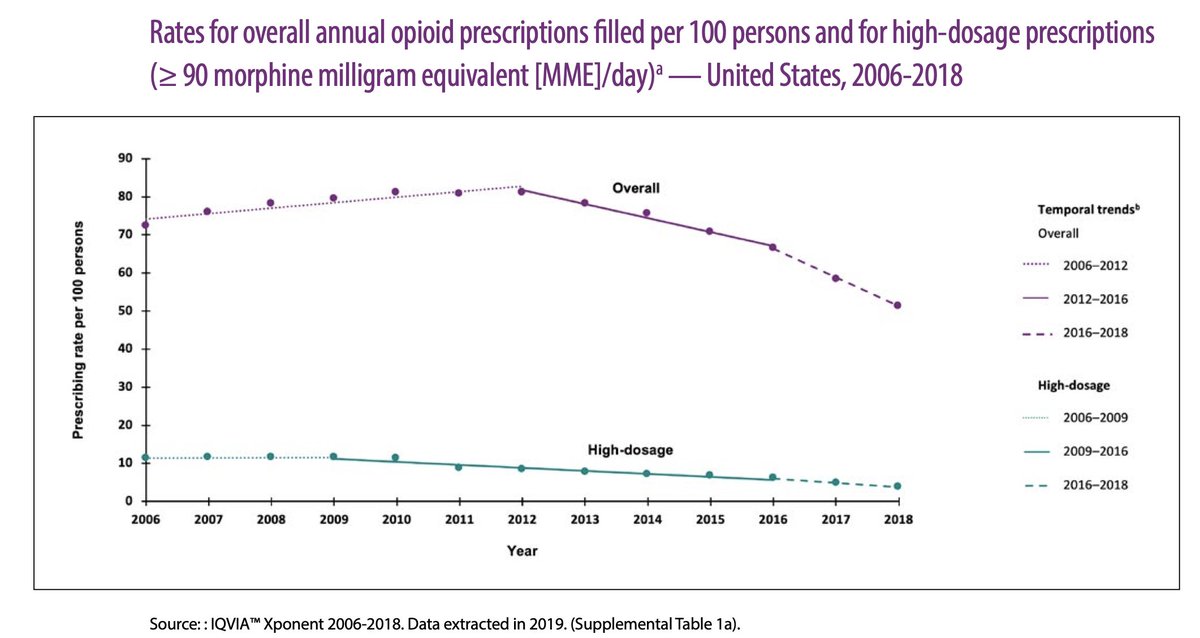
2/Historic context: #Opioid prescribing (peaking in 2012) was part of a crisis we face now. Their embrace reflected a collective failure by payers, educators, and boards who *never fostered expertise in pain, or addiction.* They/we set the table for poor care then, and now
3/Opioid Rx’s began to fall 2012, & that sped up after a @cdcgov guideline that urged caution in dosing, but did NOT require opioid stoppage or taper. CDC’s language was (still is) weaponized by insurers, employers, pharmacies, quality metric agencies
4/Despite efforts to fix misuse of @CDCgov Guideline in 2019, there was no shift in policy, e.g. laws mandating dose limits(SUPPORT Act),pharmacy benefits,etc. HHS-OIG says it uses doses to decide on referral for criminal investigation. That’s pressure.oig.hhs.gov/oei/reports/oe…
5/Why, clinically, is #opioid taper a conundrum? Start with Pain: it’s a complex nociceptive & emotional experience. No treatment has strong long-term evidence. Opioids’ mean benefit is low but at times it's the only thing that works. There is benefit for some (and yes, risk)
