On 9/11/01 I was a senior in high school in Brooklyn. I had a front row seat as planes flew into the WTC, murdering thousands & altering the course of our country
19 years later as an ICU doctor I have again been on the front lines bearing witness to another historic disaster
1/
19 years later as an ICU doctor I have again been on the front lines bearing witness to another historic disaster
1/
2977 people died on 9/11.
Every week for the last 24, more people have died from coronavirus.
This month we pass yet another grim milestone as over two hundred thousand Americans have died in the pandemic.
But the death toll alone doesn't capture the enormity of the crisis.
2/
Every week for the last 24, more people have died from coronavirus.
This month we pass yet another grim milestone as over two hundred thousand Americans have died in the pandemic.
But the death toll alone doesn't capture the enormity of the crisis.
2/
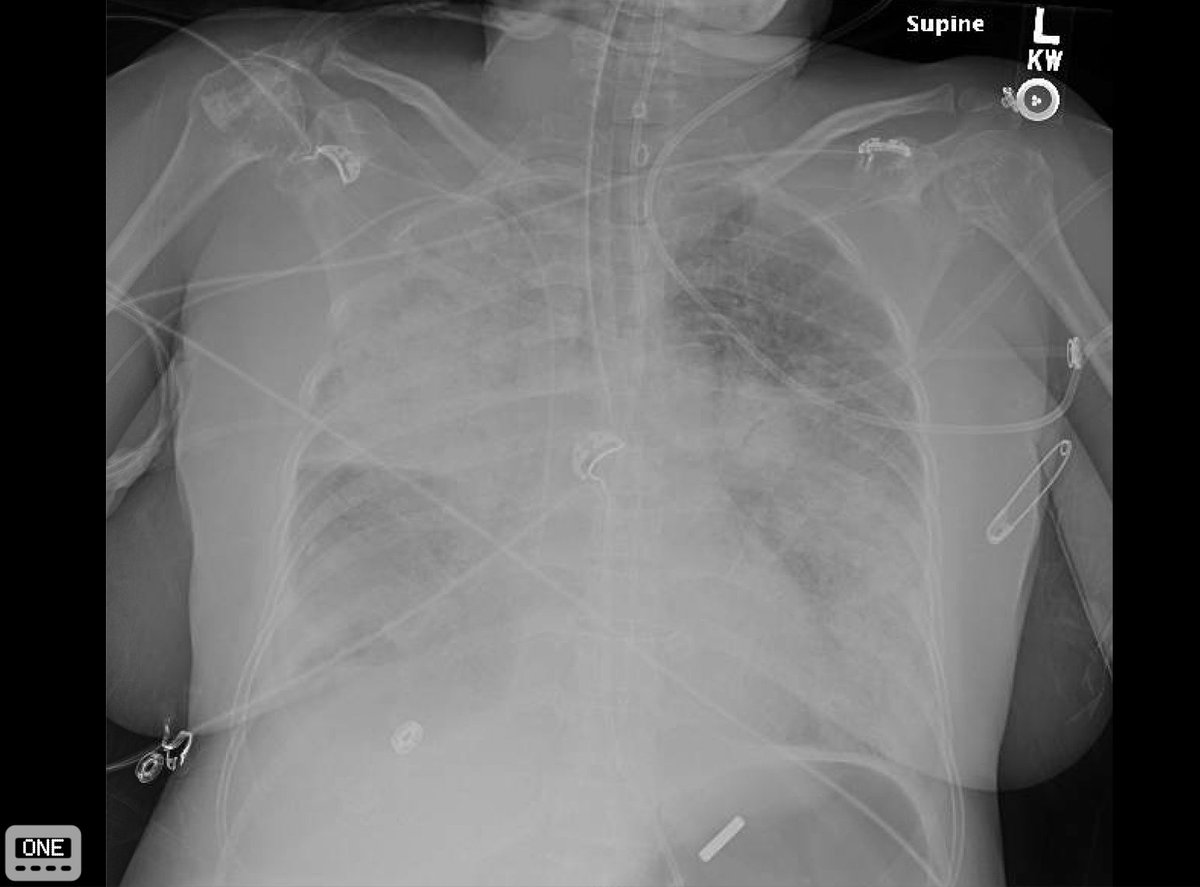
Even in the ICU, where we care for the sickest people with COVID19, most patients survive.
Over the last 6 months we’ve made progress & gotten better at treating COVID19.
But based on our experience with ARDS, many survivors of severe COVID19 will not recovery completely.
3/
Over the last 6 months we’ve made progress & gotten better at treating COVID19.
But based on our experience with ARDS, many survivors of severe COVID19 will not recovery completely.
3/
If we continue our present course millions will be infected & hundreds of thousands more will die this year.
If we had made better policy choices, we could have averted many, perhaps most, of these deaths.
But it's not too late to start making good choices.
Here are 10 ideas.
4/
If we had made better policy choices, we could have averted many, perhaps most, of these deaths.
But it's not too late to start making good choices.
Here are 10 ideas.
