Lots of articles about ICUs reaching capacity, but what does this actually mean?
Buckle up for a #tweetorial about ICU capacity and what it means in the context of #COVID19.
1/
Buckle up for a #tweetorial about ICU capacity and what it means in the context of #COVID19.
1/




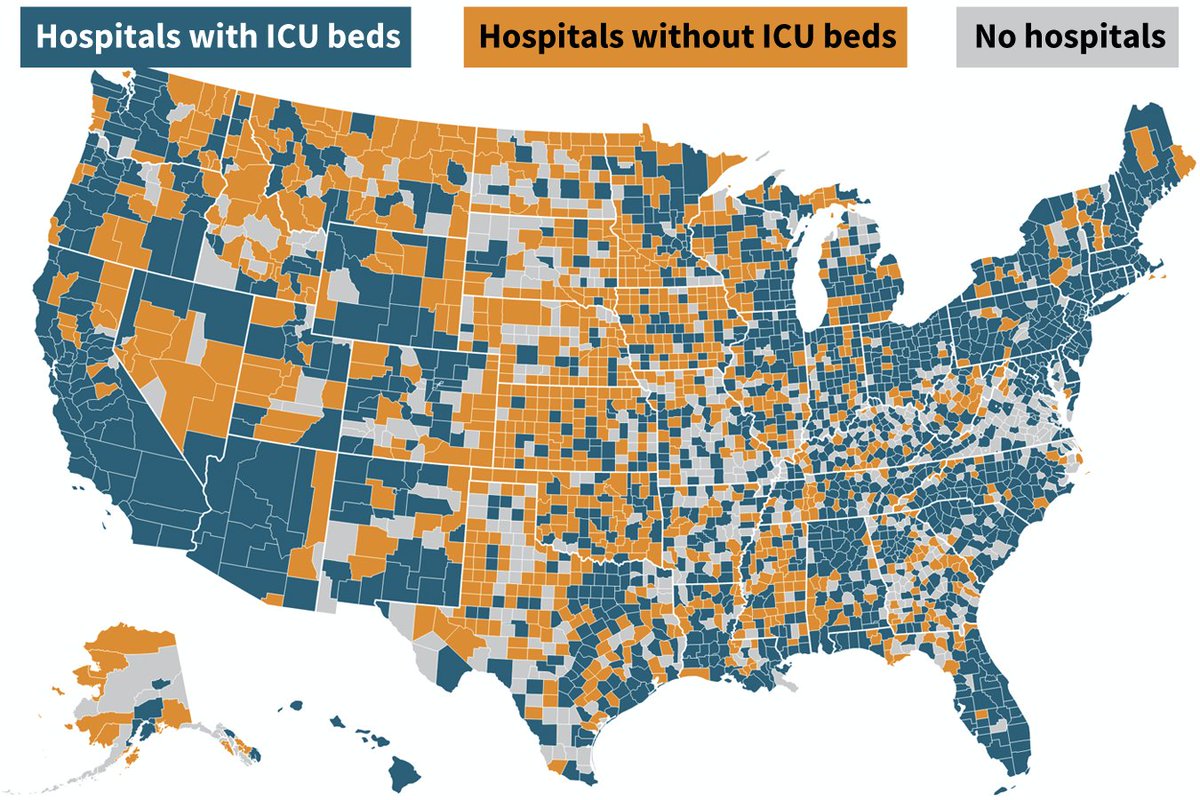
First, statewide measures of ICU capacity can be misleading. Critically ill patients generally go to the nearest hospital. Having "10% of ICU beds free statewide" isn’t reassuring if most ICUs are completely full and a few ICUs hundreds of miles away are mostly empty.
2/
2/
Instead of statewide numbers, let's focus on ICU capacity within individual hospitals. Unlike airlines that want to fly full, ICUs are not intended to be full, particularly for prolonged periods.
