
Neuroradiologist, @kpwashington, @UWRadiology, UW SOM #neuroanatomy instructor; photography, guitar, baseball, dad of 3 #neurorad
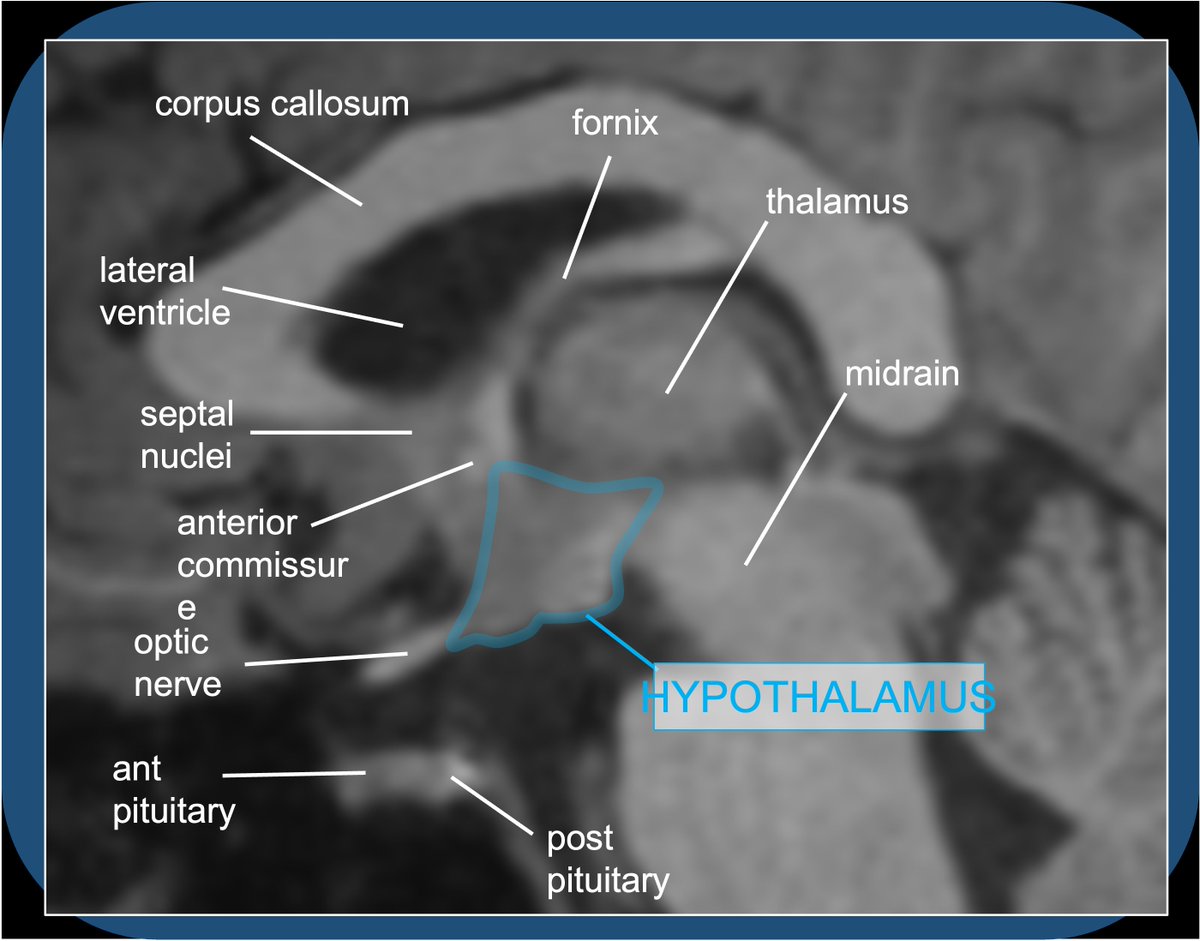 Quiz A: Histamine activity in the brain/brainstem contributes to alertness/wakefulness–hence: sleepy effects of benadryl. Histaminergic neurosecretory cell bodies are exclusively in the tuberomammillary nucleus of the TUBER CINEREUM (HT floor), with widespread projections.
Quiz A: Histamine activity in the brain/brainstem contributes to alertness/wakefulness–hence: sleepy effects of benadryl. Histaminergic neurosecretory cell bodies are exclusively in the tuberomammillary nucleus of the TUBER CINEREUM (HT floor), with widespread projections. 