4/
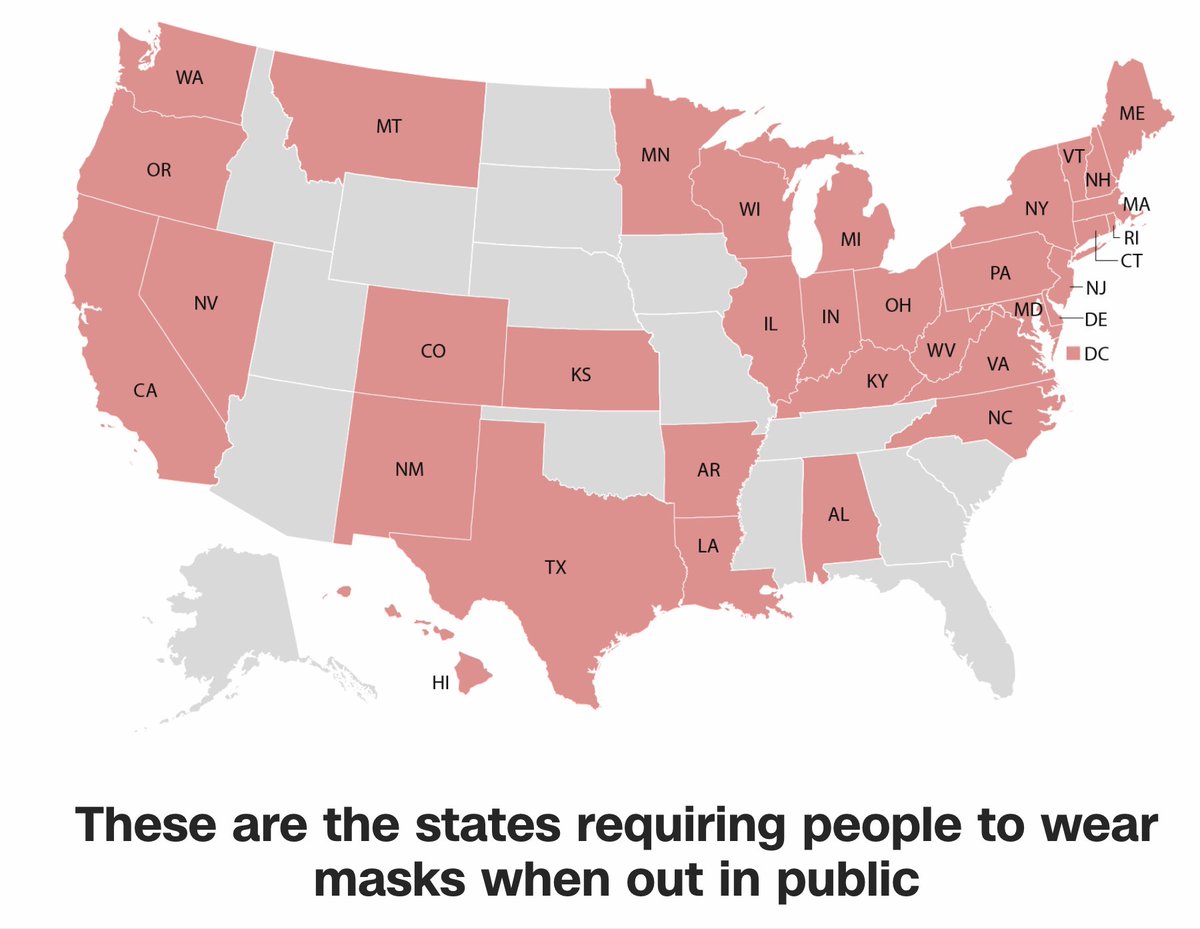
1. National Mask Mandate
COVID is airborne.
Masks are the *most* effective intervention we have, yet our national policy has been inconsistent.
An analysis in PNAS found that mask wearing was likely the biggest determinant of pandemic outcomes.
bit.ly/3hhf9bJ
5/
COVID is airborne.
Masks are the *most* effective intervention we have, yet our national policy has been inconsistent.
An analysis in PNAS found that mask wearing was likely the biggest determinant of pandemic outcomes.
