
As @JPSoucy points out in this excellent 🧵, we have a experienced a considerable drop in testing. The question we don't know is: how many should we be testing? @skepticalIDdoc and other super-smart people suggest keeping our eye on %+. I am going to try to reframe the problem.
https://twitter.com/JPSoucy/status/1319047155915673602
I will start off by saying this:
"cases" are numerator
"tests performed" are denominator
"% positivity" are cases/tests performed
If you do 20 surveillance tests (i.e. in asymptomatics) in a school, or 200, the % positivity will remain the same, but the "cases" will increase.
"cases" are numerator
"tests performed" are denominator
"% positivity" are cases/tests performed
If you do 20 surveillance tests (i.e. in asymptomatics) in a school, or 200, the % positivity will remain the same, but the "cases" will increase.

Cases matter.
They theoretically matter to the case (so they can receive treatment if they need it).
They should matter to public health to identify contacts (who may be infected) #ContactTracing
They should matter to everyone if we are treating them as surveillance.
They theoretically matter to the case (so they can receive treatment if they need it).
They should matter to public health to identify contacts (who may be infected) #ContactTracing
They should matter to everyone if we are treating them as surveillance.
When we were testing everyone and their brother and sister, dog and cat, cases kinda reflected surveillance: CASES MATTERED.
But it overwhelmed the system. So the government (who failed to plan for surveillance) employed #behaviouraleconomics to change testing and reduce backlog
But it overwhelmed the system. So the government (who failed to plan for surveillance) employed #behaviouraleconomics to change testing and reduce backlog

In BE, you either make things easier to do (sometimes referred to as "nudges") or more difficult to do (sometimes referred to as "sludge"). We already had some sludge built in (long lineups for testing; few testing locations; slow TAT).
This is a great read for those interested.
This is a great read for those interested.
Such sludge will automatically reduce low-risk people from being tested (who asymp. will line up for 5 hours for a test?) and will, without any change in epi, increase test positivity. But govt. added sludge:
- change criteria for testing (this was a good sludge)
- appointments
- change criteria for testing (this was a good sludge)
- appointments
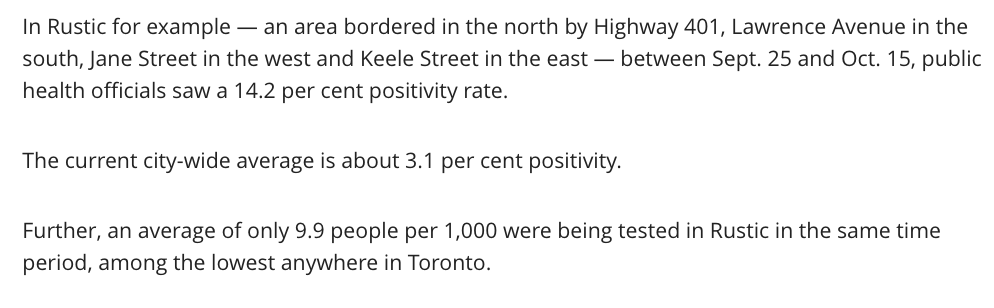
The important thing about sludge is it is designed to be "equal" but it is not equitable. So reducing testing in, say, rural areas by 50% is probably a good thing. But reducing it in NW Toronto is not. At all.
So now we need nudges in places with high epi (e.g mobile testing)
So now we need nudges in places with high epi (e.g mobile testing)
But it won't fix our dichotomous prob: as we target testing to high risk, it still won't be surveillance and test positivity will likely be non-generizable outside of those communities.
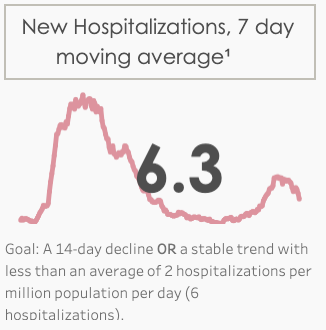
Bottom line: we're flying without a fuel gauge & navigation system. Only reliable signpost:
Bottom line: we're flying without a fuel gauge & navigation system. Only reliable signpost:
So now we need to:
a) Figure out how to do some kind of surveillance (wastewater? 613covid.ca/wastewater/)
b) Reduce sludge to identify as many cases as possible
c) Get contact tracing back on track and up to speed
d) physically distance, mask, avoid indoors & crowds, wash hands
a) Figure out how to do some kind of surveillance (wastewater? 613covid.ca/wastewater/)
b) Reduce sludge to identify as many cases as possible
c) Get contact tracing back on track and up to speed
d) physically distance, mask, avoid indoors & crowds, wash hands
• • •
Missing some Tweet in this thread? You can try to
force a refresh



