Neuroanatomy TOTD #10🧵
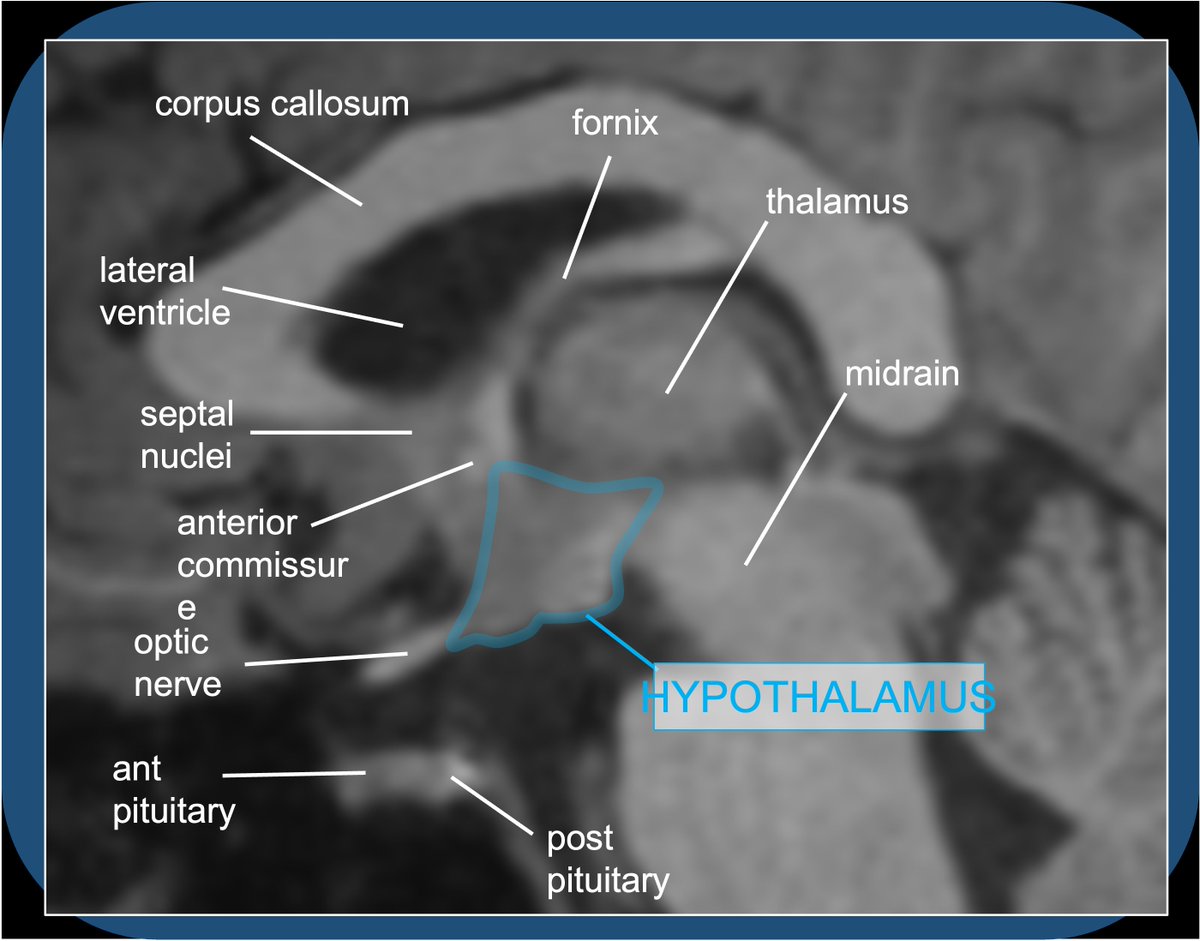
1/5 Small gray matter structure at the junction of the thalamus and midbrain is the subthalamic nucleus (STN).
#meded #FOAMed #FOAMrad #medtwitter #medstudents #radiology #neurorad #radres #neurology #neurosurgery #neuroanatomy #neuroanatomyTOTD
1/5 Small gray matter structure at the junction of the thalamus and midbrain is the subthalamic nucleus (STN).
#meded #FOAMed #FOAMrad #medtwitter #medstudents #radiology #neurorad #radres #neurology #neurosurgery #neuroanatomy #neuroanatomyTOTD

2/5...The STN is functionally a node within the basal ganglia (BG) INDIRECT LOOP. STN contains excitatory glutaminergic neurons➞output to the GABA neurons of GPi, which in turn have inhibitory effect on thalamic outputs to the motor cortex.

3/5...Loss of nigrostriatal input in Parkinsons Dz➞increased inhibitory output from GPi➞decreased thalamic stimulation of the motor cortex (through both direct and indirect loop circuits). Makes sense that DBS treatments were initially directed at disrupting activity in GPi.

4/5...DBS treatments for PD are now more commonly directed at the STN, with similar results➞decreased excitatory output to the GPi, and thus decreased inhibitory output to thalamus➞increased movement.

5/5...DBS tx for PD now more commonly directed at disruption of STN w/ similar results➞decreased excitatory output to GPi➞decreased inhibitory output to thalamus➞increased movement. DBS to the STN can also treat essential termor. Lesion/stroke involving STN➞ hemiballismus.

• • •
Missing some Tweet in this thread? You can try to
force a refresh