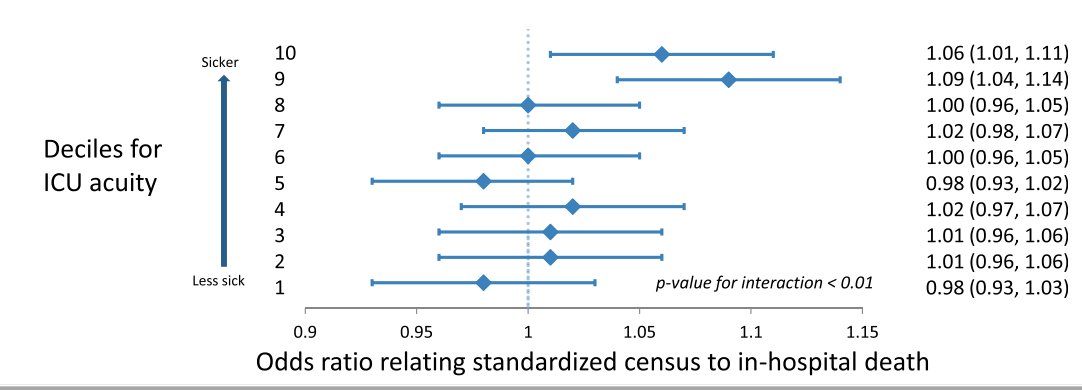
There is evidence that higher ICU census is associated with worse outcomes:
3/
There is evidence that higher ICU census is associated with worse outcomes:
3/
For example, a large observational study of 264k patients in 155 ICUs across the US found that higher census was associated with increased mortality, particularly when the average acuity was higher.
➡️atsjournals.org/doi/pdf/10.116…
4/
➡️atsjournals.org/doi/pdf/10.116…
4/
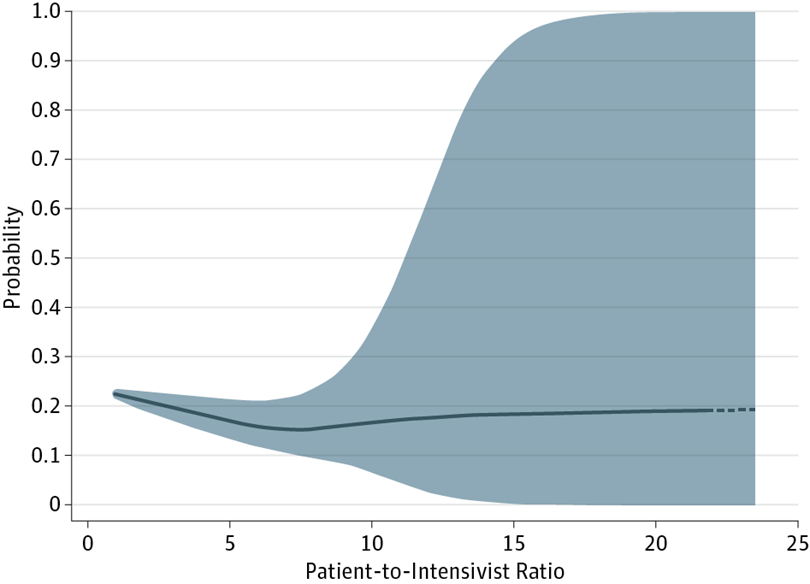
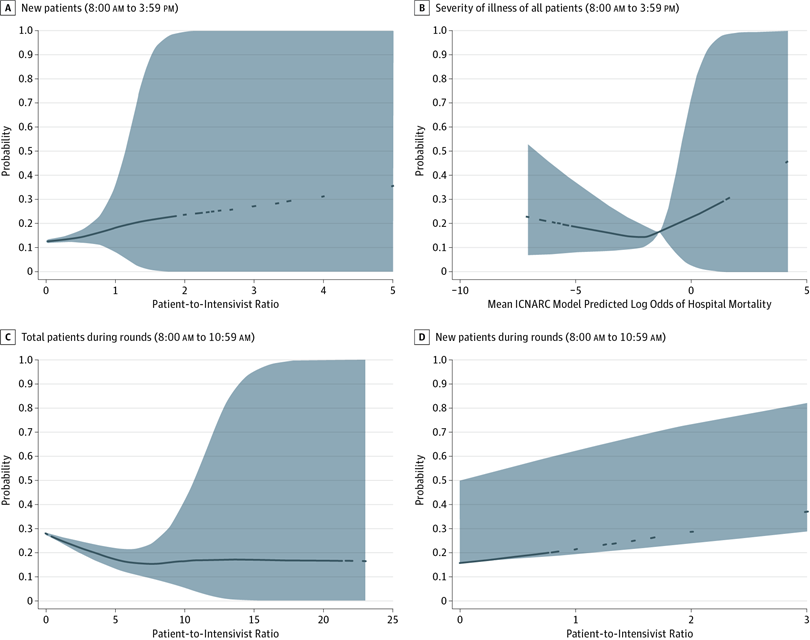
Another study looking at 64k patients in 94 ICUs in the UK, found that hospital mortality increased if the Patient to Intensivist Ratio (PIR) rose above 7.5.
