I promise that if #hydroxychloroquine was an effective therapy for #covid19 we would tell you. Many of us (myself definitely included) were hopeful that it would be at the onset of the pandemic. We now know definitively that it doesn’t work. A (long) thread
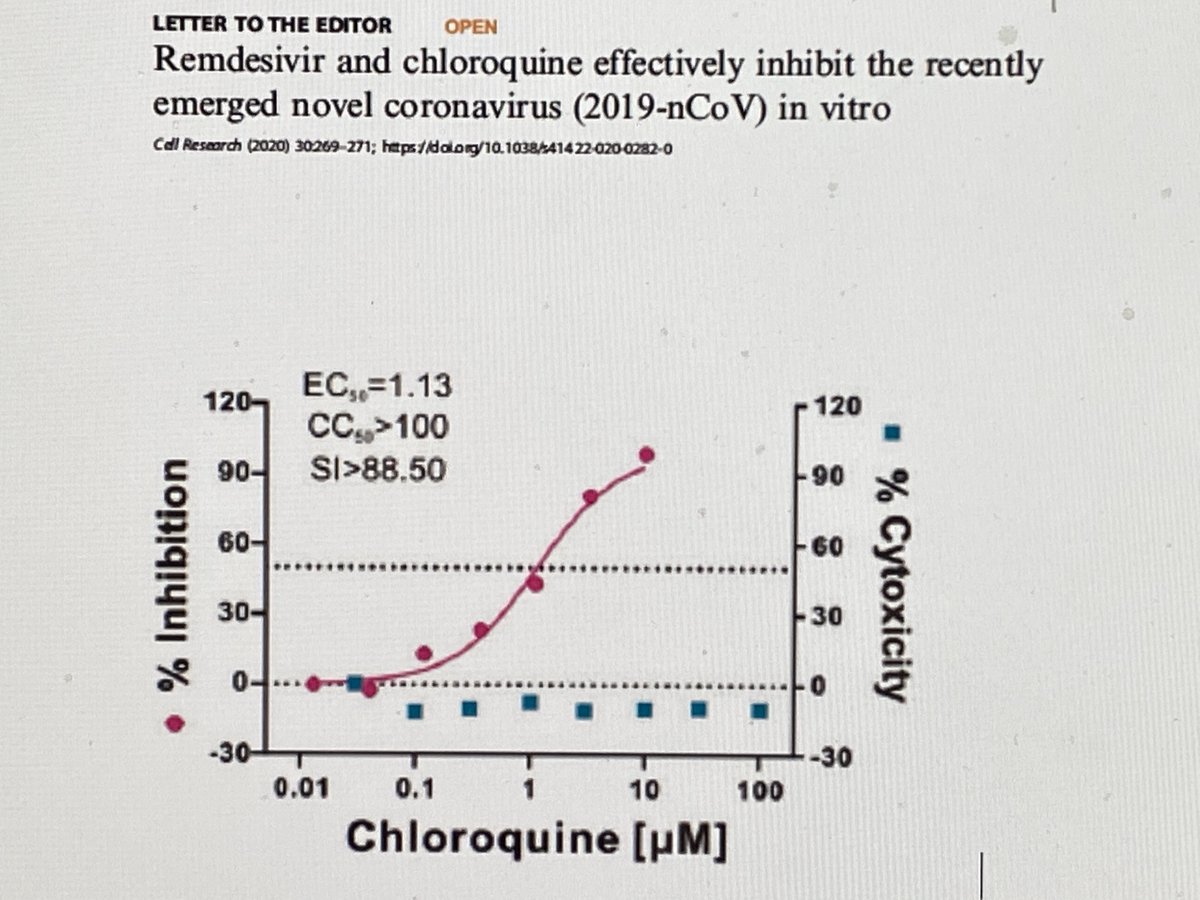
The initial hope for HCQ stemmed from in vitro work in Vero (kidney) Cells that showed potent inhibitory activity of CQ (and subsequently HCQ). 
Unfortunately, recent data demonstrate that Vero cells are a particularly bad option for assessing the in vitro activity of HCQ against SARS CoV-2 due to HCQs mechanism of action. Allow me to explain
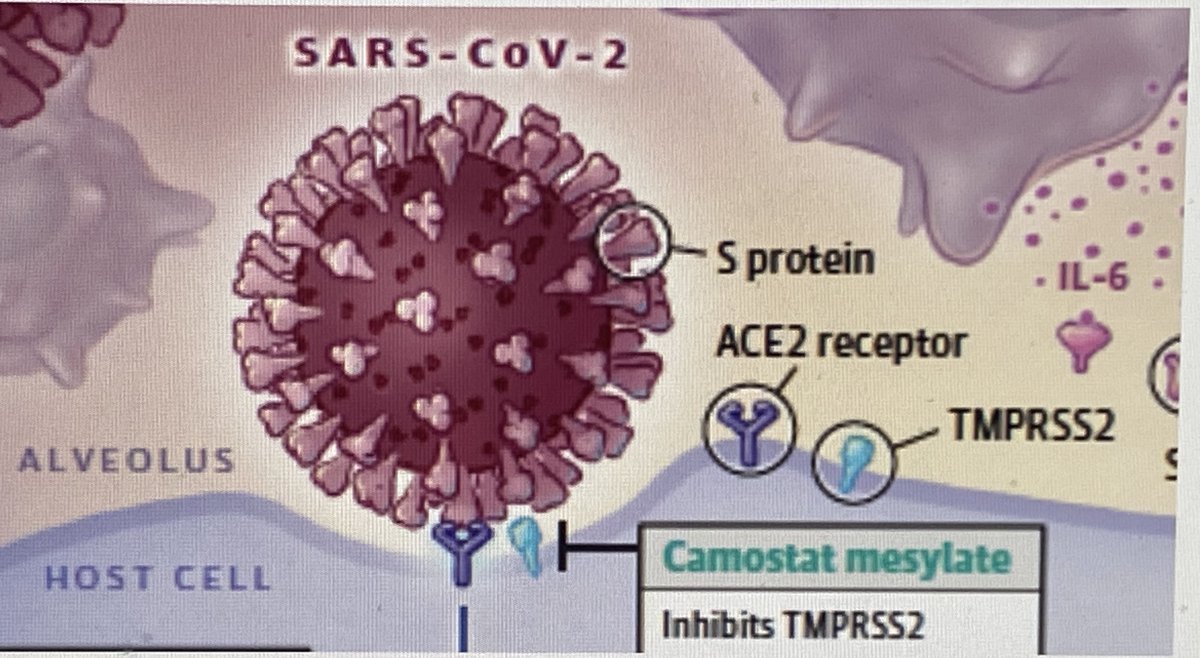
In Vero cells the SARS-CoV-2 spike protein (which mediates viral entry into cell) is activated by the endosomal pH-dependent cysteine proteases cathepsin B and L (Cat B/L). HCQ, by raising the endosomal pH will therefore inhibit this protease, cell entry, and ultimately the virus
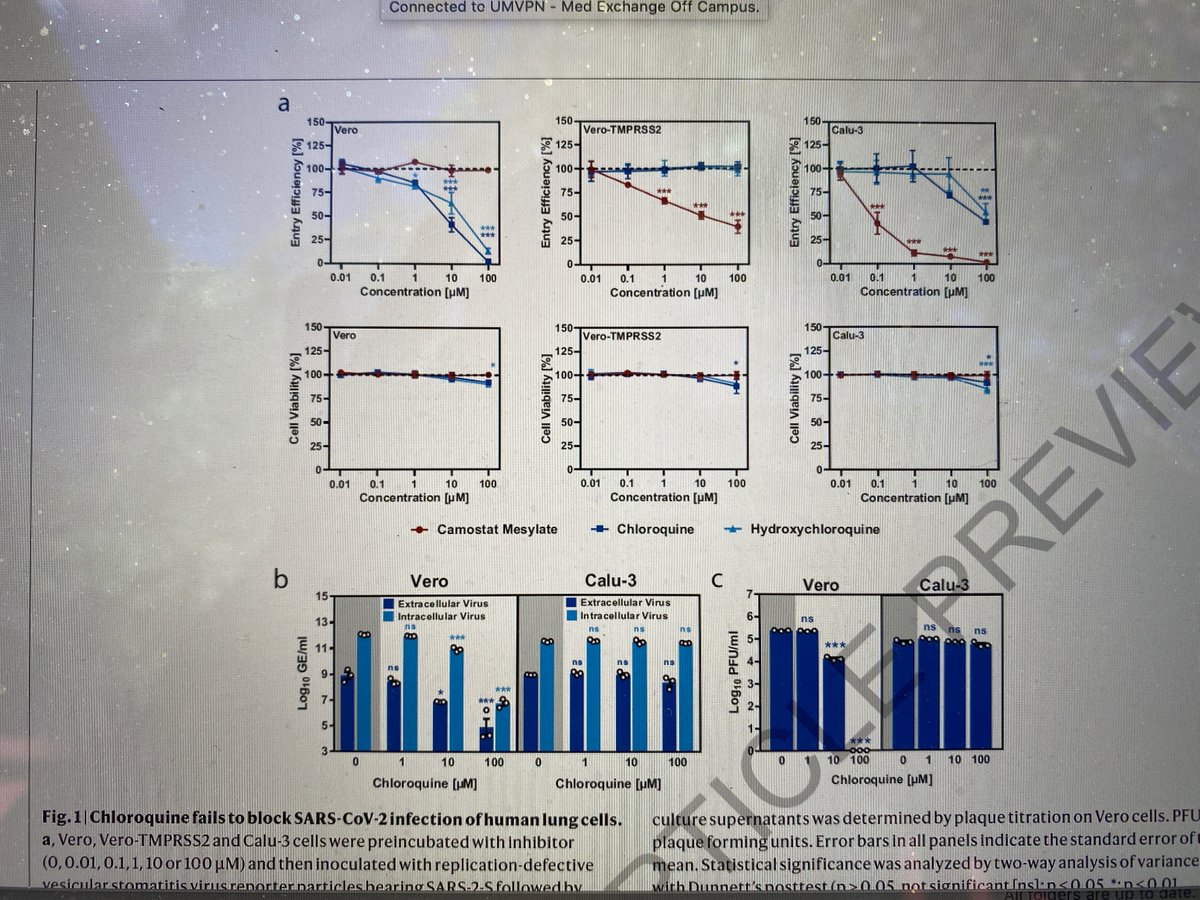
This is demonstrated nicely by the antiviral effect seen in with increasing concentrations of HCQ in Vero cell analyses (see top left figure and the left figures of "b" and "c". Increasing CQ, increasing effect.