bit.ly/3hhf9bJ
5/

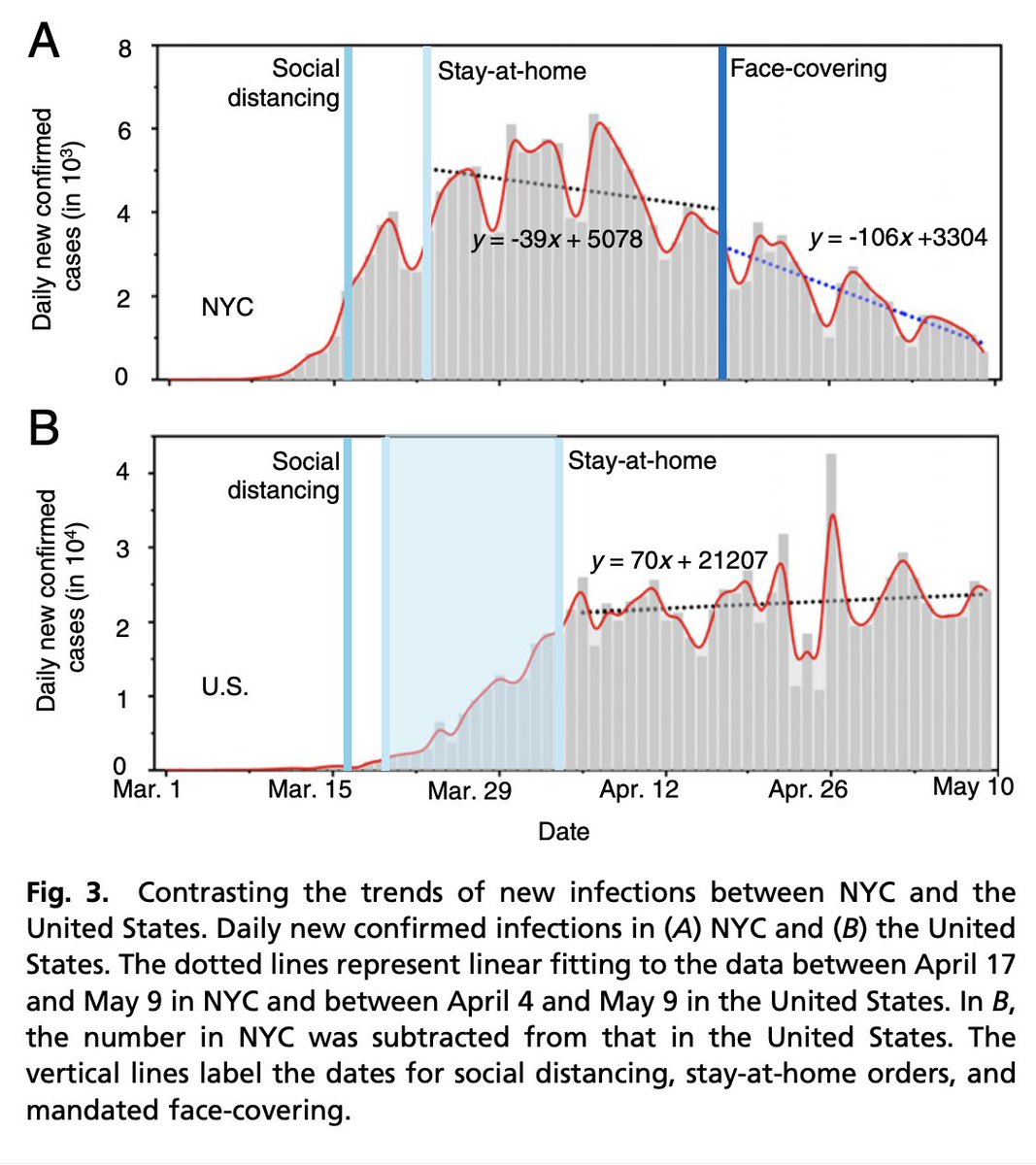
At present, 15 states do not require masks in public. This can and should change. cnn.it/2ReyWOB
@IHME_UW estimates that 410,000 Americans will die from COVID by the end of 2020. With universal masking, they estimate that we could save 122,000 lives.
6/
@IHME_UW estimates that 410,000 Americans will die from COVID by the end of 2020. With universal masking, they estimate that we could save 122,000 lives.
6/

2.Restrict large gatherings
Again and again we’ve seen super-spreader events greatly increase the number of cases.
The Sturgis Rally in SD last month is estimated to have led to 253,000 additional COVID cases. This needs to stop.
7/
Again and again we’ve seen super-spreader events greatly increase the number of cases.
The Sturgis Rally in SD last month is estimated to have led to 253,000 additional COVID cases. This needs to stop.
https://twitter.com/nickmmark/status/1303200134633644033?s=20
7/
Restricting large indoor gatherings does not mean no social events. It does force us to rethink *how* we have them.
Groups have found creative ways to hold concerts, meetings, religious services, & other gatherings outdoors with masks & social distancing precautions.
8/
Groups have found creative ways to hold concerts, meetings, religious services, & other gatherings outdoors with masks & social distancing precautions.
8/
Each state is different & there probably isn’t a one size fits all solution, but we do need NATIONAL STANDARDS.
As we’ve seen, South Dakota’s lax policies led to a resurgence of cases throughout the US.
With evidence based guidelines we can prevent this from happening again.
9/
As we’ve seen, South Dakota’s lax policies led to a resurgence of cases throughout the US.
With evidence based guidelines we can prevent this from happening again.