➡️jamanetwork.com/journals/jamai…
5/
➡️jamanetwork.com/journals/jamai…
5/
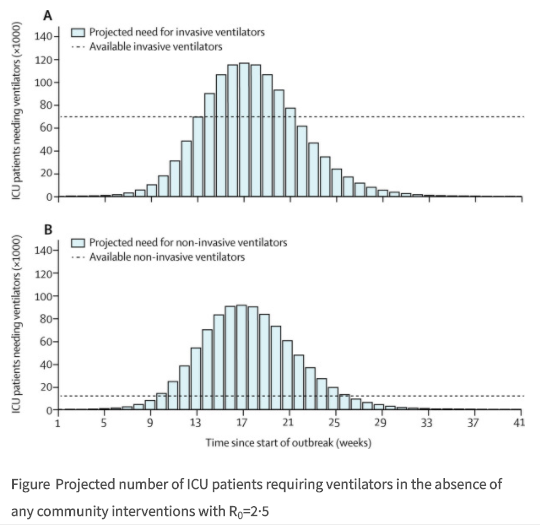
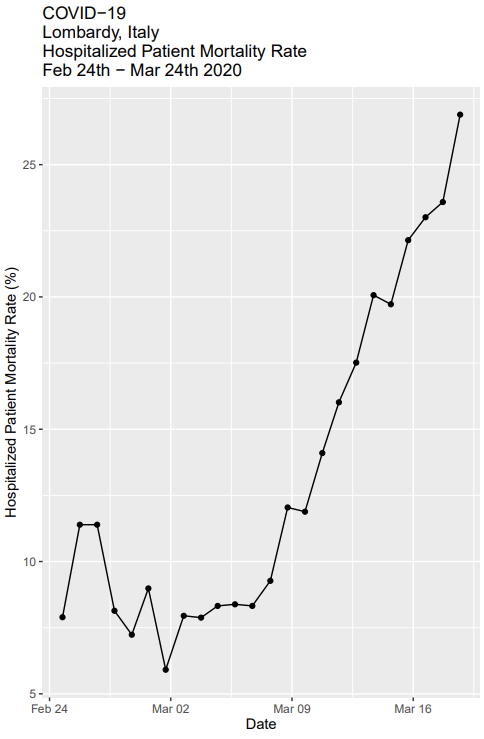
One of the factors that led to high mortality for people with #COVID19 COVID in Italy, Spain, & NYC was ICUs reaching capacity.
