Follow-on explanation from RSS statement
Fair questions about the actual figures used, and how this fits with repeated cheap testing as proposed by Michael Mina and others.
Key is that the Mina proposals (and Moonshot) only look at one side of the coin - the benefits
1/10
Fair questions about the actual figures used, and how this fits with repeated cheap testing as proposed by Michael Mina and others.
Key is that the Mina proposals (and Moonshot) only look at one side of the coin - the benefits
1/10
Moonshot does not consider the harms that mass testing will do through false positives.
In screening you always need to balance the benefits (the true positives) against the harms (mainly false positives)
So what determines how many false positives there will be?
2/10
In screening you always need to balance the benefits (the true positives) against the harms (mainly false positives)
So what determines how many false positives there will be?
2/10
Key figures that matter:
1)Prevalence of COVID
2)Specificity
An illustration - bear with my assumptions.
~3,000 cases in UK detected per day at the moment
National rate is 5 per 100,000
Double to allow for undetected asymptomatics –
Real rate of 10 per 100,000
3/10
1)Prevalence of COVID
2)Specificity
An illustration - bear with my assumptions.
~3,000 cases in UK detected per day at the moment
National rate is 5 per 100,000
Double to allow for undetected asymptomatics –
Real rate of 10 per 100,000
3/10
Spreadsheet looks at numbers of TP and FP
for tests with 60%. 80% and (dream on) 100% sensitivity
and 99% specificity (so 1% false positives)
Highlighted row shows true and false positives when prevalence is 10 per 100,000
You can see sensitivity doesn't really matter
4/10
for tests with 60%. 80% and (dream on) 100% sensitivity
and 99% specificity (so 1% false positives)
Highlighted row shows true and false positives when prevalence is 10 per 100,000
You can see sensitivity doesn't really matter
4/10
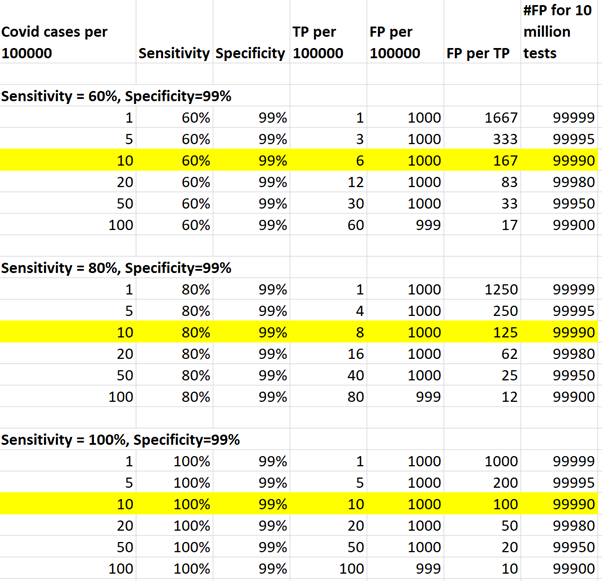
For every true case detected there will be between 100 and 170 false positives.
Testing 10 million a day there would be 100,000 false positives.
In a week, that would be 600,000 (we will rest on Sundays), the population of Sheffield (sorry Sheffield for picking on you).
5/10
Testing 10 million a day there would be 100,000 false positives.
In a week, that would be 600,000 (we will rest on Sundays), the population of Sheffield (sorry Sheffield for picking on you).
5/10
What happens to these people? What happens to their close contacts?
These are the harmful consequences that are omitted from all thinking for Moonshot.
We could test them again with another PCR test, but we can’t really do 200,000 PCR tests a day at the moment anyway
6/10
These are the harmful consequences that are omitted from all thinking for Moonshot.
We could test them again with another PCR test, but we can’t really do 200,000 PCR tests a day at the moment anyway
6/10
And we will do it all go through it again next week, and the week after, and the week after ....
7/10
7/10
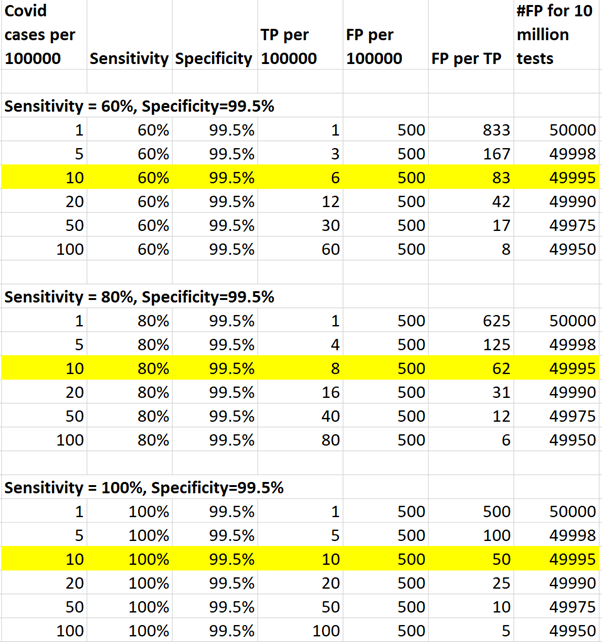
Reducing false positives (increasing specificity) is the only way to improve this. Halve false positives to 0.5% and the harms will halve.
8/10
8/10
SO Mina and Moonshot are right that tests with any sensitivity can catch disease and help, and the more times you use them the more they will catch
but they are wrong in ignoring the accumulating harms that will occur with every repeat of testing.
9/10
but they are wrong in ignoring the accumulating harms that will occur with every repeat of testing.
9/10
Establishing specificity of these tests when used in the community is essential to get a grip on how big the problem would be.
Not the values from the cleanest most professional laboratory setting, but when they are used at home.
Is only 1% false positive optimistic?
10/10
Not the values from the cleanest most professional laboratory setting, but when they are used at home.
Is only 1% false positive optimistic?
10/10
• • •
Missing some Tweet in this thread? You can try to
force a refresh