9/
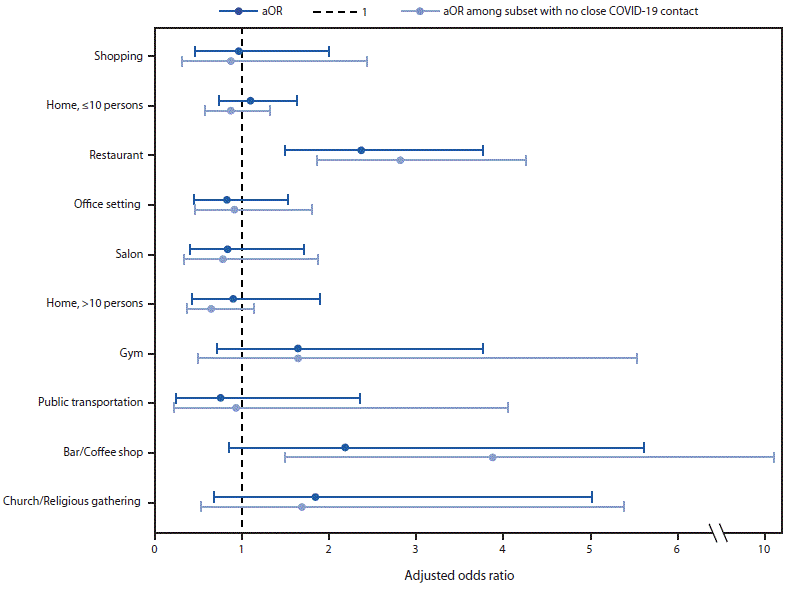
3.Safer restaurants
This week CDC MMWR reports that restaurant dining is one of the biggest risk factors for acquiring COVID. bit.ly/2RlLQu1
This is soluble: Take out is best.🥡
Also evidence based rules for (outdoor) table spacing, party size, etc.
10/
This week CDC MMWR reports that restaurant dining is one of the biggest risk factors for acquiring COVID. bit.ly/2RlLQu1
This is soluble: Take out is best.🥡
Also evidence based rules for (outdoor) table spacing, party size, etc.
10/

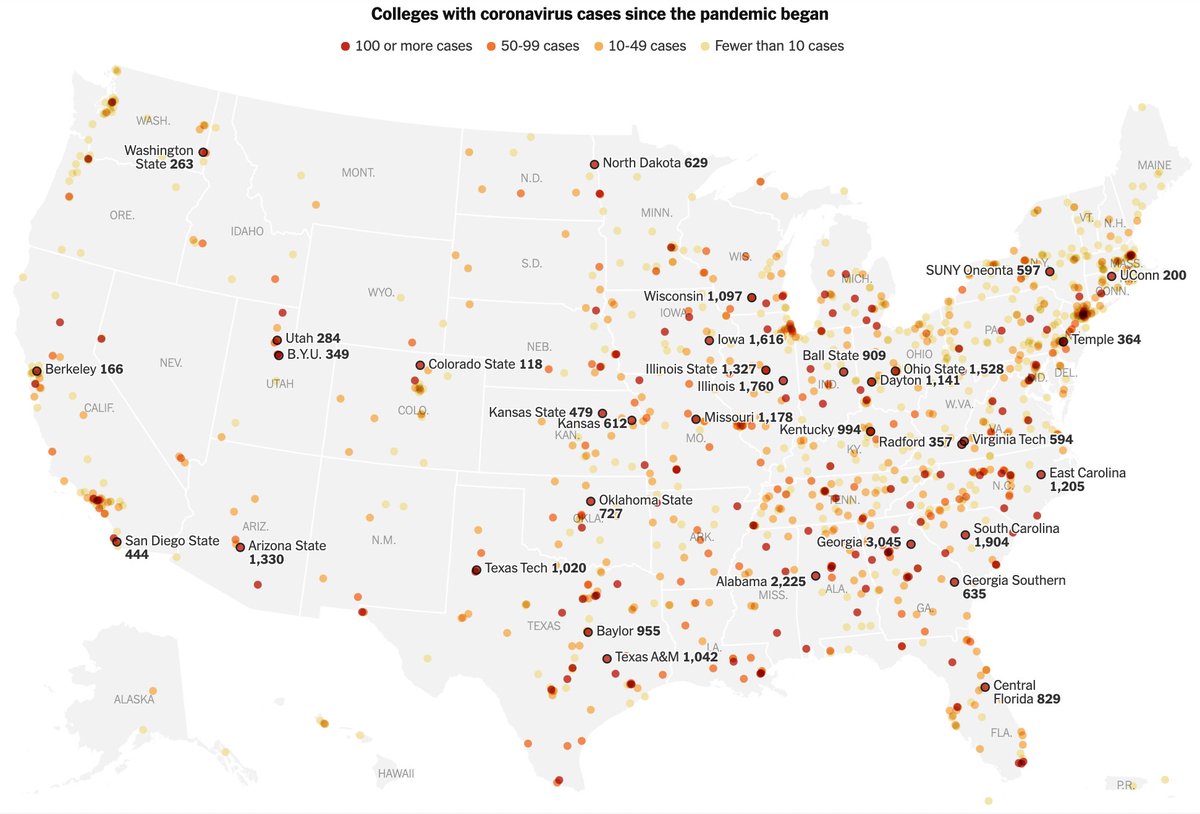
4.Pause school reopening
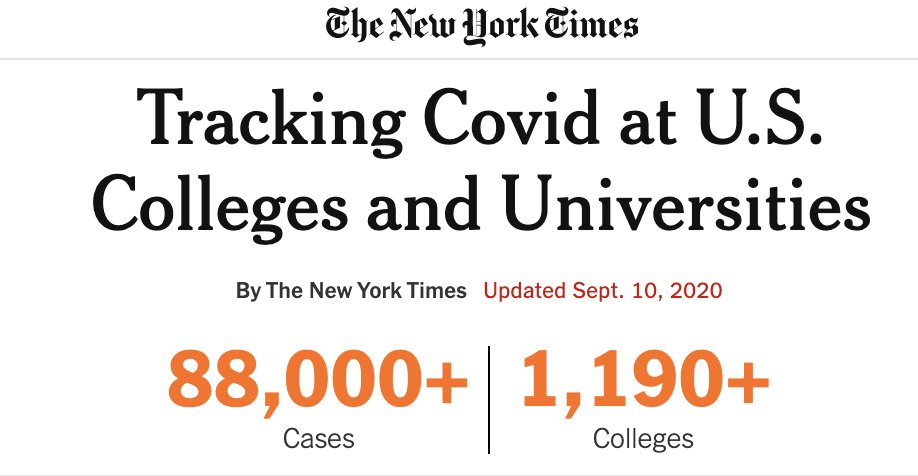
Re-opening schools has been a disaster:
*There are outbreaks in schools & universities in *every* state
*Almost 90,000 cases on university campuses. nyti.ms/2Fwj4UT
*At least 3 deaths of young teachers from COVID19.