When there aren’t enough beds, some people who need ICU interventions (ventilators, vasopressors, dialysis) don’t get them, as in Italy:
6/
When there aren’t enough beds, some people who need ICU interventions (ventilators, vasopressors, dialysis) don’t get them, as in Italy:
6/
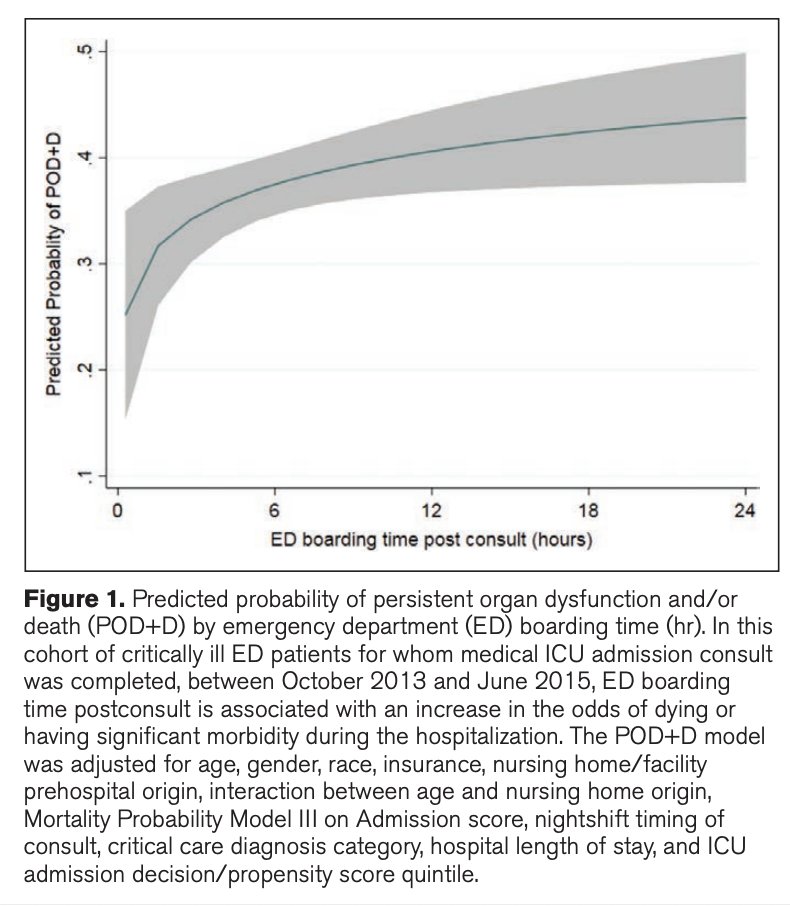
Where do patients go when ICUs are full? They can stay in the ED, but EDs don’t have the staffing ratios to optimally care for critically ill pts for long.
A 2018 study in NYC found that ED boarding of critically ill patients was associated with increased risk of death.
7/
A 2018 study in NYC found that ED boarding of critically ill patients was associated with increased risk of death.
7/
People critically ill with #COVID19 require a lot of attention: managing ventilators, analgesia, hemodynamics takes time. When ICUs get full details get missed.
From the perspective of ICU strain, acuity, & Patient:Intensivist ratio (PIR), COVID-19 is the perfect storm.
8/
From the perspective of ICU strain, acuity, & Patient:Intensivist ratio (PIR), COVID-19 is the perfect storm.