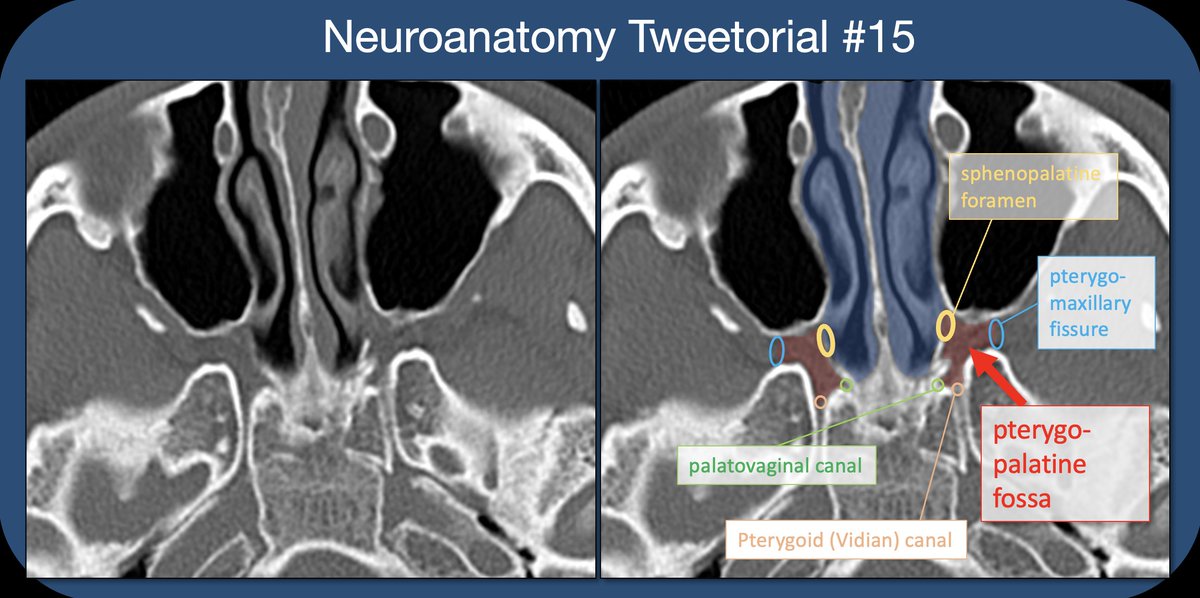 The PTERYGOPALATINE FOSSA (PPF) is a space deep in the face/skull base, bordered anteriorly by the maxilla (max sinus), posteriorly by the pterygoid base of the sphenoid, and medially by the perpendicular plate of the palatine bone. 2/22
The PTERYGOPALATINE FOSSA (PPF) is a space deep in the face/skull base, bordered anteriorly by the maxilla (max sinus), posteriorly by the pterygoid base of the sphenoid, and medially by the perpendicular plate of the palatine bone. 2/22 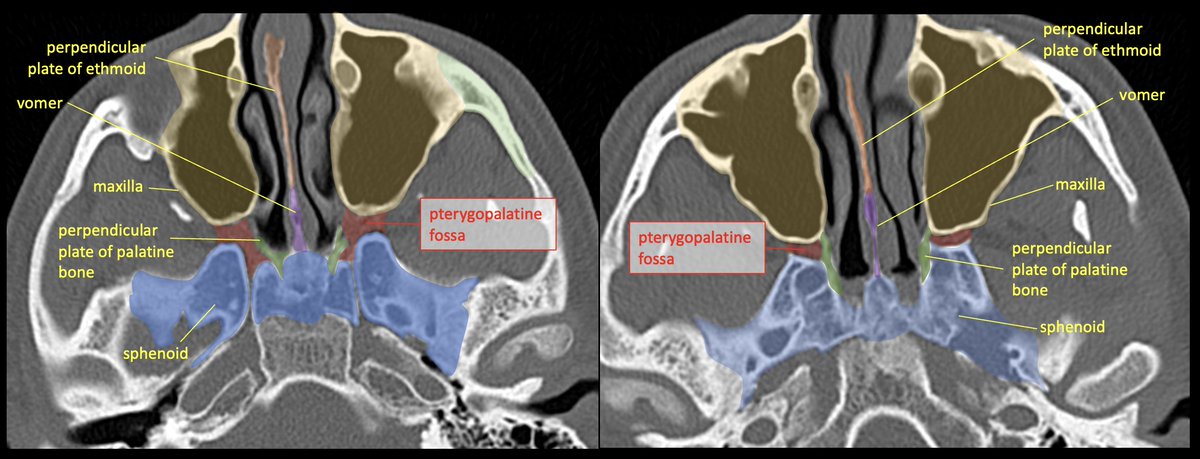
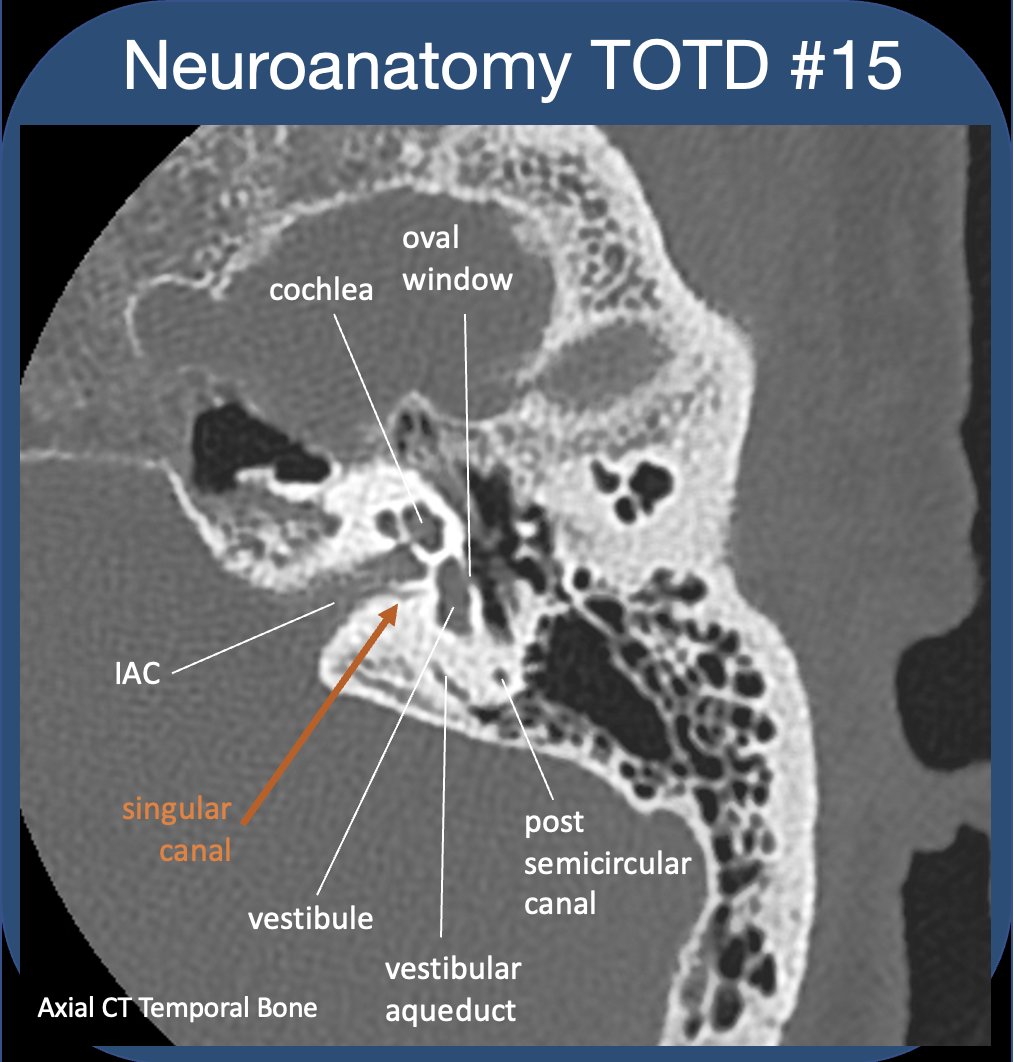 To evaluate the t-bone, best to compartmentalize--external/middle/inner ear (IE). See previous #tweetorial of the ME. The IE is difficult as most structures are obliquely oriented (at different obliquities!)-and can be hard to see on standard views. 2/24
To evaluate the t-bone, best to compartmentalize--external/middle/inner ear (IE). See previous #tweetorial of the ME. The IE is difficult as most structures are obliquely oriented (at different obliquities!)-and can be hard to see on standard views. 2/24
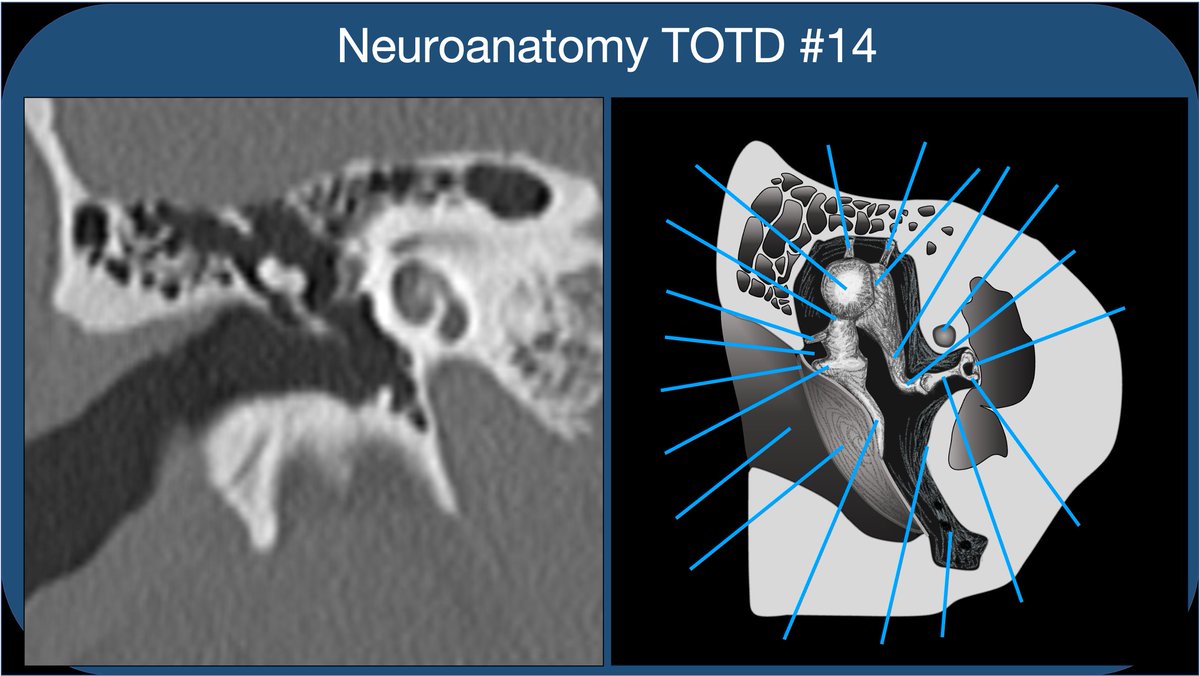 Whether learning t-bone anatomy as a medical student or evaluating a CT of the t-bone as a radres, it’s best to compartmentalize into external, middle, and inner ear. This thread🧵is on the middle ear: Inner ear to follow, some day:)
Whether learning t-bone anatomy as a medical student or evaluating a CT of the t-bone as a radres, it’s best to compartmentalize into external, middle, and inner ear. This thread🧵is on the middle ear: Inner ear to follow, some day:)
 Time for a deep dive into limbic networks. Bear with me—this is a fun subject. I got carried away preparing slides—it’s hard to know when to stop!
Time for a deep dive into limbic networks. Bear with me—this is a fun subject. I got carried away preparing slides—it’s hard to know when to stop! Facial motor nucleus is in the pontine tegmentum; axons loop dorsally around the abducens nucleus, then course anterolaterally, exiting the brainstem at the CPA.