abcn.ws/35tc5ab
11/
Re-opening schools has been a disaster:
*There are outbreaks in schools & universities in *every* state
*Almost 90,000 cases on university campuses. nyti.ms/2Fwj4UT
*At least 3 deaths of young teachers from COVID19.
abcn.ws/35tc5ab
11/
In many cases this was predictable: inadequate planning, testing, & PPE coupled with high density indoor activities.
But even ostensibly well prepared and well equipped schools have failed to contain the virus as illustrated by this @nytimes article:
nytimes.com/2020/09/10/hea…
12/
But even ostensibly well prepared and well equipped schools have failed to contain the virus as illustrated by this @nytimes article:
nytimes.com/2020/09/10/hea…
12/
Unchecked, COVID transmission in schools will lead to another massive wave of community infections. We must suspend in person classes in areas/schools with incipient outbreaks.
This was the case in 1919 and it’s true again in 2020.
to.pbs.org/32hwzkf
13/
This was the case in 1919 and it’s true again in 2020.
to.pbs.org/32hwzkf
13/
In person instruction in schools and universities is undeniably valuable. Education will suffer if we move teaching online.
But we are in the midst of a pandemic.
Until we have sufficient PPE & tests, we need to shut down in-person instruction where there are outbreaks.
14/
But we are in the midst of a pandemic.
Until we have sufficient PPE & tests, we need to shut down in-person instruction where there are outbreaks.
14/
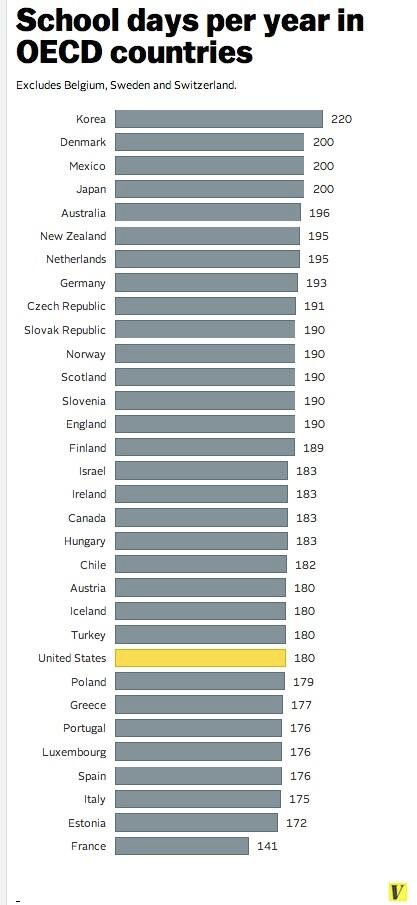
For those worried about how much ground students have already lost, consider this:
The US has fewer school days than most industrialized nations. <1% of students work on farms.
Maybe we can pay teachers more and finally move away from the 180 day agrarian school calendar…?
15/
The US has fewer school days than most industrialized nations. <1% of students work on farms.
Maybe we can pay teachers more and finally move away from the 180 day agrarian school calendar…?
15/
7.More Testing
In the first weeks of the pandemic we couldn’t get prompt COVID test results. Things still aren’t fixed.
Despite more testing kits, other shortages stymie testing: currently a lack of pipette tips and other reagents.
nytimes.com/2020/07/23/hea…
16/
In the first weeks of the pandemic we couldn’t get prompt COVID test results. Things still aren’t fixed.
Despite more testing kits, other shortages stymie testing: currently a lack of pipette tips and other reagents.
nytimes.com/2020/07/23/hea…
16/
How many tests per day do we actually need? It turns out we have no idea.
Estimates for how many daily COVID tests are needed range from 430k to 23m.
kff.org/policy-watch/w…
17/
Estimates for how many daily COVID tests are needed range from 430k to 23m.
kff.org/policy-watch/w…
17/
Eight months in we need a national strategy for testing.
At a minimum we need enough test to enable results in 24 hours. In hospitals we need rapid 1 hr testing so we can appropriately triage admissions and enroll ED patients in tele-monitoring.
18/
https://twitter.com/SenSchumer/status/1304149274675105792?s=20
At a minimum we need enough test to enable results in 24 hours. In hospitals we need rapid 1 hr testing so we can appropriately triage admissions and enroll ED patients in tele-monitoring.
