Lots of talk about “skipping the phase III” trials of #COVID19 #vaccines and going straight to widespread vaccination.
Here’s a not-so-brief thread on why that’s a terrible idea.
1/
Here’s a not-so-brief thread on why that’s a terrible idea.
1/
Ethical considerations aside, there are several reasons we *need* phase 3 trials as part of a developing COVID vaccines:
* Prove Efficacy
* Ensure Safety
* Conserve Limited resources
* Preserve Public confidence
2/
* Prove Efficacy
* Ensure Safety
* Conserve Limited resources
* Preserve Public confidence
2/
Efficacy
Despite efforts to develop vaccines against other coronaviruses (SARS, MERS) we haven’t yet succeeded
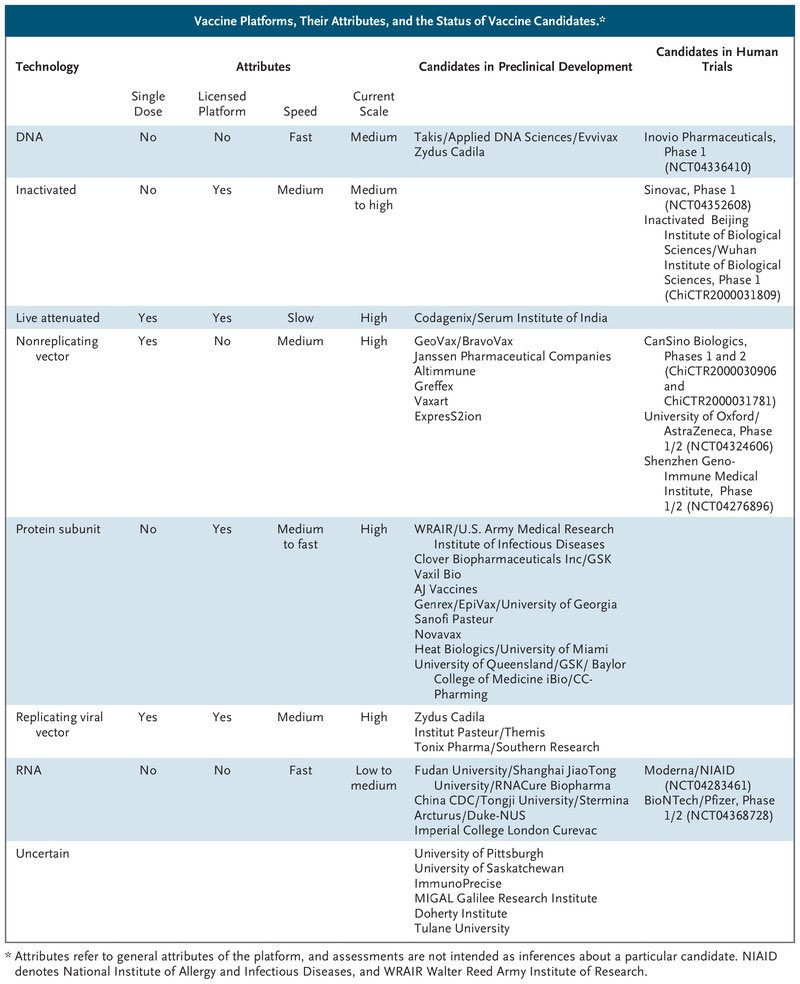
Against SARS-CoV2 we are trying a myriad of strategies: mRNA, recombinant, viral vectors, inactivated, etc. We hope one will succeed, but we don’t yet know which one
