
Hi #MedTwitter #NeuroTwitter #medstudenttwitter!
How about another #EndNeurophobia neuroanatomy #tweetorial?
This one goes out to all those USMLE studiers out there:
THE BASAL GANGLIA
cc: @CrystalYeoMDPhD @MadSattinJ @Tracey1milligan @DxRxEdu @CPSolvers @MedTweetorials
How about another #EndNeurophobia neuroanatomy #tweetorial?
This one goes out to all those USMLE studiers out there:
THE BASAL GANGLIA
cc: @CrystalYeoMDPhD @MadSattinJ @Tracey1milligan @DxRxEdu @CPSolvers @MedTweetorials
Grateful for ❤️ #EndNeurophobia received but hope you read rest of my feed seeking to amplify voices I’m learning from on path to being an antiracist ally.
follow @BlackInNeuro @LashNolen @uche_blackstock @DrOniBee @gradydoctor
listen @thepraxispod @thenocturnists
read @DrIbram
follow @BlackInNeuro @LashNolen @uche_blackstock @DrOniBee @gradydoctor
listen @thepraxispod @thenocturnists
read @DrIbram
First, the anatomy:
The basal ganglia are islands of gray matter embedded in the subcortical white matter. Texts vary on what they include but most agree on at least:
Caudate
Putamen
Globus pallidus (interna and externa)
Subthalamic nucleus
I’ll call these C, P, GPi, GPe, STN
The basal ganglia are islands of gray matter embedded in the subcortical white matter. Texts vary on what they include but most agree on at least:
Caudate
Putamen
Globus pallidus (interna and externa)
Subthalamic nucleus
I’ll call these C, P, GPi, GPe, STN
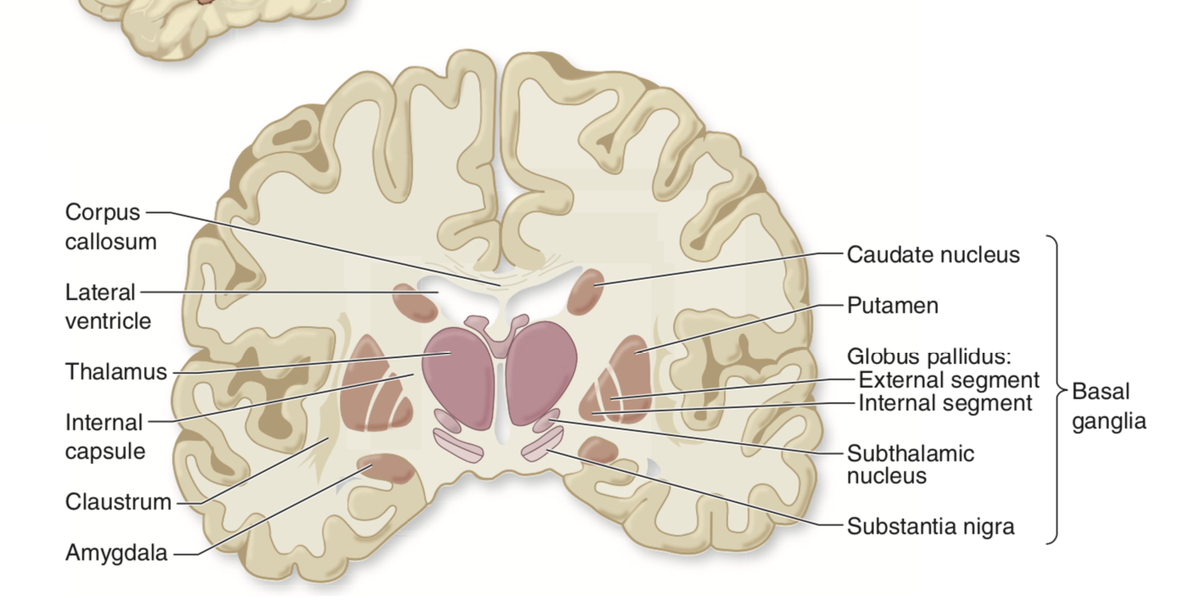
Caudate + putamen = STRIATUM
Putamen + GP together = LENTICULAR NUCLEI
C runs just lateral to the lateral ventricles.
Gpi is nestled medial to the GPe, which is nestled just medial to the putamen.
STN sits inferior to the thalamus as name suggests
Putamen + GP together = LENTICULAR NUCLEI
C runs just lateral to the lateral ventricles.
Gpi is nestled medial to the GPe, which is nestled just medial to the putamen.
STN sits inferior to the thalamus as name suggests
Now for the circuit we have to memorize = a model for how BG are involved in control of movement.
This is likely an oversimplification but is helpful in understanding 2 conditions: PARKINSON’s and HEMIBALLISMUS
This can get confusing so let’s build it up piece by piece
This is likely an oversimplification but is helpful in understanding 2 conditions: PARKINSON’s and HEMIBALLISMUS
This can get confusing so let’s build it up piece by piece
First, understand the basic LOOP circuit:
Motor cortex->BG->Thalamus (VL/VA nuc)->back to cortex
Cortex excites BG, thalamus excites cortex, but whether the overall circuit INCREASES motor cortex activity or DECREASES it depends on the OUTPUT of the BG.
Motor cortex->BG->Thalamus (VL/VA nuc)->back to cortex
Cortex excites BG, thalamus excites cortex, but whether the overall circuit INCREASES motor cortex activity or DECREASES it depends on the OUTPUT of the BG.