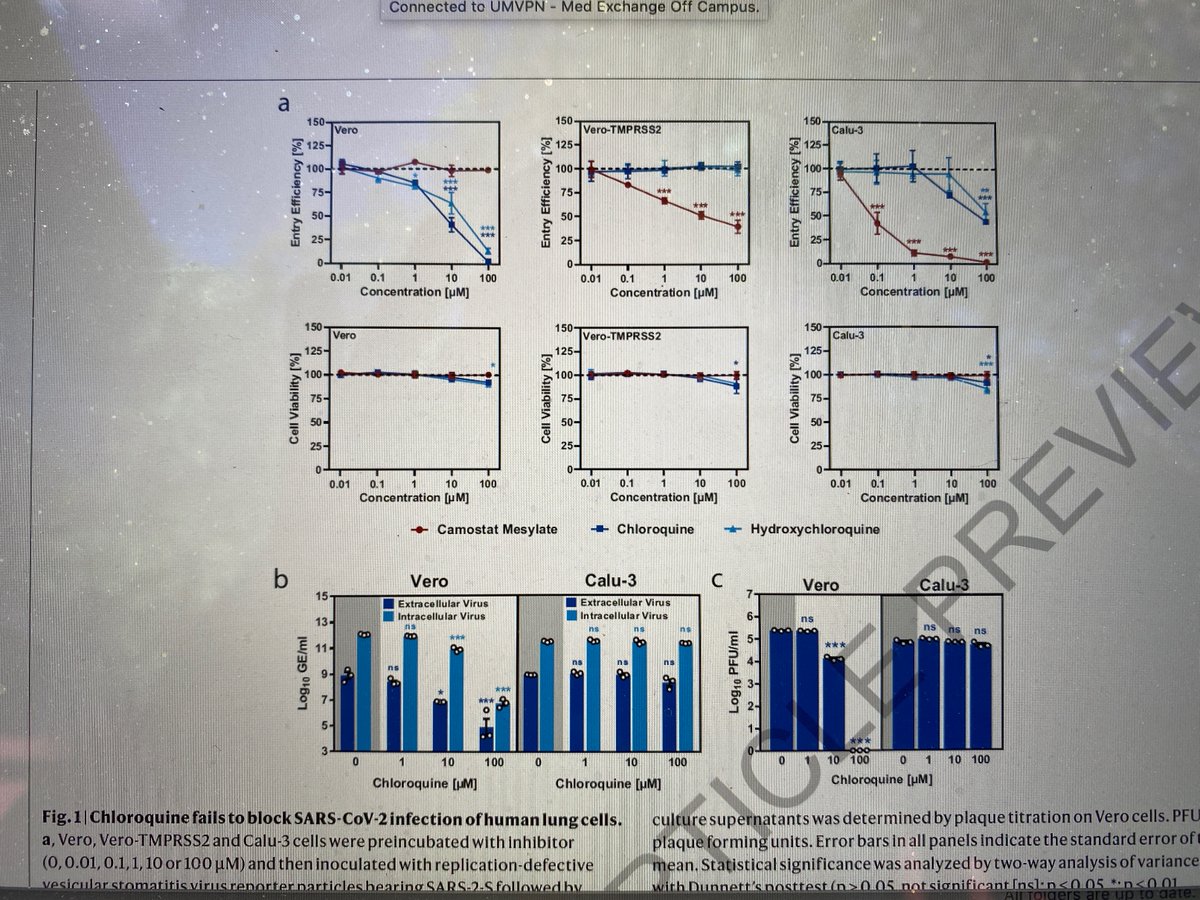
Unfortunately, in human airway epithelial cells, which express low levels of CatB/L, this pathway plays a minor role for viral entry for SARS-CoV-2. Here viral entry primarily depends on the pH-independent, plasma membrane resident serine protease TMPRSS2
Now let’s look at the same activity in human epithelial airway cells (Calu-3) cells. The pictures of interest this time are top right as well as the right pictures of "b" and "c"

As the data show, (H)CQ fails to show a meaningful effect here. Conversely, an agent that inhibits TMPRSS2 (which Camostat does, red line in first figure) has significant inhibitory activity in these cells.
This lack of activity in relevant cell lines was also demonstrated in the human airway epithelium (HAE) model developed from primary nasal or bronchial cells where HCQ was not helpful in reducing the titers of SARS-CoV-2 compared to untreated controls (titers actually higher)

So HCQ fails in vitro when assessing activity against appropriate cell lines. This would often be a stop point for assessment of a drug, but since everything is backwards here we have much more to explore. Let’s next look at animal data.