3/
Despite efforts to develop vaccines against other coronaviruses (SARS, MERS) we haven’t yet succeeded
Against SARS-CoV2 we are trying a myriad of strategies: mRNA, recombinant, viral vectors, inactivated, etc. We hope one will succeed, but we don’t yet know which one
3/
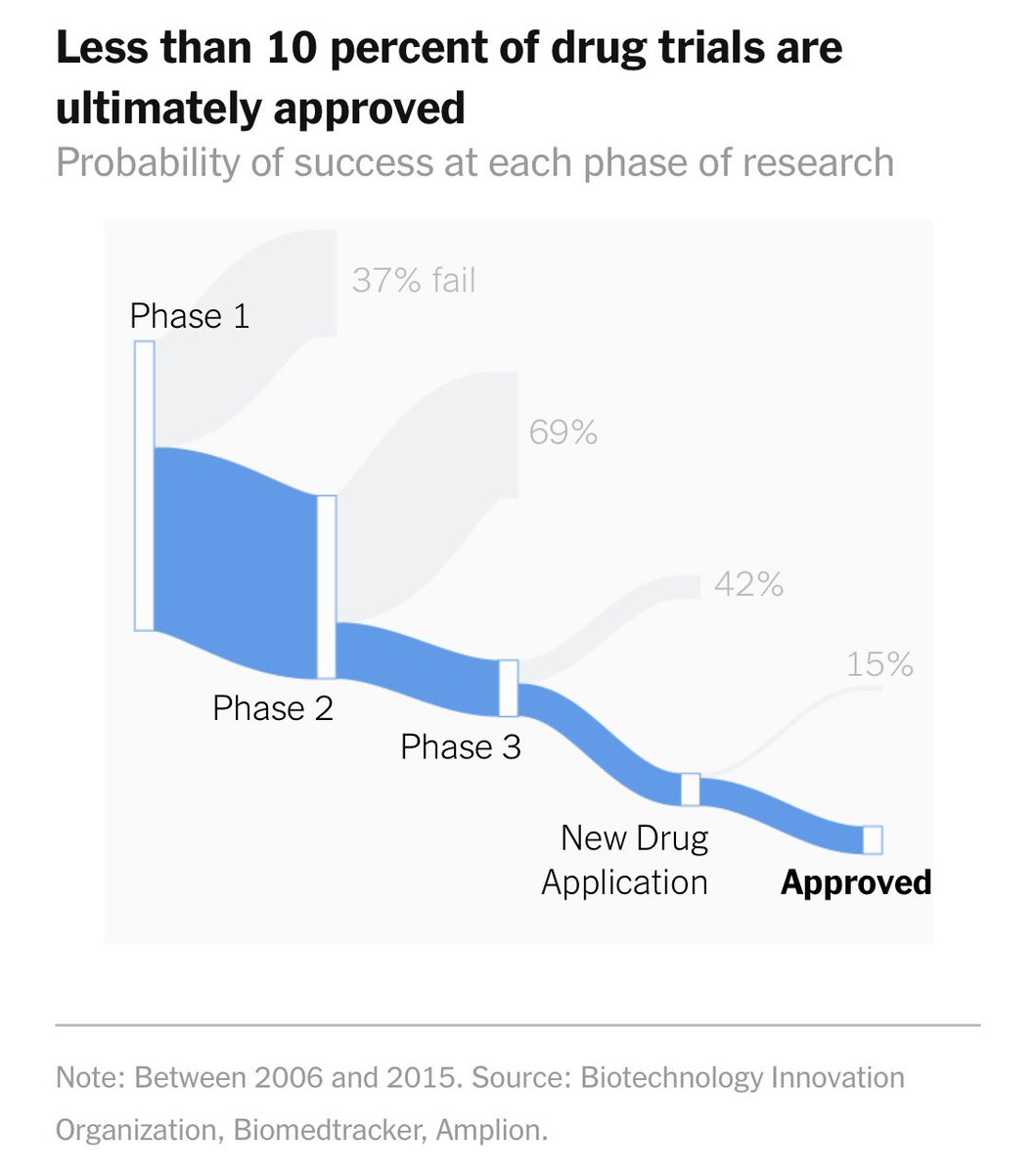
Most new therapeutics don’t succeed in development. Much of this selection occurs early, but as this Sankey diagram from @nytimes @stuartathompson shows, almost half of new drugs fail while in phase 3.
nytimes.com/interactive/20…
4/
nytimes.com/interactive/20…
4/
Turning to vaccines. No mRNA vaccine has ever been successfully developed.
Pre-clinical efficacy (producing antibodies) does not ensure clinical efficacy, and unfortunately there is ample precedent for promising vaccines to fail in phase III.