6/Dependence (usually NOT addiction) is part of the opioid bargain. With any form of relief or reward, there's “pushback” in the brain called “opponent process” –described first in psychology (1980s lit) and then neurobiology. Our excerpt below. One ref: ncbi.nlm.nih.gov/pmc/articles/P…
7/How often does dependence/opponent process look “problematic” clinically? In surveys predating Rx cut-backs, 7-15% of patients & families reported problems with overuse and fear they were addicted, etc. Likely most wouldn’t qualify for OUD diagnosis.
ncbi.nlm.nih.gov/pmc/articles/P…
ncbi.nlm.nih.gov/pmc/articles/P…
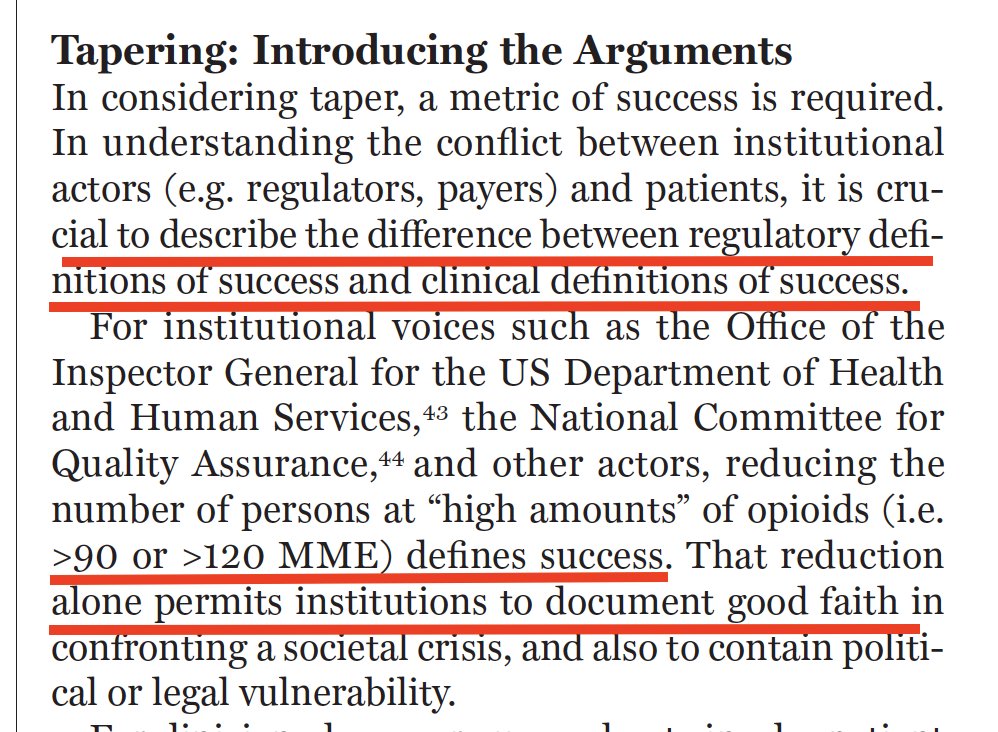
8/I wish it were the case that we just had a clinical question to wrestle with. But right now the *TENSION* is because institutional metrics of success used by regulators (total pills prescribed) are different from those that matter clinicians ("is my patient healthy & safe?")
9/So what's the evidence *for* opioid dose reduction? Evidence FOR taper comes from a superb 2017 summary of studies rated mostly as “low quality”, involving voluntary patients, with hints of improvement across a range of outcomes, with supportive care and dose reduction.