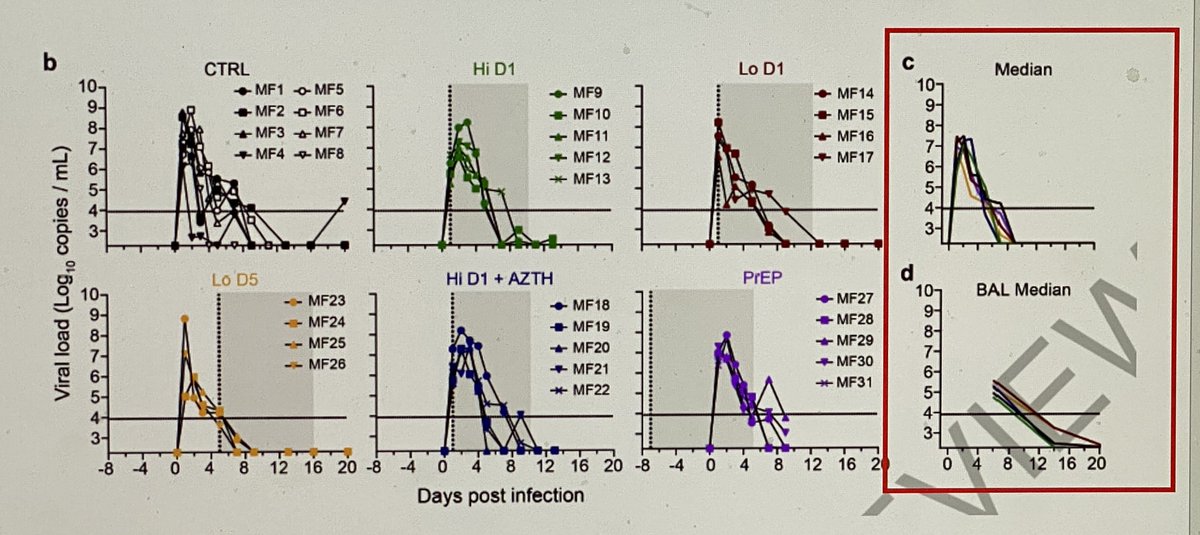
Figures show the impact of pre exposure HCQ, low/high dose early treatment, or low dose late treatment on viral kinetics in the macaque respiratory tract. Pay attention to “c” and “d” below. The control and HCQ overlap.HCQ had no impact on viral kinetics or progression of disease
So, HCQ doesn’t work in vitro in lung cells. It doesn’t work in animals as prevention or treatment. This would normally be a “don’t go” moment,but we also have placebo controlled RCTs across the spectrum(from post exposure prophy to severe disease) investigating the impact in pts
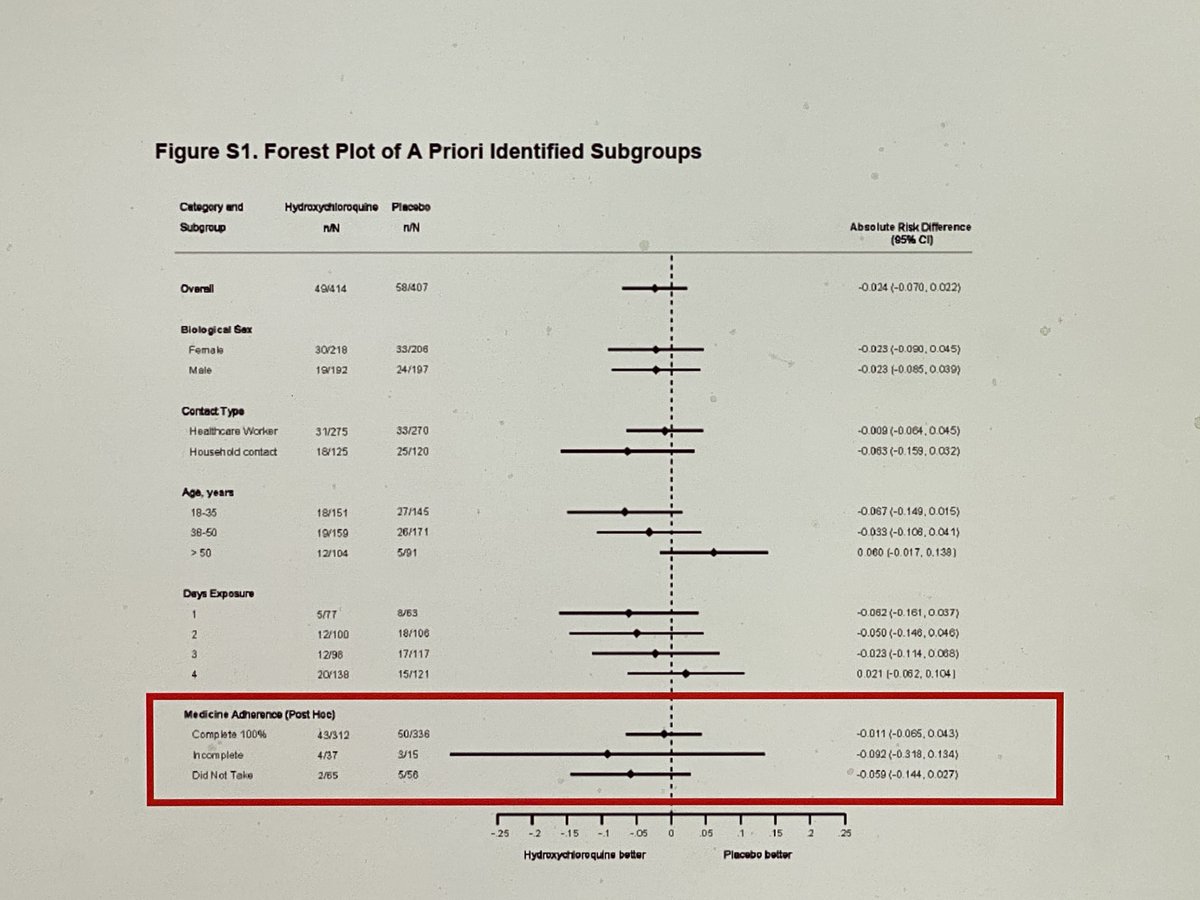
First off, post-exposure prophylaxis. The goal here would be to prevent infection and we have two studies. First one came from Boulware et al. HCQ dose was 800 mg x 1, 600 mg 6-8 hours later then 600 mg days 2-5 compared to placebo. No impact on confirmed or probable Covid-19

While some might suggest that there was a ~17% reduction (from 14.3 to 11.8 percent) that might not have been detected due to the small sample size, figure S1 refutes this. Any difference occurred in patients who did not take their study drug. HCQ is 0 for 1.
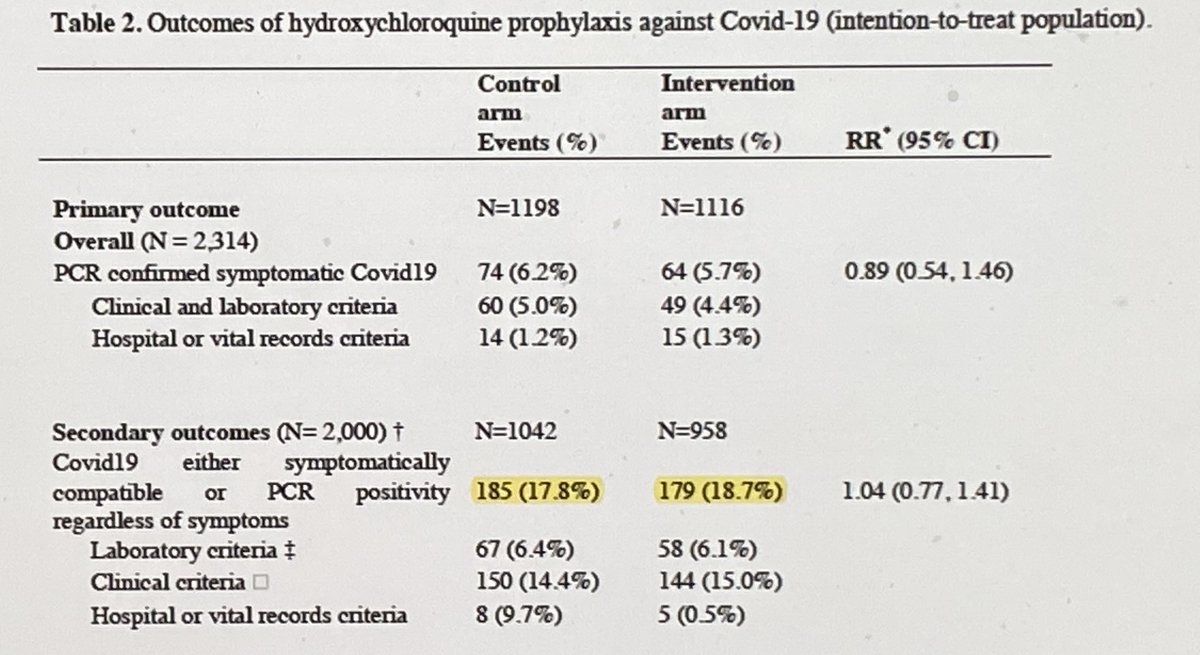
Second post exposure prophy study came out Monday as a preprint. While there are some things that will need to be addressed on peer review, I didn’t see anything that will impact the main findings. HCQ 800 mg x 1 then 400 mg/day x 6 days vs. placebo
Larger study, over 1100 patients in each arm. Primary outcome was incidence of PCR confirmed symptomatic Covid-19. Secondary outcome was incidence of PCR positivity OR symptomatic Covid-19 in those who were not PCR positive at baseline. Either way- no difference. HCQ 0 for 2.
Moving forward to early outpatient treatment for mild-moderate disease. The goal here would be primarily to stop progression of illness (the need for hospitalization or death) or lead to quicker symptom resolution. Two studies here.
First one again comes from the collaboration between the Minnesota and Canadian groups. Same dosing strategy as the post exposure prophy study and compared to placebo
Primary outcome was change in symptom score severity over 14 days (on a 0 -10 scale). No meaningful decrease with the use of HCQ. Even if this hit statistical significance, I am not sure a difference of 0.27 points on a ten-point scale would be of clinical significance.

