Did monoclonal antibodies save the President's life?
We'll never know, but it's possible and the implications are profound.
Let me explain 1/
We'll never know, but it's possible and the implications are profound.
Let me explain 1/
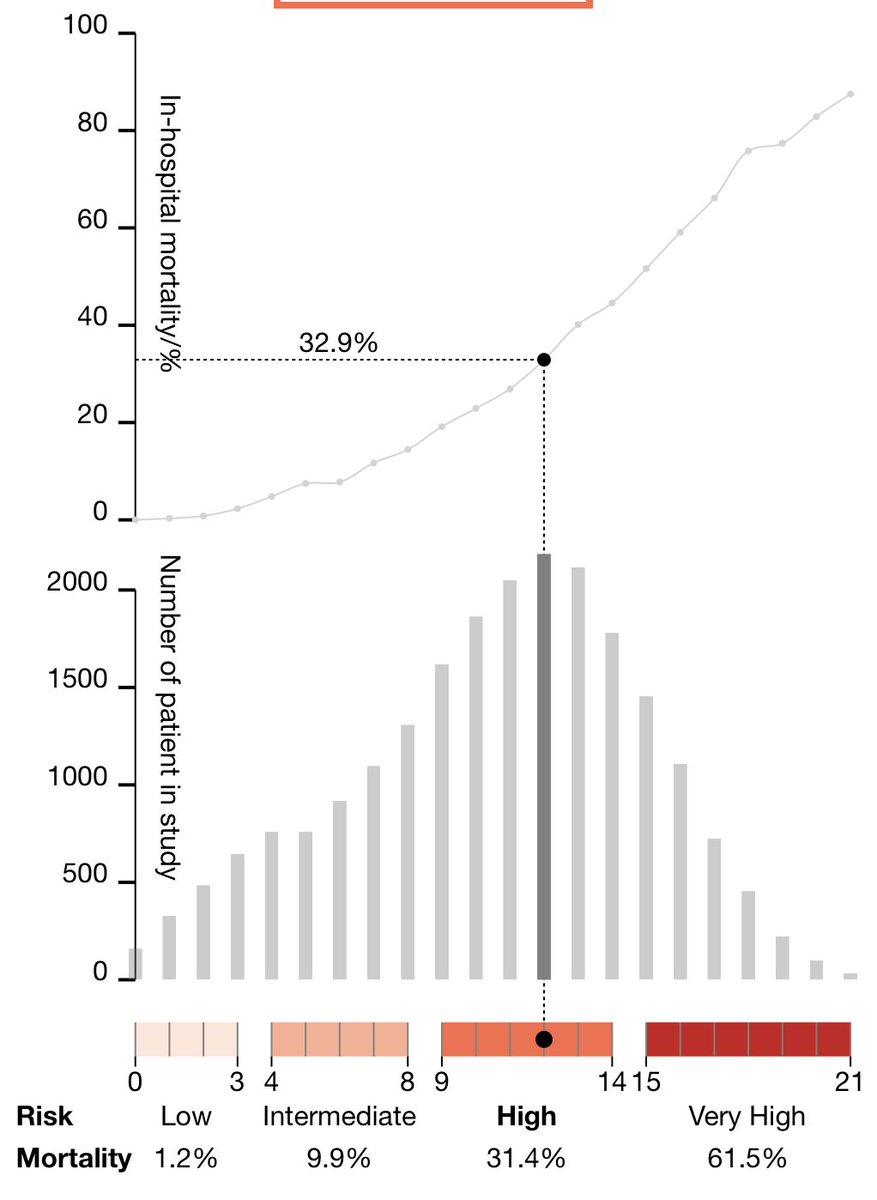
Trump's risk profile by demographics was high (age, male, obesity) but it markedly increased when he had blood oxygen desaturation, had an abnormal lung CT scan of pneumonia, and was hospitalized
Mortality risk > 32% isaric4c.net/risk/ 2/
Mortality risk > 32% isaric4c.net/risk/ 2/
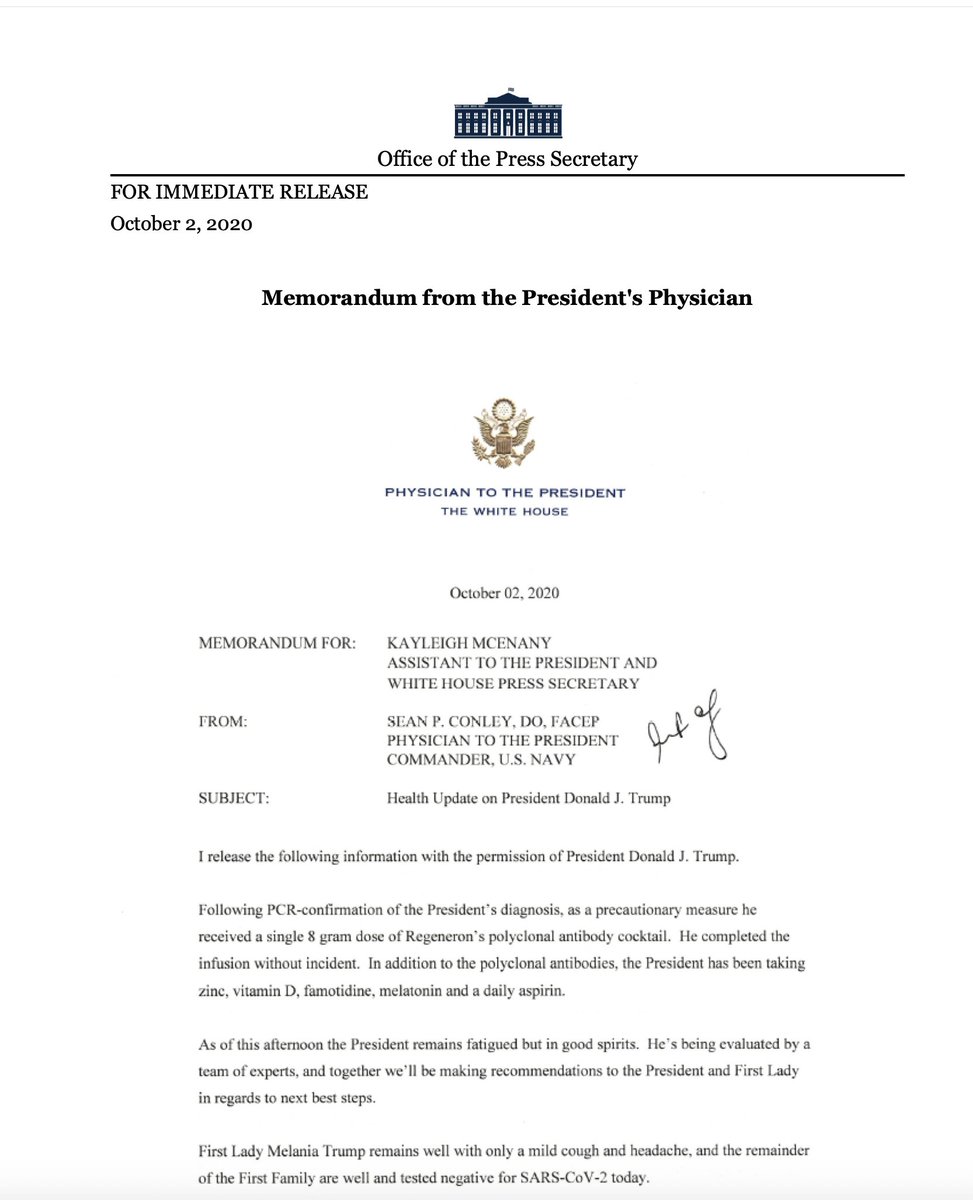