18/
We need POC testing in schools, clinics, & travel hubs (airports, etc).
We won’t be able to safely reopen schools and many businesses without this capability.
Saliva testing could go a long way towards accomplishing this.
sciencefriday.com/segments/covid…
19/
We won’t be able to safely reopen schools and many businesses without this capability.
Saliva testing could go a long way towards accomplishing this.
sciencefriday.com/segments/covid…
19/
8.More PPE
Unbelievably, Eight months into the pandemic, PPE is still in short supply.
Beyond masks, gowns & gloves, we now face shortages of cleaning wipes and other supplies.
khn.org/news/ppe-short…
20/
Unbelievably, Eight months into the pandemic, PPE is still in short supply.
Beyond masks, gowns & gloves, we now face shortages of cleaning wipes and other supplies.
khn.org/news/ppe-short…
20/
A study in @TheLancet found that shortages of PPE were one of the biggest risk factors of health care workers (HCWs) becoming infected with COVID19.
Minority HCWs were disproportionally effected by the PPE shortages.
We need to do better.
thelancet.com/journals/lanpu…
21/
Minority HCWs were disproportionally effected by the PPE shortages.
We need to do better.
thelancet.com/journals/lanpu…
21/
In the early days of the pandemic, the federal govenment seized PPE and forced domestic suppliers to sell to them first.
Desperately, hospitals bought up all the PPE they could get, much of it imported from China and elsewhere.
This was a stopgap not a solution.
22/
Desperately, hospitals bought up all the PPE they could get, much of it imported from China and elsewhere.
This was a stopgap not a solution.
22/
We are going to need PPE for years to come. We need a reliable domestic supply.
We should nationalize production of PPE: Similar to investments in vaccine under Operation Warp Speed, the federal government should subsidize domestic PPE production.
cnbc.com/2020/08/22/cor…
23/
We should nationalize production of PPE: Similar to investments in vaccine under Operation Warp Speed, the federal government should subsidize domestic PPE production.
cnbc.com/2020/08/22/cor…
23/
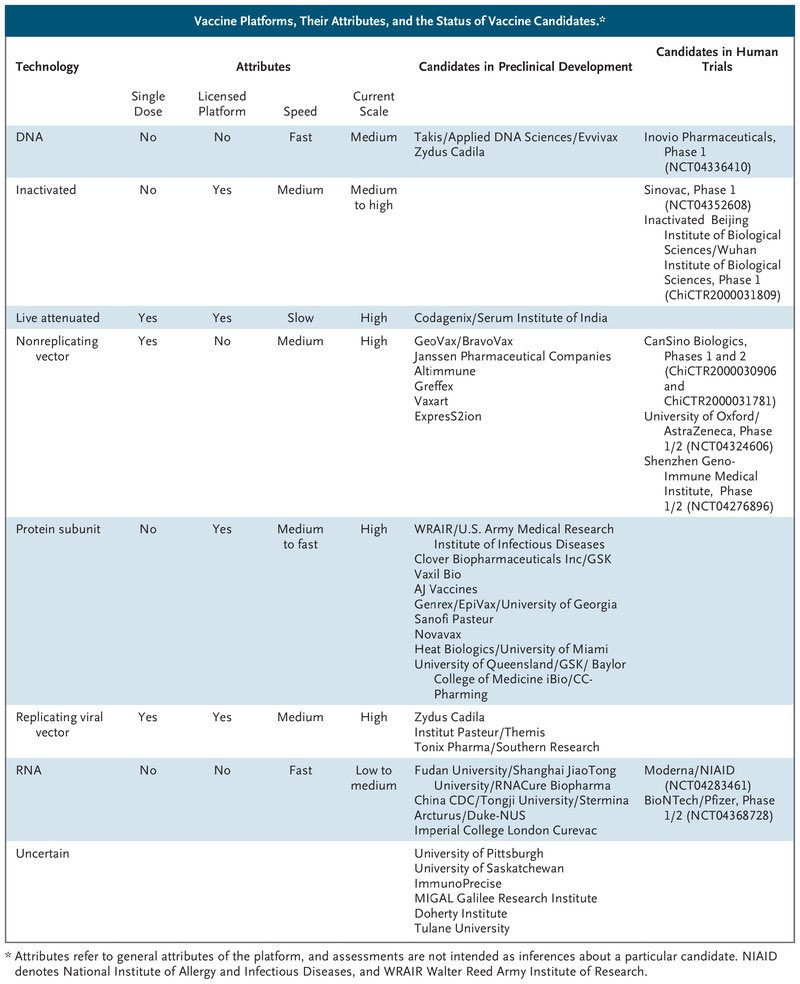
9.Don’t rush a vaccine
Long term we will need an effective vaccine to end the pandemic.
Fortunately dozens are in development including 3 promising candidates in Phase III trials.
The worst thing we could possibly do is screw it up by rushing.
24/
Long term we will need an effective vaccine to end the pandemic.
Fortunately dozens are in development including 3 promising candidates in Phase III trials.
The worst thing we could possibly do is screw it up by rushing.