Secondary outcomes looked at the percentage of patients with resolved symptoms at the different assessment time points (day 0, 3, 5, 10, 14) or incidence of hospitalization or death. No clinically or statistically significant difference in either endpoint
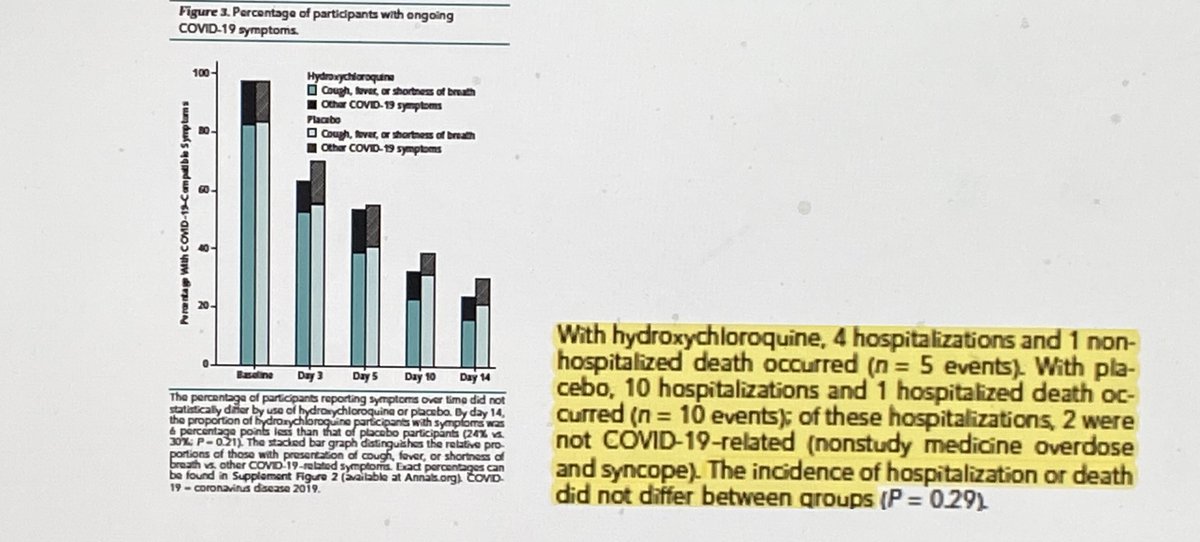
Yes, I noticed the “numerical” differences in hospitalizations/death between the two groups. The reason I do not put much stock in because it is 8 (3.7%) versus 5 (2.4%) events once we remove the non Covid-19 hospitalizations, and deaths are the same (1 vs 1). HCQ is now 0 for 3
The second early outpatient study (amazingly) came out on the same day. This was an open label comparing HCQ 800 mg x 1 then 400 mg/day x 6 days to placebo for mild Covid-19.
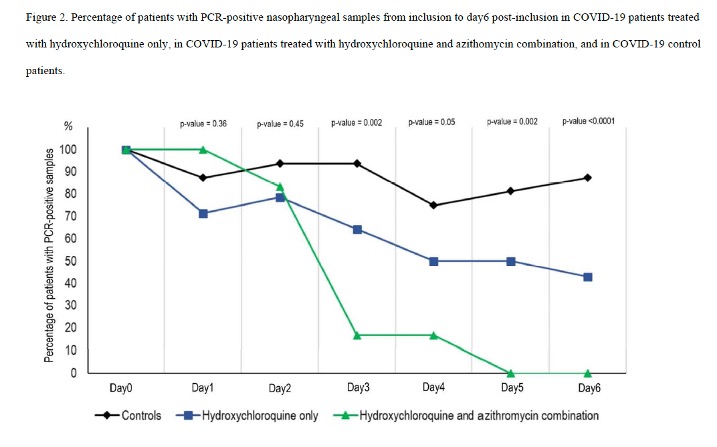
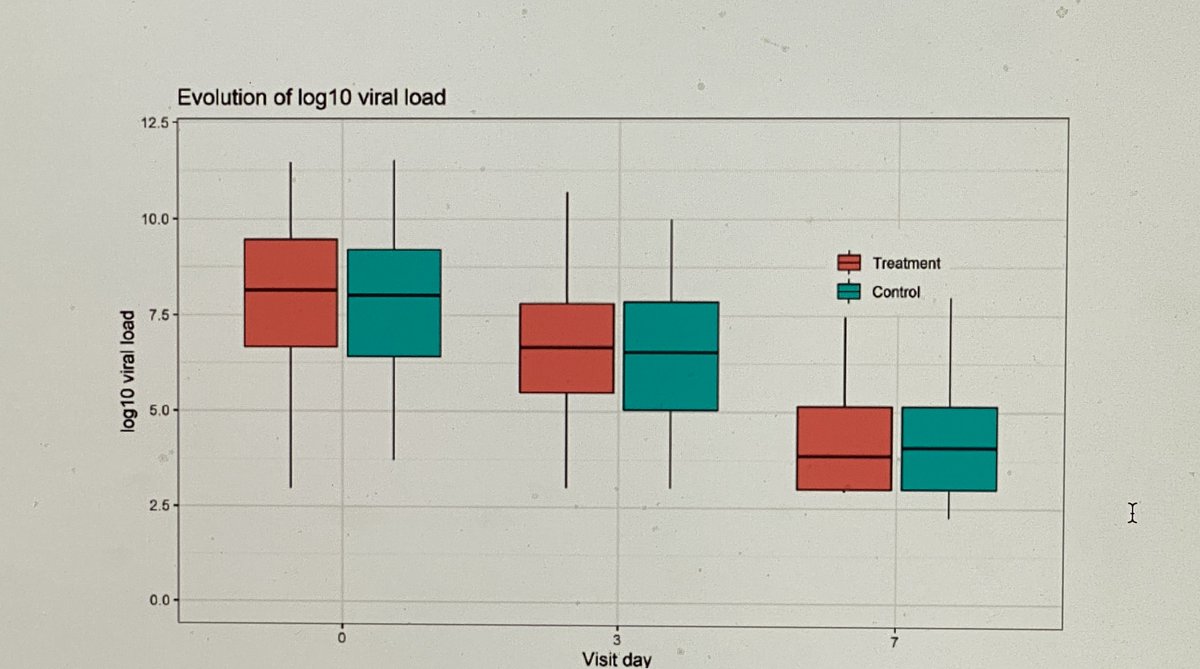
Primary endpoint here was decrease viral load in nasopharyngeal swabs over time. As the figure shows, absolutely no impact of HCQ.