Sometime on Friday (<-presumably) he received a monoclonal antibody cocktail (2 different antibodies to override the potential of a virus escape variant)
Diagram from @VirusesImmunity 3/
Diagram from @VirusesImmunity 3/
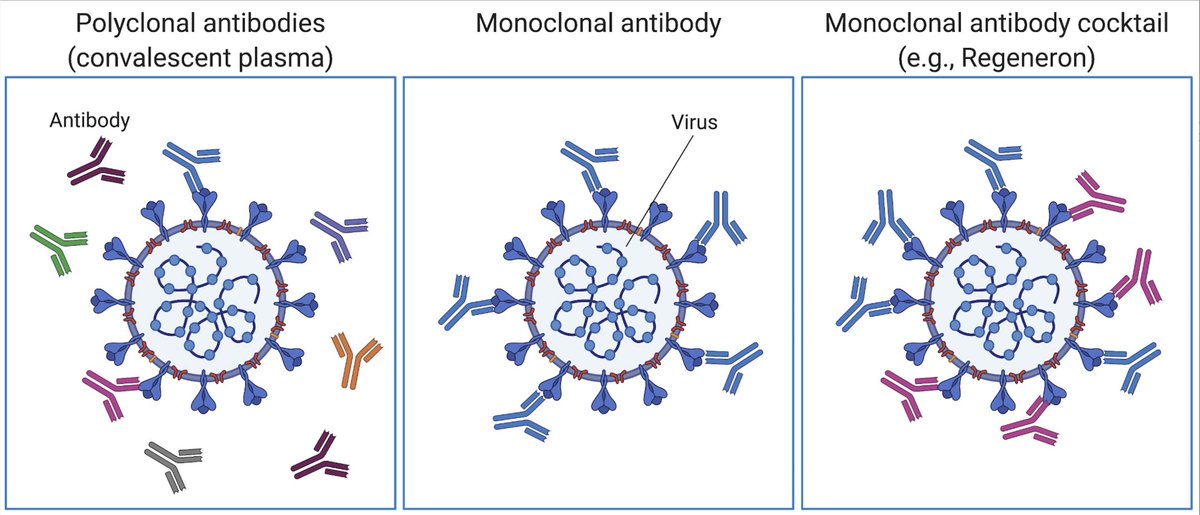
Convalescent plasma has many antibodies that are not neutralizing, do not atttack/inactivate the virus. And plasma has many other constituents. Monoclonals Abs are pure, potent neutralizing antibodies. Reviewed here
https://twitter.com/EricTopol/status/12903562009539379214/
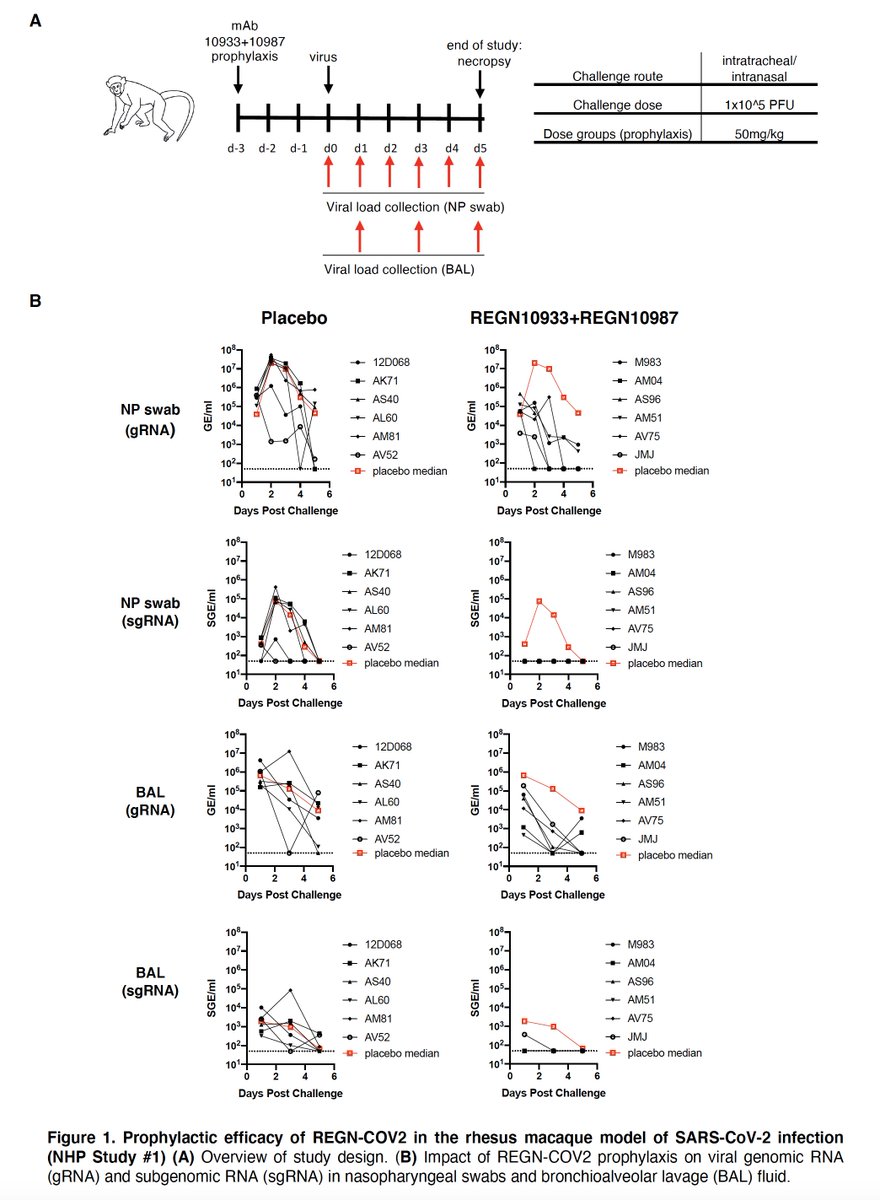
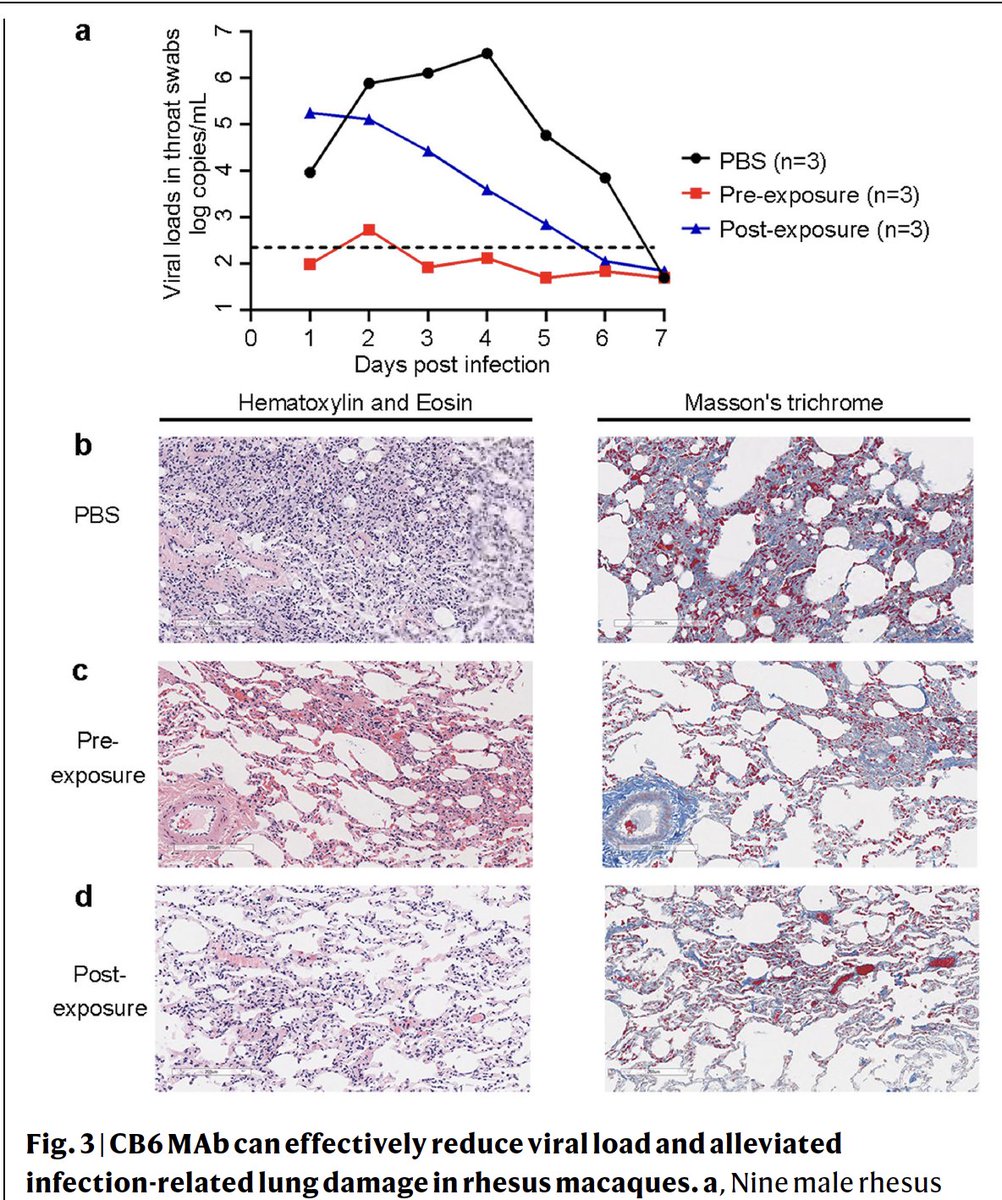