If BG output = +, then we have + + + = + = increase motor activity
If BG output = -, then we have + - + = - =decrease motor activity
If BG output = -, then we have + - + = - =decrease motor activity


Now let’s see what happens within the BG. We have two circuits DIRECT pathway and INDIRECT pathway.
BOTH begin in C/P and end with GPi.
INDIRECT adds GPe and STN
BOTH begin in C/P and end with GPi.
INDIRECT adds GPe and STN
DIRECT pathway:
C/P inhibits GPi which inhibits thalamus, so within BG C/P inhibits GPi from inhibiting thalamus =decrease inhibition, so VL/VA are not inhibited and can excite cortex
So: - x - = overall + (the negatives cancel)
So DIRECT pathway DIsinhibits= ⬆️ motor activity
C/P inhibits GPi which inhibits thalamus, so within BG C/P inhibits GPi from inhibiting thalamus =decrease inhibition, so VL/VA are not inhibited and can excite cortex
So: - x - = overall + (the negatives cancel)
So DIRECT pathway DIsinhibits= ⬆️ motor activity

INDIRECT adds GPe and STN.
Note that ALL internal synapses in BG circuit here are – EXCEPT STN->GPi which is +
so indirect pathway = - x - x + x - = overall – so INdirect pathway INhibits =⬇️motor activity
In sum DIRECT = the gas, INDIRECT = the brake.
Note that ALL internal synapses in BG circuit here are – EXCEPT STN->GPi which is +
so indirect pathway = - x - x + x - = overall – so INdirect pathway INhibits =⬇️motor activity
In sum DIRECT = the gas, INDIRECT = the brake.

Now we must add another layer: the substantia nigra (SN)
SN sends dopaminergic projections to C/P
Dopamine acts at D1 receptors to EXCITE the D1rect pathway, and at D2 receptors to INHIBIT the Indirect pathway.
SN sends dopaminergic projections to C/P
Dopamine acts at D1 receptors to EXCITE the D1rect pathway, and at D2 receptors to INHIBIT the Indirect pathway.

So SN->BG = increase direct (gas) and decrease indirect (brake) meaning overall more gas /less brake = ⬆️ motor activity.
In PARKINSON’S DISEASE, SN degenerates->lose dopaminergic input to BG
Less stimulation of direct pathway (⬇️gas) and less Inhibition of Indirect pathway (⬆️ brake) = overall indirect wins=less motor activity
This explains bradykinesia and rigidity of PD but not tremor.
Less stimulation of direct pathway (⬇️gas) and less Inhibition of Indirect pathway (⬆️ brake) = overall indirect wins=less motor activity
This explains bradykinesia and rigidity of PD but not tremor.

STN and GPi are targets of Deep Brain Stimulation in PD.
DBS INHIBITS activity in these structures—see how inhibiting either would lead to decreased inhibitory output of BG = increased motor activity-> improve PD symptoms?
DBS INHIBITS activity in these structures—see how inhibiting either would lead to decreased inhibitory output of BG = increased motor activity-> improve PD symptoms?
Lesion of STN ->HEMIBALLISMUS=uncontrolled erratic large amplitude movements on one side.
Why INCREASED movement with STN lesion?
By decreasing STN excitation of GPi we essentially ‘remove’ indirect pathway from equation, and direct pathway becomes unchecked -> ⬆️movement
Why INCREASED movement with STN lesion?
By decreasing STN excitation of GPi we essentially ‘remove’ indirect pathway from equation, and direct pathway becomes unchecked -> ⬆️movement
So in sum
Direct=
Ctx->C/p->GPi->thal->ctx
+ - - + = overall +
DIrect DIsinhibits = gas= Drive
Indirect Ctx->C/p->GPe->STN->GPi->thal->ctx
+ - - + - + = overall inhibits
INdirect INhibits = gas
Dopamine from SN ⬇️Direct and ⬆️ INdirect
Direct=
Ctx->C/p->GPi->thal->ctx
+ - - + = overall +
DIrect DIsinhibits = gas= Drive
Indirect Ctx->C/p->GPe->STN->GPi->thal->ctx
+ - - + - + = overall inhibits
INdirect INhibits = gas
Dopamine from SN ⬇️Direct and ⬆️ INdirect
Now do we use this in practice? Not really, but it's a helpful model for understanding how the brain creates complexity out of pluses and minuses and some features of PD, DBS, and hemiballismus on an anatomic/physiologic basis.
What should I cover next?
#EndNeurophobia 🧠❤️
What should I cover next?
#EndNeurophobia 🧠❤️