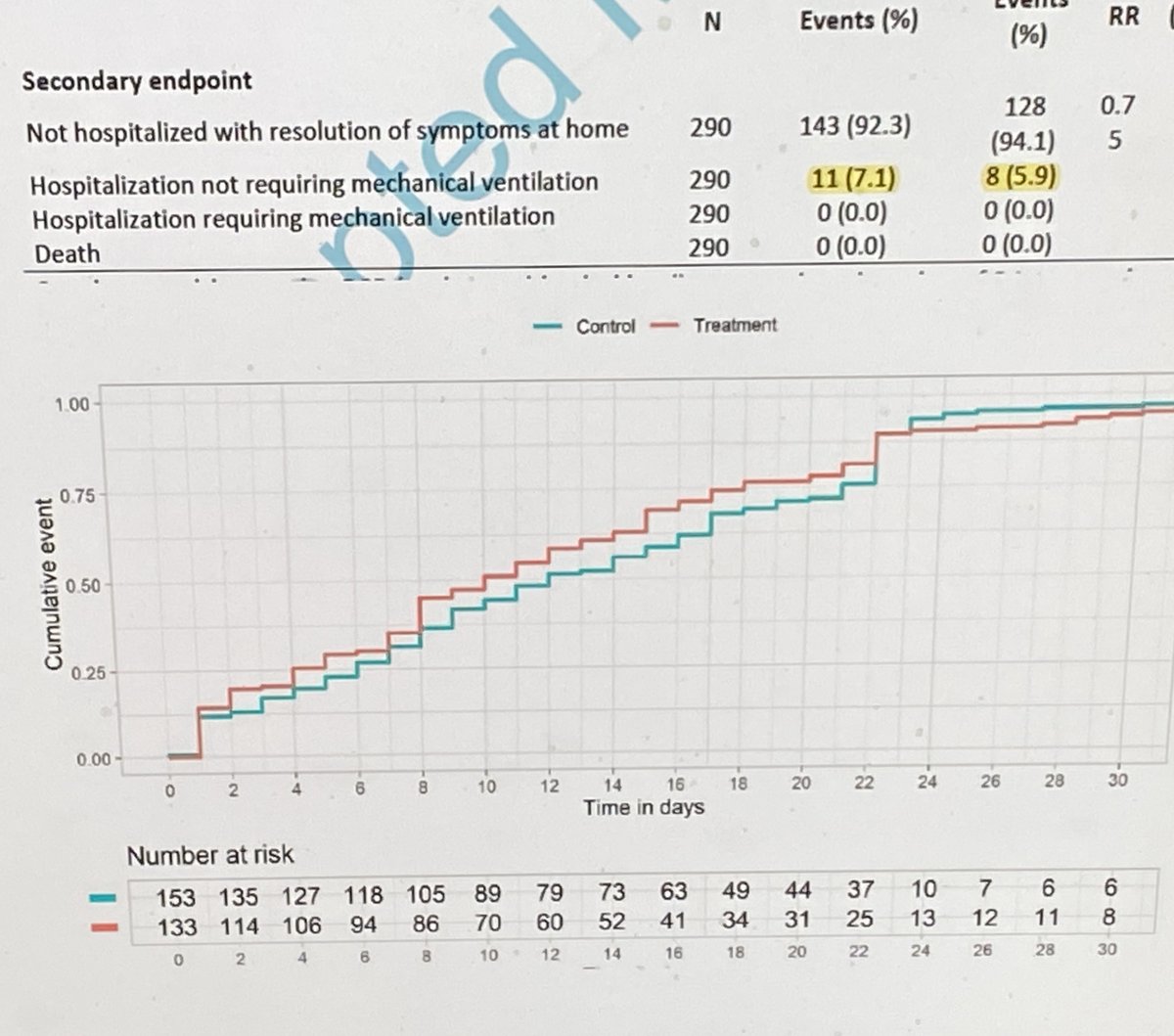
Secondary endpoints included rate of hospitalization and time until resolution of symptoms. Again, a lack of meaningful impact. 0 for 4
A quick side note here. The previous two studies included 713 patients with mild outpatient Covid-19, half of which were treated and half who got placebo. Only two of these patients (0.3%) died, one of which received HCQ and one of which received placebo
The point is that in this population, death rate is extremely low. Therefore, when you folks are pushing anecdotal evidence that they treated XX patients EARLY and none died note that even if this is a factual statement - it would be the same if they weren’t treated