When monoclonal Abs were given to non-human primates who were then #SARSCoV2 infected, illness was prevented. 5/
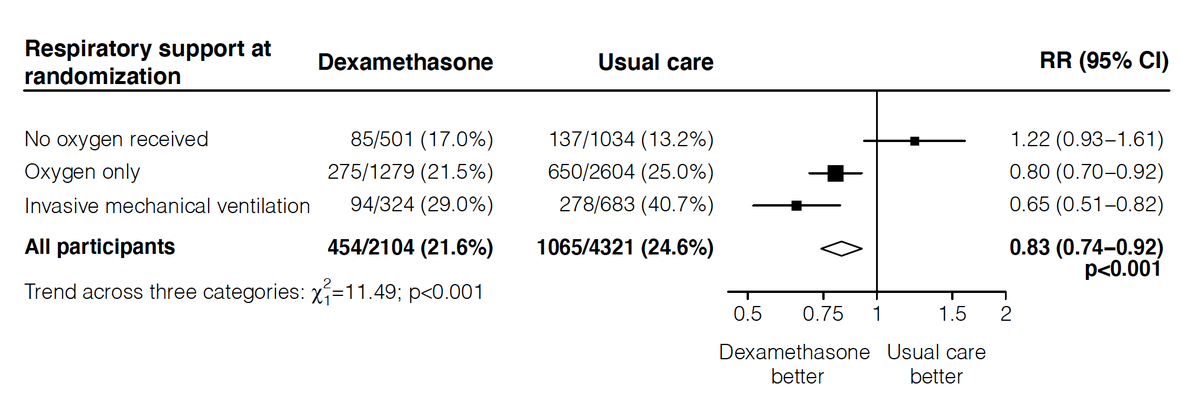
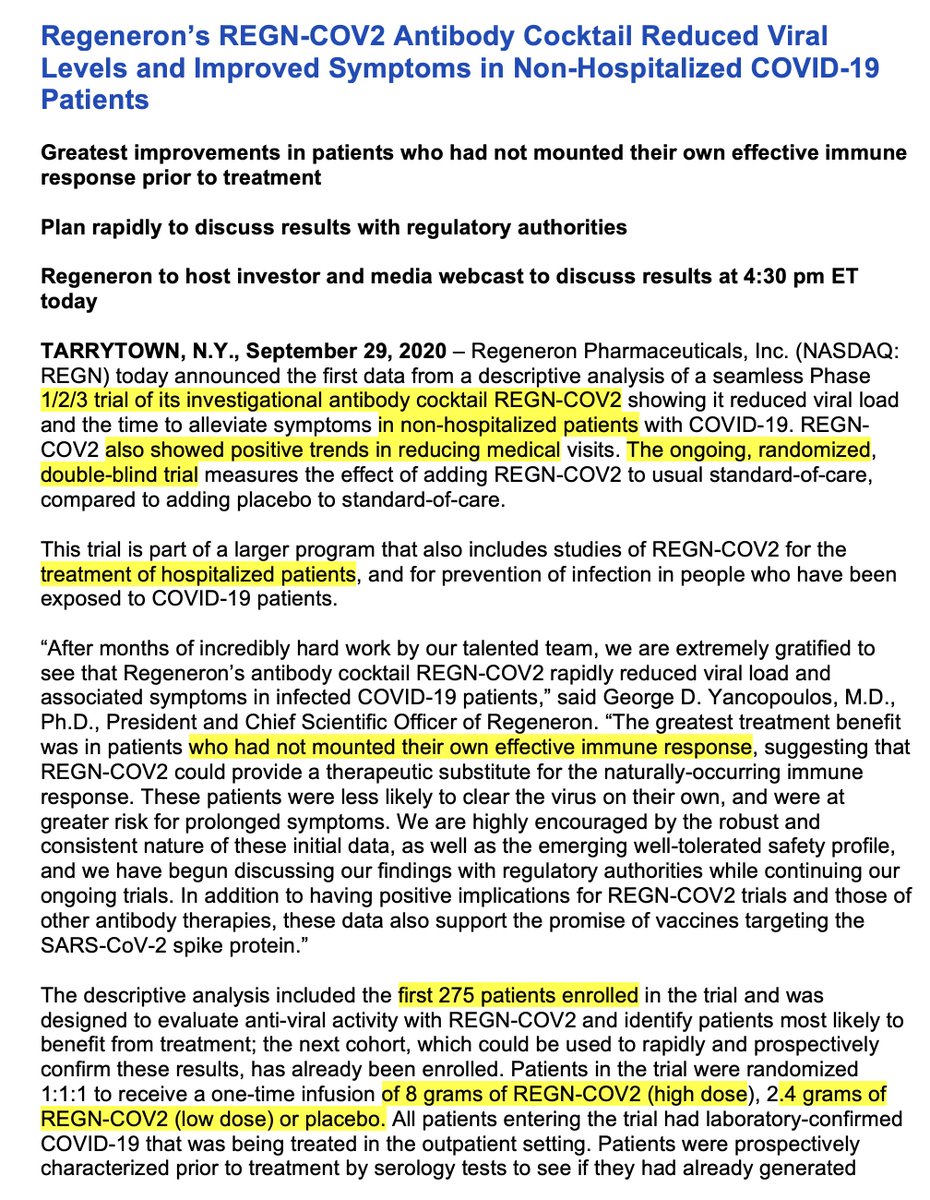
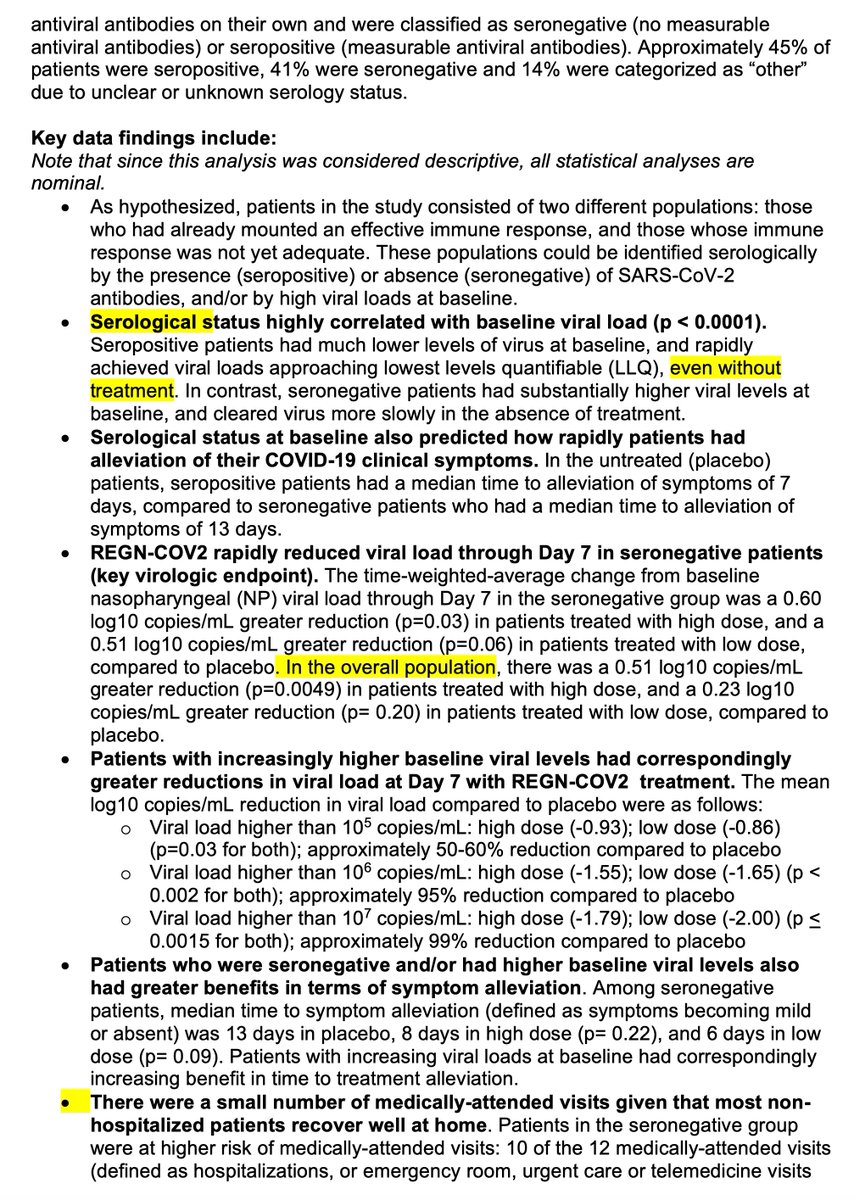
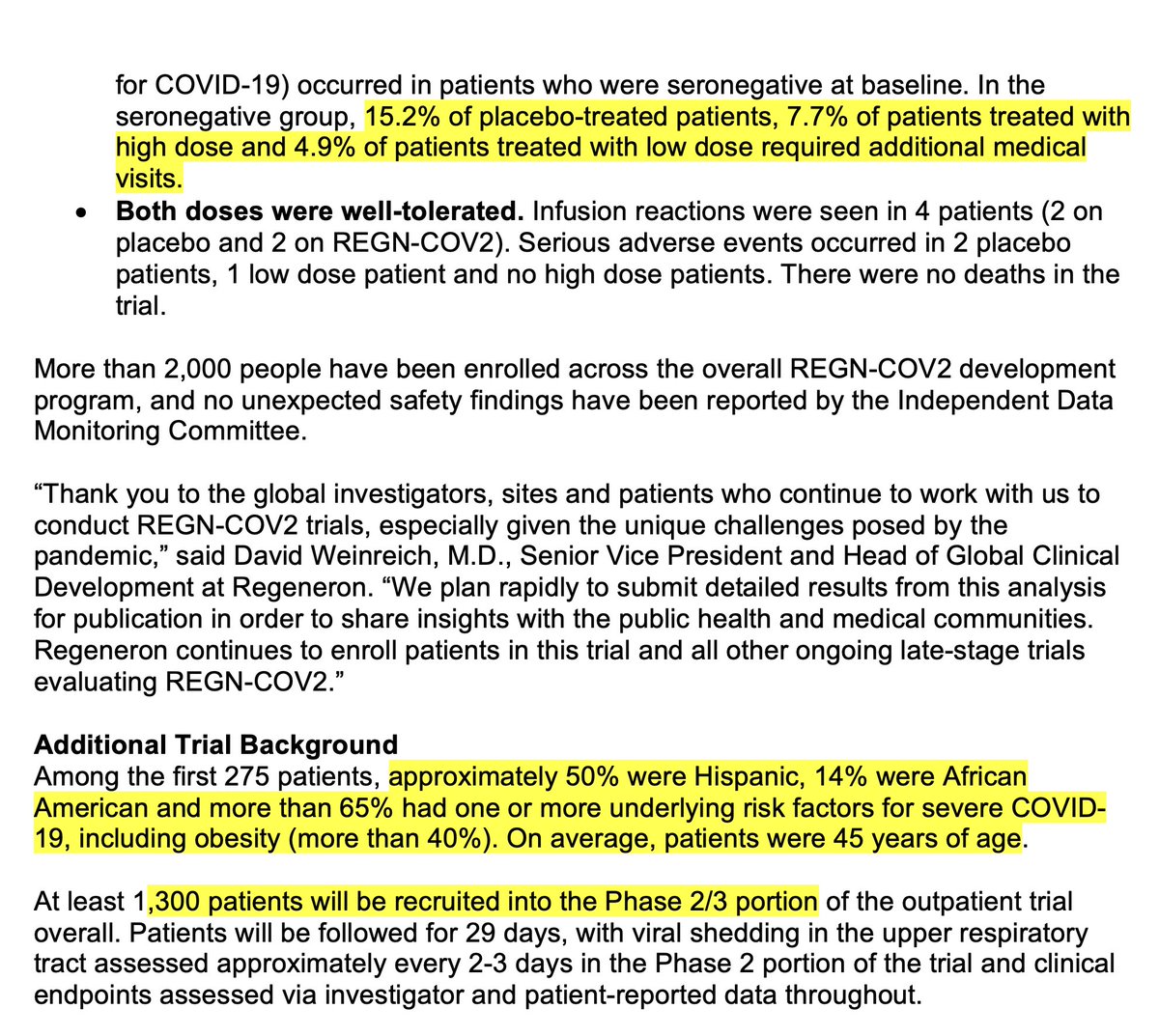
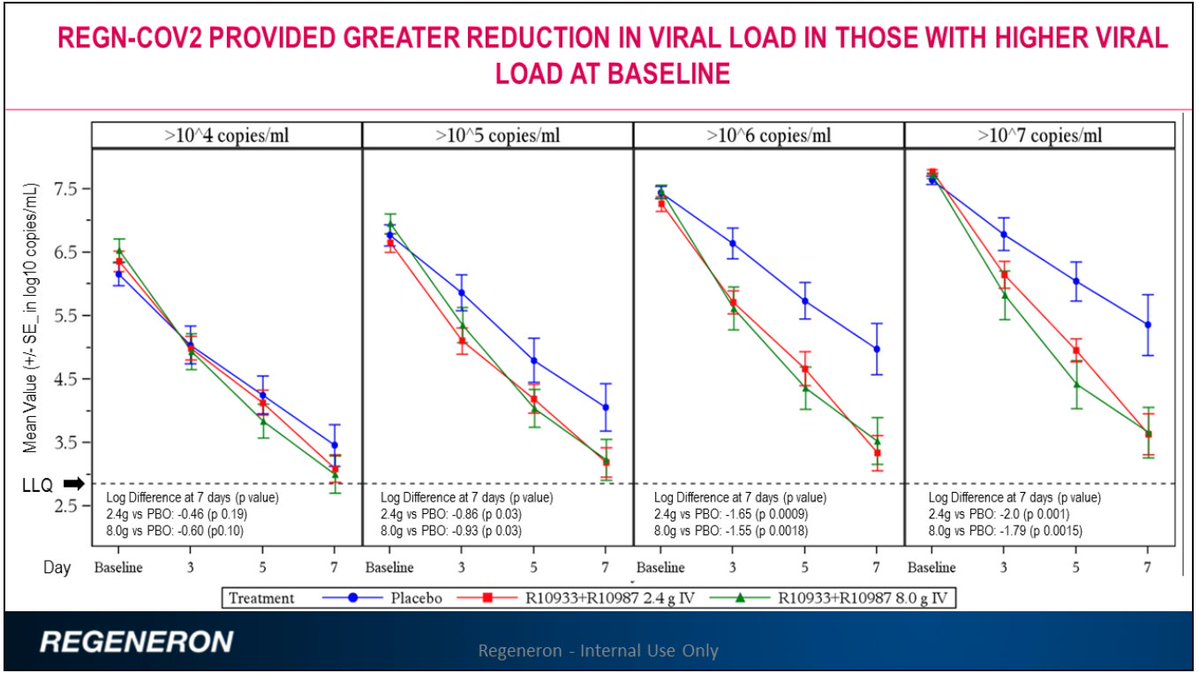
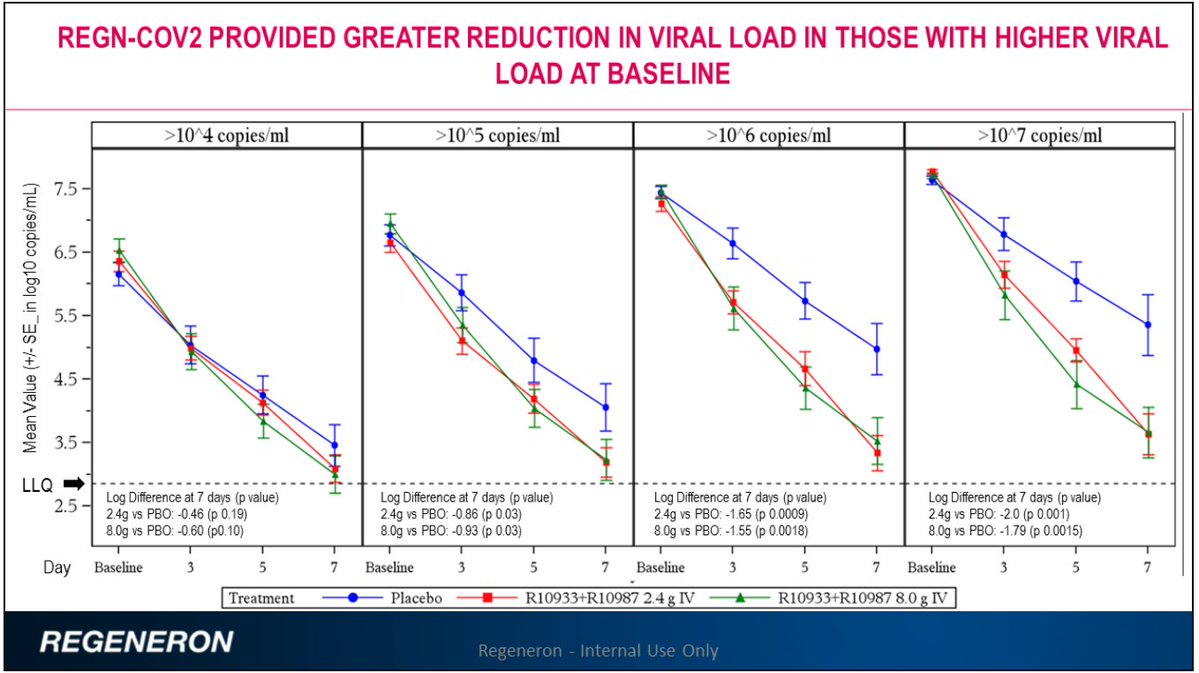
In two Phase 2 covid outpatient clinical trials of different monoclonal antibody preparations there was good evidence of viral load reduction and potential support for clinical benefit. Regeneron data summed up previously; ? high dose used here