10/Data *not for* opioid taper? 1st- the 2017 summary said they lacked data on mandates (or quasi-mandates) like we have now, or on suicidality or resort to illegal opioids. Strange that Congress, HHS-OIG, insurers and pharmacies all made a policy of something with no data, huh?

11/Let’s say it: if you didn’t like hydroxychloroquine touted for COVID19 based on thin data, you should not like *federal laws, investigative thresholds, quality metrics, or payer decisions* based on an assumption that dose reduction is always good, without any data for that
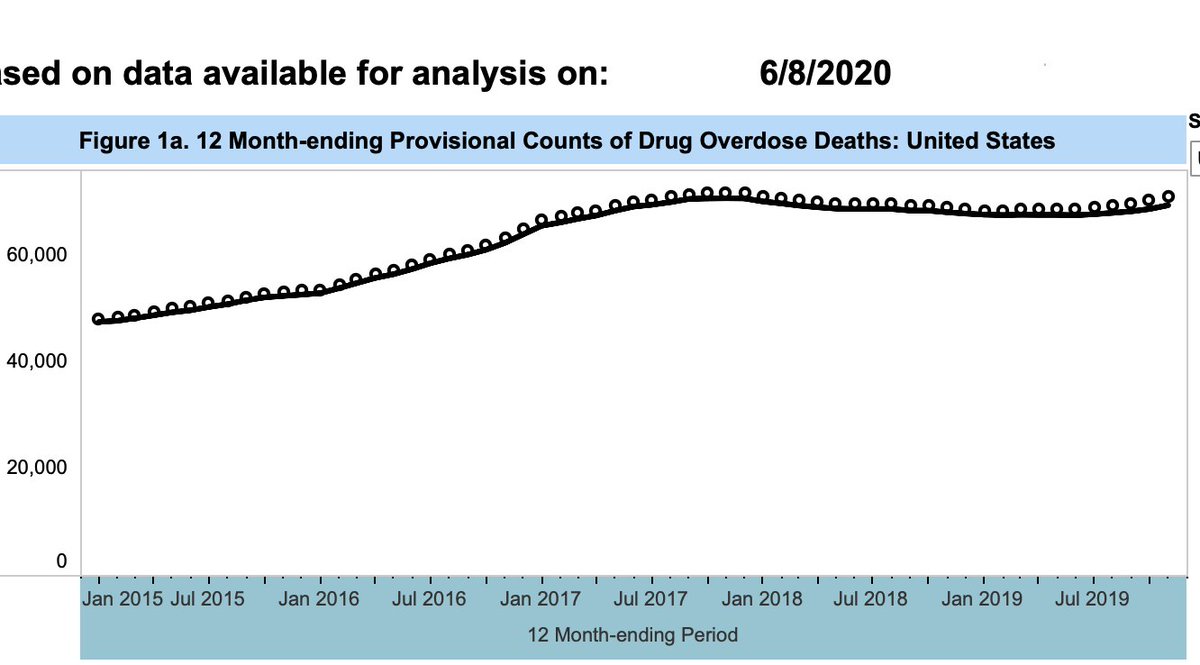
12/Data against 2nd: Rx opioid OD mostly is in folks with low-dose Rx, or no Rx. Polypharmacy, life chaos, lack of therapeutic relationships historically characterize both prescription and non-prescription (heroin) overdoses. Dose reductions don’t address their risk at all.

13/And remember that lack of data on outcomes from involuntary Rx opioid stoppage &taper? Well, we have data now. It looks bad for safety. Yes, the authors know “stoppage” can reflect *actual concerning behaviors* in patients. But stoppage seems to make safety worse, not better


15/Clinicians are subject a distinct ethic. We aren’t allowed to treat patients as a "means to an end", but only as "an end in themselves". Bowing to pressure, despite concern a patient will be hurt, violates a categorical imperative, described by Kant (1st time we cite Kant!)

16/When clinicians are asked to uphold institutional interests in ways that conflict with patient protection, that’s termed “dual agency” – and there is no one solution for that, because it happens in many different ways, we note pubmed.ncbi.nlm.nih.gov/25127273/
17/For this situation we suggest “do no harm” can anchor us. Yes, scrutinize your opioid Rx. Taper can & should be discussed if you plan to monitor and reverse course if harm emerges. But actions that risk “grievous harm” in favor of institutional pressures are not justifiable.
18/Conclusion: For now, clinicians seeking to uphold a fiduciary duty to patients, on the matter of #opioid prescriptions, will continue to find their actions are in tension with the agencies that pay, regulate, measure and govern us. Gratitude to @AjayManhapra @AJ_Gordon /FIN