Anyway, moving along the next study focuses on the next level of progression- patients hospitalized with mild-moderate illness. Three arms in this one. Standard care (SOC), SOC + HCQ 400 mg twice daily, SOC +HCQ + azithromycin 500 mg once daily for 7 days
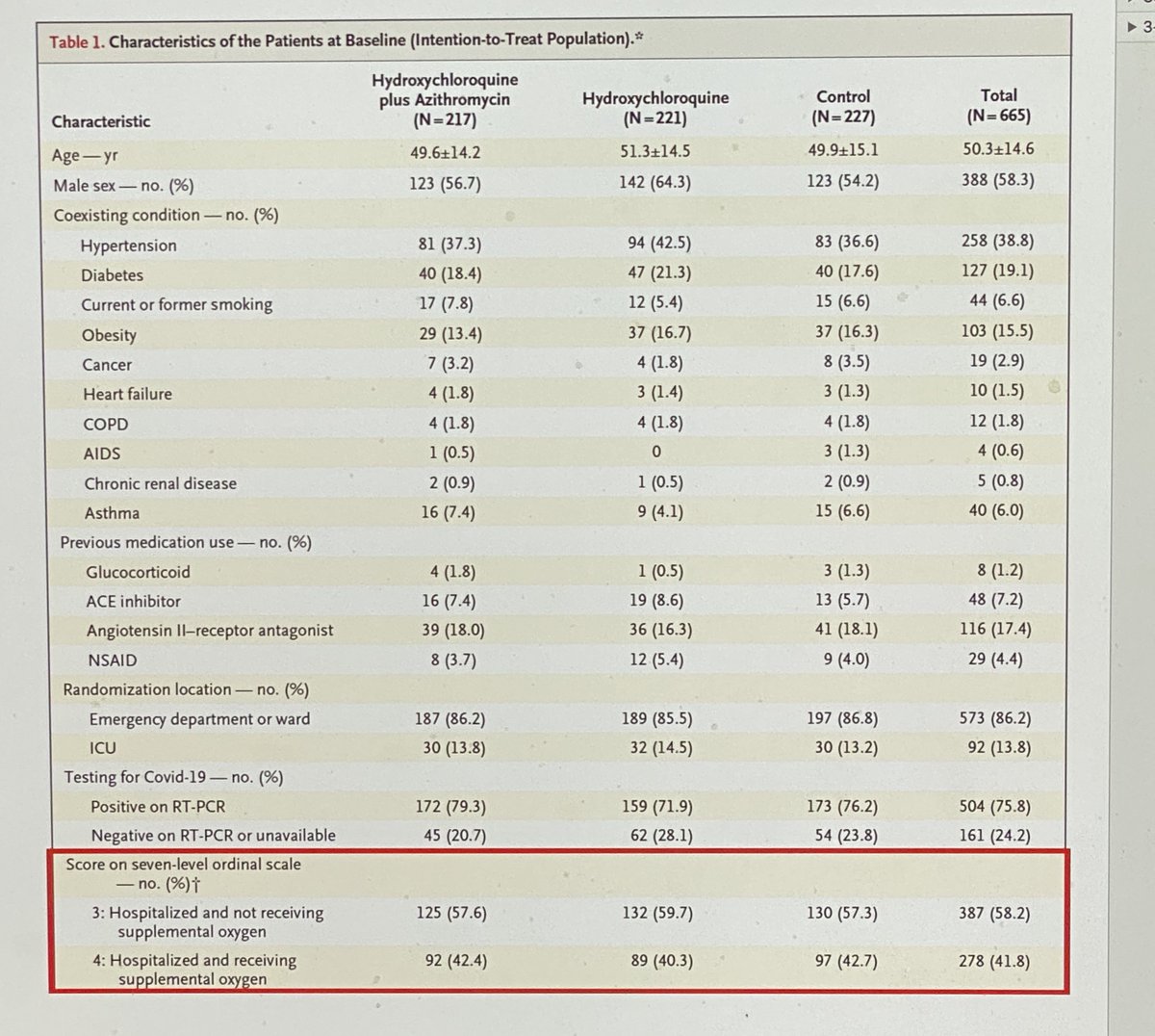
The goal here would be to stop the progression of illness and/or getting patients home faster. As you can see, baseline these groups were similar. About 60% not requiring supplemental oxygen, and 40% requiring it across the three groups (n ~ 220 in each treatment group)
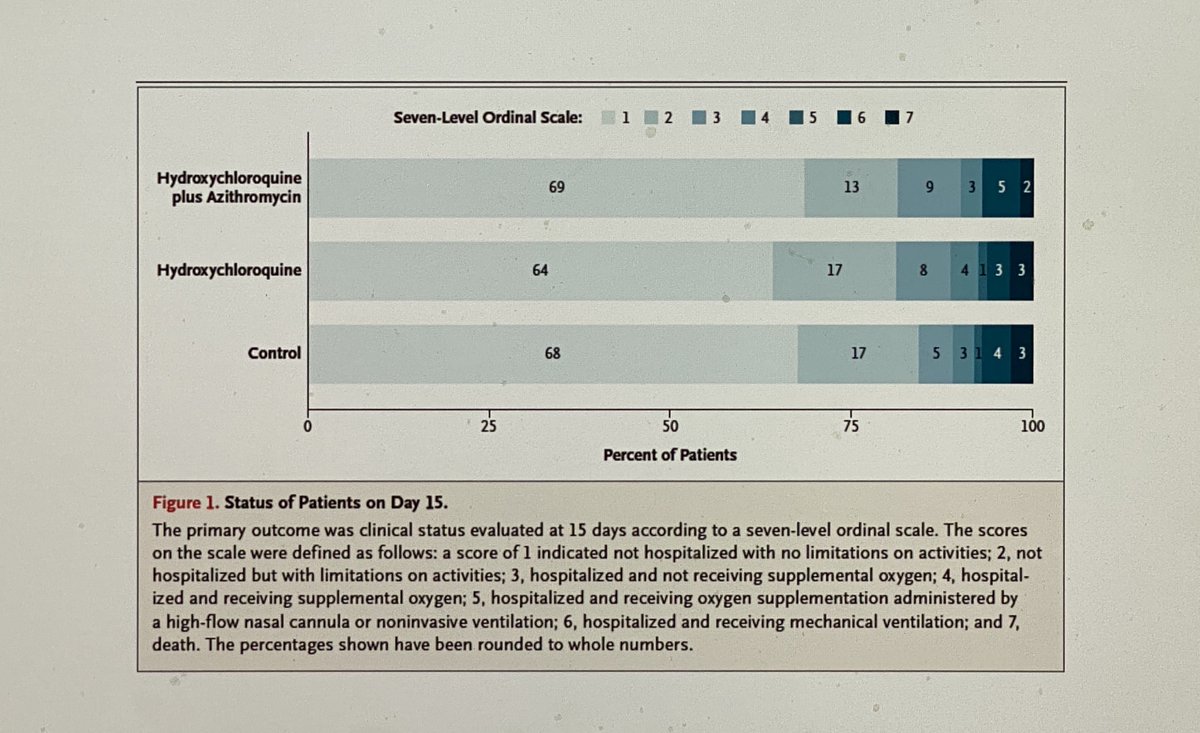
Primary outcome was clinical status on an ordinal scale at day 15 (should look familiar to you from the #remdesivir trials). As you can see – no impact of HCQ or HCQ + AZ when compared to placebo.