24/
I’ve previously written about the perils of skipping phase III trials:
There are 3 major reasons not to rush a vaccine development program: Safety, Efficacy, and Trust
25/
https://twitter.com/nickmmark/status/1290041919465091073?s=20
There are 3 major reasons not to rush a vaccine development program: Safety, Efficacy, and Trust
25/
As we saw this week, vaccine recipients sometimes develop rare complications like transverse myelitis.
Ensuring safety takes time and large trials. It sometimes even requires pausing the trial. Pausing is a normal part of a development program.
26/
Ensuring safety takes time and large trials. It sometimes even requires pausing the trial. Pausing is a normal part of a development program.
https://twitter.com/nickmmark/status/1303459838693785601?s=20
26/
We have 3 major vaccine candidates. If any of them succeeds we will have a vaccine
If we rush we may never know which vaccine is best. We could pick the wrong one
Once a vaccine is approved its hard to conduct more trials; who would volunteer if an approved vaccine exists?
27/
If we rush we may never know which vaccine is best. We could pick the wrong one
Once a vaccine is approved its hard to conduct more trials; who would volunteer if an approved vaccine exists?
27/
It will be a herculean task to vaccinate 300+ million Americans (esp if it requires 2 shots each).
For context, the most flu vaccines we've *ever* given in 1 yr was 160 million.
We will only succeed if providers & patients trust the vaccine. Rushing compromises that trust
28/
For context, the most flu vaccines we've *ever* given in 1 yr was 160 million.
We will only succeed if providers & patients trust the vaccine. Rushing compromises that trust
28/
So how long will it take to get an approved vaccine? Most experts predict January or February 2021 (or later).
We need to be patient and not screw this up.
29/
We need to be patient and not screw this up.
https://twitter.com/katrinarmstrong/status/1304197317206192133?s=20
29/
10. Support our colleagues
Hundreds of healthcare workers have died from COVID19 infection.
Less publicized but no less tragic are our colleagues who have died from suicide.
30/
Hundreds of healthcare workers have died from COVID19 infection.
Less publicized but no less tragic are our colleagues who have died from suicide.
30/
COVID has been a marathon of physical and emotional stress.