https://twitter.com/EricTopol/status/13121600018514165776/
Lilly/AbCellera data here. Hospitalization reduction trend, dose response issue
investor.lilly.com/news-releases/…
blogs.sciencemag.org/pipeline/archi… 7/
investor.lilly.com/news-releases/…
blogs.sciencemag.org/pipeline/archi… 7/
Back to the patient. It's fuzzy. But,he had a pretty dramatic turnaround from Friday to Saturday. He received 2 drug treatments, the antibody prep and Remdesivir. The effect of the latter is modest and its indication soft, only proven in a randomized trial for severe covid 8/
If indeed his course substantially changed, as further suggested Sunday that he's potentially ready for hospital discharge Monday, it might be attributable to the antibody. It's the only Rx he received that could account for this. But it might also have occurred spontaneously 9/
We may find out about real life-saving potential of the monoclonals from ongoing large randomized Phase 3 trials. For now, from the body of data we have, let's make an assumption they have strong clinical benefit. What's the effect at many levels? 10/
For Trump, he may now think covid-19 is no big deal since he was only sick for a couple of days and because he's so "strong" he conquered the disease. Unlike anyone who can, he refused to wear a mask @fmanjoo @nytopinion
nytimes.com/2020/09/30/opi… 11/
nytimes.com/2020/09/30/opi… 11/
But, ironically, now he is only 1 of 10 people who received a monoclonal antibody cocktail for "compassionate use"
washingtonpost.com/health/an-army… @lauriemcginley2 12/
washingtonpost.com/health/an-army… @lauriemcginley2 12/
The monoclonal antibody preparations are hard to scale and will undoubtedly be very expensive. Even with all the different manufacturers and assuming all get formal FDA approval, the number of available dose will be very limited washingtonpost.com/health/2020/09… @Carolynyjohnson
13/
13/
This will inevitably worsen the profound inequities in the US since we know the highest risk patients are the underrepresented minorities, the least likely to get access to #healthcare, testing, care and this advanced, costly therapy 14/
So the case of Trump and monoclonals may portend both the best and worst. Best that the drugs could be used to stop the progression of covid illness and save lives. Worst is that they will only be accessible for few, and likely the people who don't need them the most. 15/
There's an alternative strategy to monoclonal antibodies that would be cheaper, more scalable, and could potentially be given by inhalation. Nanobodies. Seems like this path should be actively pursued. 16/
nature.com/articles/s4146…
nature.com/articles/s4146…

Nanobodies
Fixed link nature.com/articles/s4146…
@AashishManglik @UCSF @HHMINews work (preprint) biorxiv.org/content/10.110…
Summary by @Dereklowe blogs.sciencemag.org/pipeline/archi…
Fixed link nature.com/articles/s4146…
@AashishManglik @UCSF @HHMINews work (preprint) biorxiv.org/content/10.110…
Summary by @Dereklowe blogs.sciencemag.org/pipeline/archi…
• • •
Missing some Tweet in this thread? You can try to
force a refresh