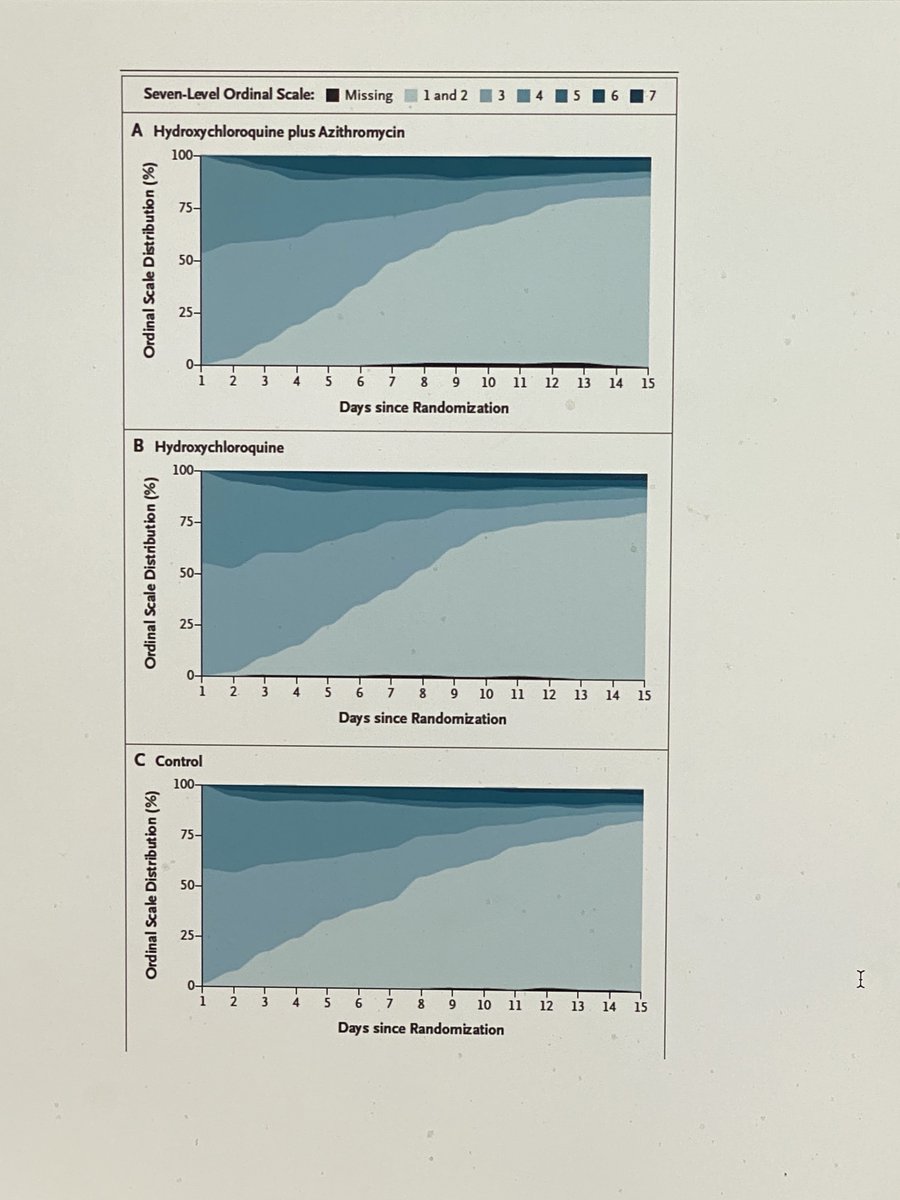
Looking at clinical outcomes over time you see similar pace of improvement across the three groups
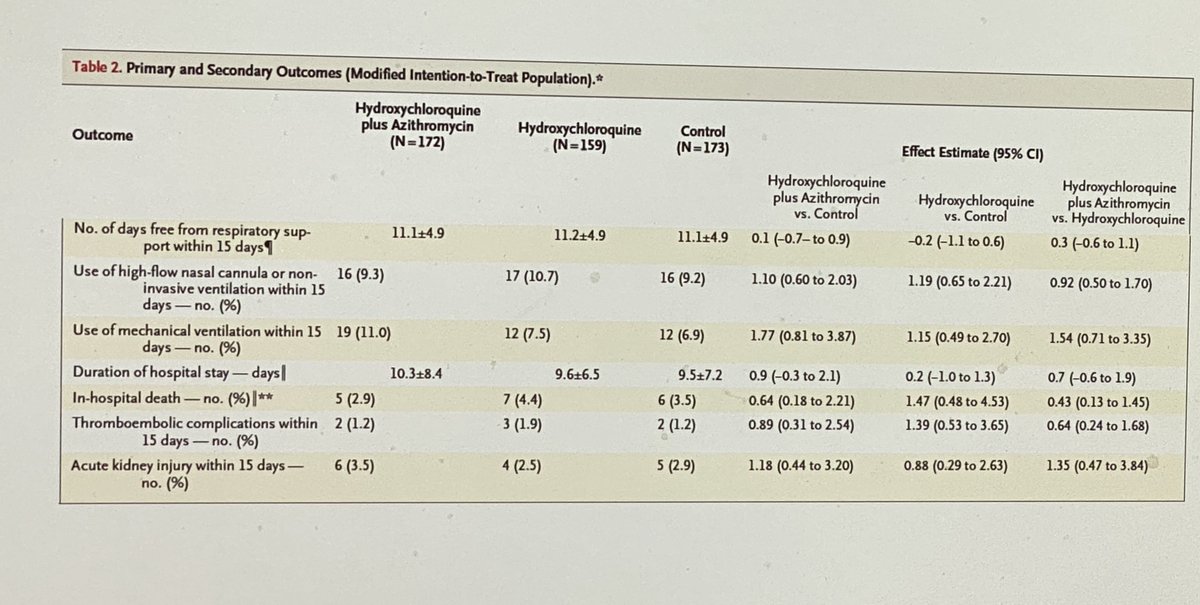
Other key secondary outcomes look similar. No difference in need for high flow or mechanical ventilation, length of stay, or in hospital death. That’s zero out of five for HCQ for those of you scoring at home.
This leads to the final step in the progression of Covid-19. Sicker inpatients. RECOVERY investigates this question. Over 6000 patients. Aggressive HCQ dosing – 800 mg at time zero and 6 hours then 400 mg q12. If this dose fails, there is unlikely to be an efficacious dose.
And unfortunately, across the board we see no impact of HCQ versus untreated controls. No benefit in patients on room air, those on supplemental oxygen, nor those mechanically ventilated. That’s 0 for 6- across the whole spectrum of disease.

Additionally, two other RCTs, the Solidarity trial who.int/news-room/deta… and the ORCHID trial nih.gov/news-events/ne… have been stopped for futility.
So, there you have it. It fails in vitro (once the right cells are used), in animal models, and across the spectrum of disease in patients. There is no conspiracy. Just, unfortunately, an ineffective drug. (End)