8/
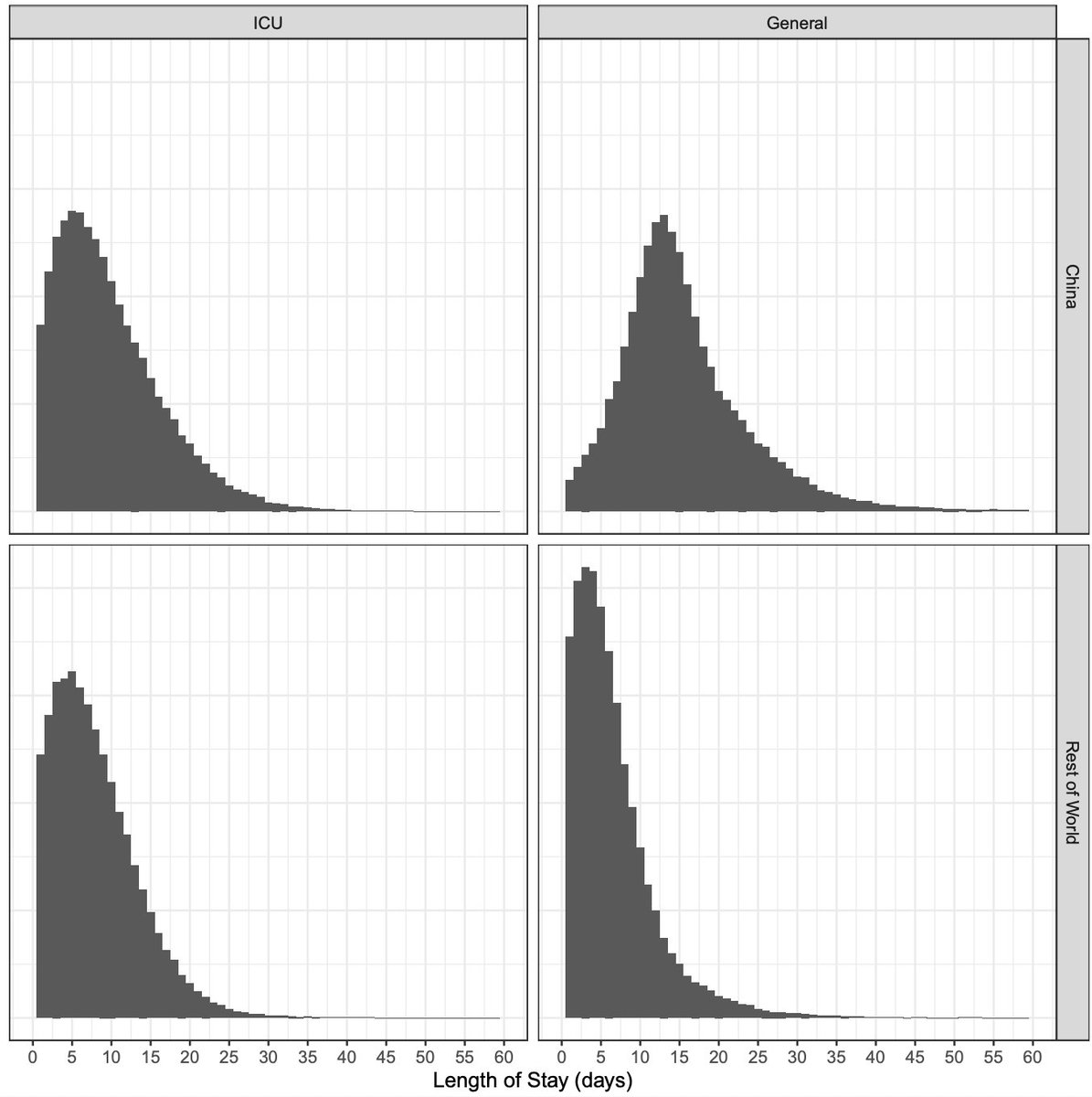
Another challenge is length of stay (LOS). Normally, ICU LOS is ~3 days. Many ICU patients are sick on admission but recovery quickly. (Think about CHF w/ diuresis, COPD w/ steroids and antibiotics, etc).
This is not the case with COVID19.
9/
This is not the case with COVID19.
9/
Patients with COVID19 in the ICU tend to require mechanical ventilation for much longer in order to recover. A pre-print found that among people with COVID admitted to the ICU the median LOS was 4-19 days.
➡️medrxiv.org/content/10.110…
10/
➡️medrxiv.org/content/10.110…
10/
This means that an ICU filled with COVID19 patients will stay full for much longer.
Even if the influx of critically ill patients ceased today, ICUs would remain full for weeks. Given the 2-4 week lag b/w public health interventions and a decline in cases, this is bad news.
11/
Even if the influx of critically ill patients ceased today, ICUs would remain full for weeks. Given the 2-4 week lag b/w public health interventions and a decline in cases, this is bad news.
11/

It’s also worth discussing the dubious math used to calculate ICU beds & capacity. The denominator (# of ICU beds) includes all ICU beds: medical, surgical, cardiac, neuroscience, burn, trauma, & in some cases even pediatric ICUs. Some hospitals even count PACUs as ICU beds.