Medical training teaches us to be tough, put our heads down, & push on. Those tactics work for acute stressors but poorly for chronic stress.
seattletimes.com/seattle-news/h…
31/
Medical training teaches us to be tough, put our heads down, & push on. Those tactics work for acute stressors but poorly for chronic stress.
seattletimes.com/seattle-news/h…
31/
In addition to the stress and worry we feel as HCWs, the pandemic has been profoundly isolating.
We should all reach out to our colleagues. And listen.
More resources from ACP on physician suicide prevention are available here:
bit.ly/2Fmqs5J
32/
We should all reach out to our colleagues. And listen.
More resources from ACP on physician suicide prevention are available here:
bit.ly/2Fmqs5J
32/
11. Vote
As healthcare workers we are bearing witness to the immense human costs of our failure to control the pandemic. As witnesses it is our duty to come forward and testify.
We need to educate our family and friends about what we’ve seen.
And we need to vote.
33/
As healthcare workers we are bearing witness to the immense human costs of our failure to control the pandemic. As witnesses it is our duty to come forward and testify.
We need to educate our family and friends about what we’ve seen.
And we need to vote.
33/
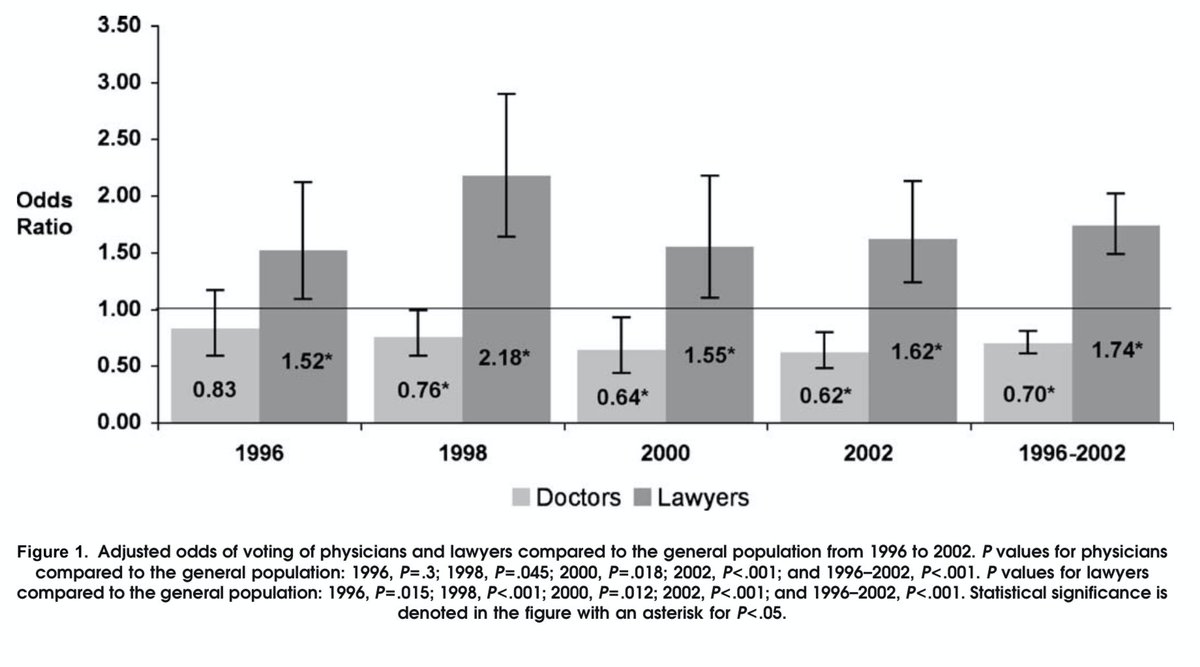
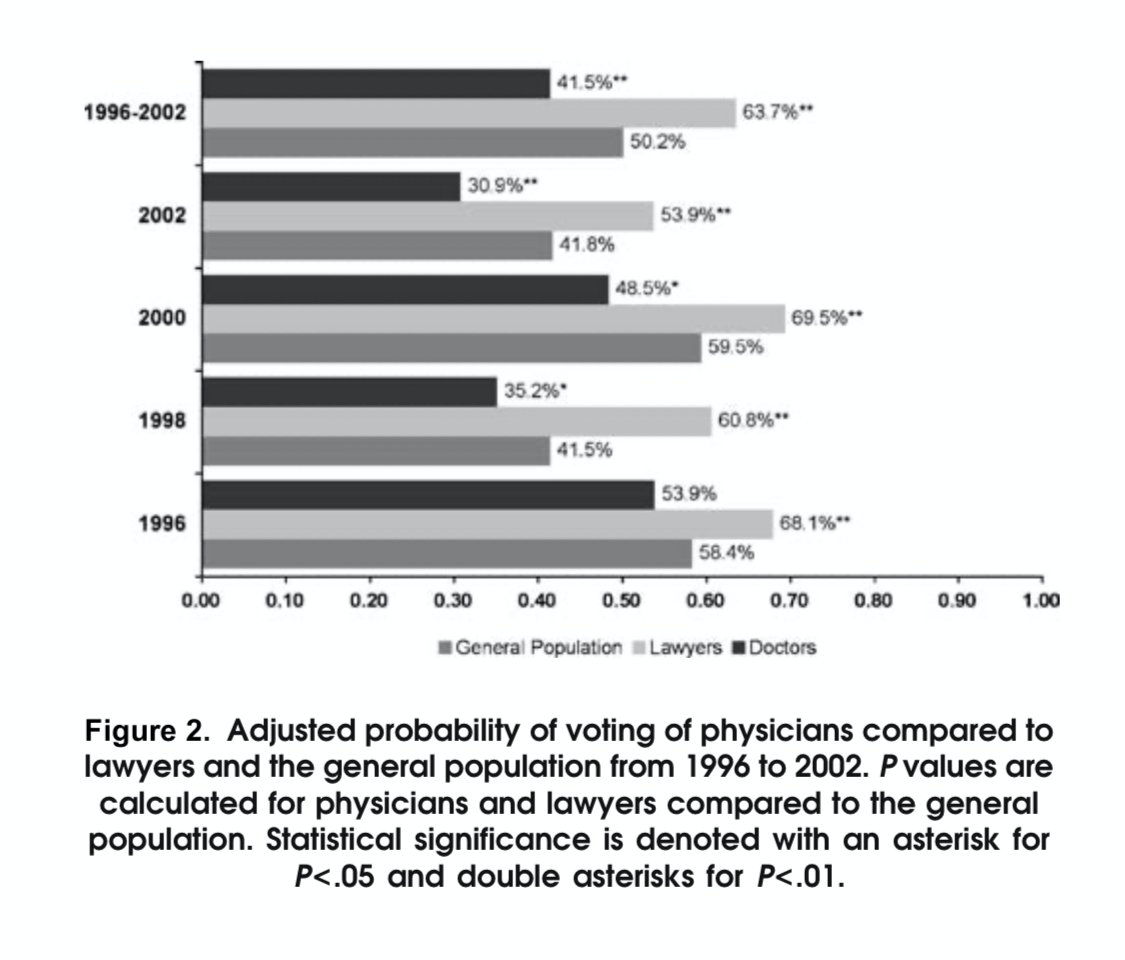
Historically, physicians vote at lower rates than the general population and much less frequently than other professionals such as lawyers.
link.springer.com/article/10.100…
34/
link.springer.com/article/10.100…
34/
That can change this year. We can do three things:
1. Register to vote: vote.org/am-i-registere…
2. Help patients & colleagues register to vote: bit.ly/33oUGNA
3. Help get out the vote: on 11/3 cancel a conference, hold someones pager, etc.
35/
1. Register to vote: vote.org/am-i-registere…
2. Help patients & colleagues register to vote: bit.ly/33oUGNA
3. Help get out the vote: on 11/3 cancel a conference, hold someones pager, etc.
35/
We can’t save the 200,000 people already killed & the millions more irreparably harmed by COVID19.
Every week thousands more are dying.
Most of these deaths are preventable.
We need leaders implementing national evidence based policies to make it stop.
36/36
Every week thousands more are dying.
Most of these deaths are preventable.
We need leaders implementing national evidence based policies to make it stop.
36/36
• • •
Missing some Tweet in this thread? You can try to
force a refresh