5/
Pre-clinical efficacy (producing antibodies) does not ensure clinical efficacy, and unfortunately there is ample precedent for promising vaccines to fail in phase III.
5/
For example, a promising HIV vaccine failed due to lack of efficacy after a n=3000 phase 3 trial.
ncbi.nlm.nih.gov/pmc/articles/P…
Similarly, several promising RSV vaccines have failed to reach an efficacy endpoint in phase III trials
pubmed.ncbi.nlm.nih.gov/27903593/
6/
ncbi.nlm.nih.gov/pmc/articles/P…
Similarly, several promising RSV vaccines have failed to reach an efficacy endpoint in phase III trials
pubmed.ncbi.nlm.nih.gov/27903593/
6/
Furthermore, with multiple candidate COVID vaccines, we need Phase III results to choose between them. Without phase III data we could easily mass produce the less effective (or ineffective) vaccine.
7/
7/
Getting this wrong would be catastrophic.
Widespread administration of an ineffective vaccine could increase risk taking behaviors, potentially making the pandemic worse.
It would also make it difficult (or impossible) to enroll further studies.
8/
Widespread administration of an ineffective vaccine could increase risk taking behaviors, potentially making the pandemic worse.
It would also make it difficult (or impossible) to enroll further studies.
8/
Safety
Vaccine safety is not a mere technicality. Approved vaccines are extremely safe precisely because they go through rigorous late stage testing.
Though rare, serious safety signals have been uncovered in late stage trials.
9/
Vaccine safety is not a mere technicality. Approved vaccines are extremely safe precisely because they go through rigorous late stage testing.
Though rare, serious safety signals have been uncovered in late stage trials.
9/
This @US_FDA report outlines 22 case studies of therapies that appeared promising after phase II but failed in phase III (including 5 vaccines).
Most fail for efficacy, however, the greatest fear is that a novel vaccine could actually worsen #COVID19
fda.gov/media/102332/d…
10/
Most fail for efficacy, however, the greatest fear is that a novel vaccine could actually worsen #COVID19
fda.gov/media/102332/d…
10/
For example, Merck’s V710 vaccine against s. aureus not only failed at reducing post-op infections it actually *increased* risk of multi-organ failure & death among those who acquired staph infection in the vaccine group compared to placebo.
pubmed.ncbi.nlm.nih.gov/25483690/
11/
pubmed.ncbi.nlm.nih.gov/25483690/
11/
#Antibody dependent enhancement (ADE) is a phenomenon whereby low titers of antibody can potentiate viral infection, potentially *exacerbating* disease.
ADE has been a challenge in developing vaccines against other viruses, such as #Dengue virus.
ncbi.nlm.nih.gov/pmc/articles/P…
ADE has been a challenge in developing vaccines against other viruses, such as #Dengue virus.
ncbi.nlm.nih.gov/pmc/articles/P…
The risk of ADE in human coronavirus is uncertain, and is probably low.
But in a disease like #COVID with such prominent immune pathology we should be cautious, especially since Vaccines against Feline Coronaviruses have been shown to exacerbate inflammation via ADE.
13/
But in a disease like #COVID with such prominent immune pathology we should be cautious, especially since Vaccines against Feline Coronaviruses have been shown to exacerbate inflammation via ADE.
13/
Although lack of efficiency is probably the biggest risk, given the potential hazard of ADE (and other adverse effects), its crucial to verify safety before proceeding with widespread vaccination.
14/
14/
Wasting resources
Vaccinating 330 million Americans will be a momentous logistical challenge.
Some vaccines require 2 injections a mo apart.
Manufacturing, shipping, & administering 2/3 of a billion doses is non-trivial. Imagine screwing it up and having to do it twice?
15/
Vaccinating 330 million Americans will be a momentous logistical challenge.
Some vaccines require 2 injections a mo apart.
Manufacturing, shipping, & administering 2/3 of a billion doses is non-trivial. Imagine screwing it up and having to do it twice?
15/
• • •
Missing some Tweet in this thread? You can try to
force a refresh