12/
12/

While all ICUs can provide standard ICU interventions
- Not all have negative pressure rooms.
- Not all have connections to run dialysis machines.
- Not all are accustomed to caring for patients with severe ARDS from COVID & only some are familiar with ECMO, proning, etc.
13/
- Not all have negative pressure rooms.
- Not all have connections to run dialysis machines.
- Not all are accustomed to caring for patients with severe ARDS from COVID & only some are familiar with ECMO, proning, etc.
13/
Finally, the most important factor to consider: People
Critical care is less about specialized machines & more about highly trained professionals who can care for sick patients. You can ‘uplevel’ a step-down unit but you can’t easily create more CCRNs, RTs, pharmacists, etc.
14/
Critical care is less about specialized machines & more about highly trained professionals who can care for sick patients. You can ‘uplevel’ a step-down unit but you can’t easily create more CCRNs, RTs, pharmacists, etc.
14/
At many hospitals, staff is already limiting.
Prior to COVID there was a national shortage of ICU RNs: of the 3.3m RNs in the US, just 290k (~15%) are critical care RNs. This includes adult, peds, & neonatal.
COVID has exacerbated the shortage.
➡️healthaffairs.org/do/10.1377/hbl…
15/
Prior to COVID there was a national shortage of ICU RNs: of the 3.3m RNs in the US, just 290k (~15%) are critical care RNs. This includes adult, peds, & neonatal.
COVID has exacerbated the shortage.
➡️healthaffairs.org/do/10.1377/hbl…
15/
ICU occupancy varies by hospital, but nationally occupancy is ~60-65%.
ICU staffing flexes to match these changes. Short term holes can be filled with overtime, but this model can't work for months on end.
If ICUs are full for weeks, we will have major staffing shortages.
16/
ICU staffing flexes to match these changes. Short term holes can be filled with overtime, but this model can't work for months on end.
If ICUs are full for weeks, we will have major staffing shortages.
16/
Also, critical care providers are at risk for contracting #COVID19.
Despite widespread underreporting, as of May >60,000 US HCPs had been infected.
In NYC, serological testing revealed that 12% of HCWs had antibodies against SARS-CoV-2.
17/
npr.org/sections/healt…
Despite widespread underreporting, as of May >60,000 US HCPs had been infected.
In NYC, serological testing revealed that 12% of HCWs had antibodies against SARS-CoV-2.
17/
npr.org/sections/healt…
Part of the reason so many HCP got sick was a lack of PPE, which was a major issue early in the pandemic.
Despite 6 more months to prepare, there are worrisome signs that this new surge could once again make PPE scarce.
18/
washingtonpost.com/health/2020/07…
Despite 6 more months to prepare, there are worrisome signs that this new surge could once again make PPE scarce.
18/
washingtonpost.com/health/2020/07…
Another issue is burnout. Caring for many critically ill patients is physically & emotionally exhausting.
A recent review noted “The backbreaking workload shouldered by RNs…contributes to burnout by depleting the capacity of the people available to meet the needs of the job”
19
A recent review noted “The backbreaking workload shouldered by RNs…contributes to burnout by depleting the capacity of the people available to meet the needs of the job”
19

As the pandemic goes on, healthcare providers will get sick and burnt out, staffing will likely get even more limited. ICU capacity will be further strained.
I’ve been worried about this since the early days of the pandemic:
20/
I’ve been worried about this since the early days of the pandemic:
20/
So what can we do about this?
* limit further spread of the coronavirus #stayhome #WashYourHands #WearAMask
* bring trained staff, such as civilian volunteers or military medical teams, to the hardest hit hospitals,
* keep staff safe & healthy #GetUsPPE
* limit further spread of the coronavirus #stayhome #WashYourHands #WearAMask
* bring trained staff, such as civilian volunteers or military medical teams, to the hardest hit hospitals,
* keep staff safe & healthy #GetUsPPE