Facial motor nucleus is in the pontine tegmentum; axons loop dorsally around the abducens nucleus, then course anterolaterally, exiting the brainstem at the CPA.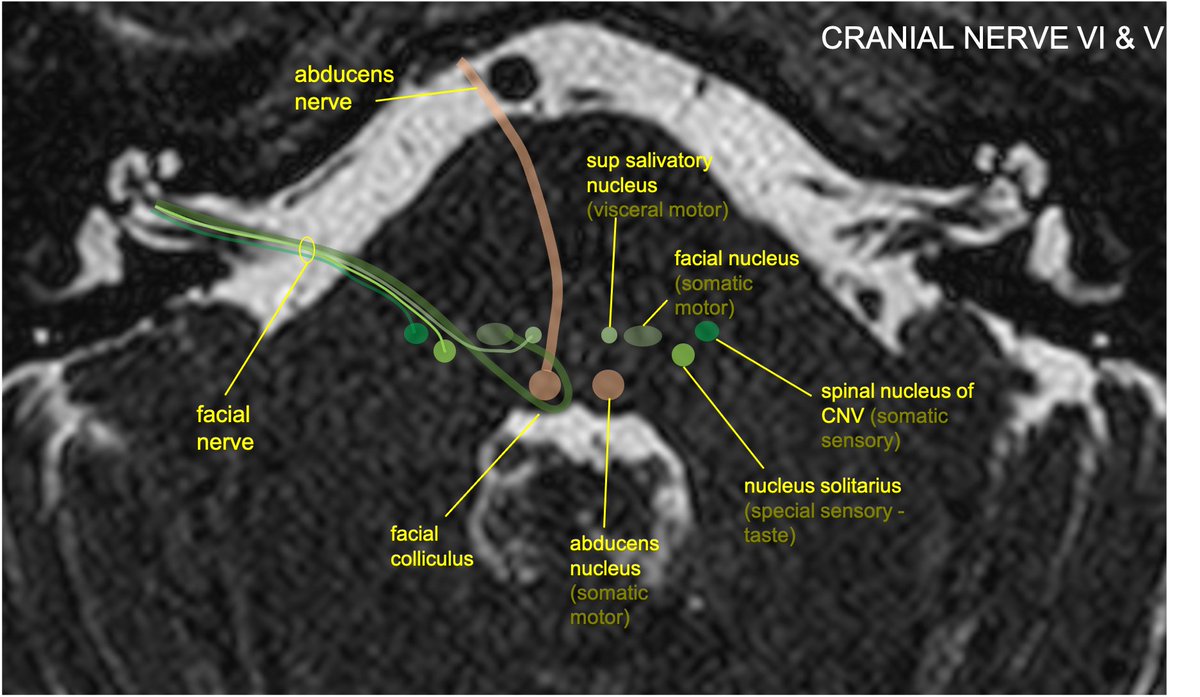
 2/5...The STN is functionally a node within the basal ganglia (BG) INDIRECT LOOP. STN contains excitatory glutaminergic neurons➞output to the GABA neurons of GPi, which in turn have inhibitory effect on thalamic outputs to the motor cortex.
2/5...The STN is functionally a node within the basal ganglia (BG) INDIRECT LOOP. STN contains excitatory glutaminergic neurons➞output to the GABA neurons of GPi, which in turn have inhibitory effect on thalamic outputs to the motor cortex. 
 2/6...Meckel’s cave (MC) is open to the subarachnoid space at its posterior margin (and is therefore filled with CSF). The trigeminal (Gasserion) ganglion lives in MC. Superiomedial to MC (and sharing a dural border), is the cavernous sinus. #radres #neurorad
2/6...Meckel’s cave (MC) is open to the subarachnoid space at its posterior margin (and is therefore filled with CSF). The trigeminal (Gasserion) ganglion lives in MC. Superiomedial to MC (and sharing a dural border), is the cavernous sinus. #radres #neurorad 
 2/8..The HC: complex structure of limbic system; encodes memories from short->long term (also involved in pattern recognition,memory encoding & association, working memory,spatial nav, emotional behavior,awareness of conscious knowledge). Am I missing anything neuroscientists?
2/8..The HC: complex structure of limbic system; encodes memories from short->long term (also involved in pattern recognition,memory encoding & association, working memory,spatial nav, emotional behavior,awareness of conscious knowledge). Am I missing anything neuroscientists?
 2/7...CN 3,6,V1 travel between two dural layers in the lateral wall of the CS. V2 often travels in the the inferolateral wall of the CS (sometimes inferior to the CS). Cranial nerve 6 floats freely in the CS (why CS pathology often selectively affects CN6).
2/7...CN 3,6,V1 travel between two dural layers in the lateral wall of the CS. V2 often travels in the the inferolateral wall of the CS (sometimes inferior to the CS). Cranial nerve 6 floats freely in the CS (why CS pathology often selectively affects CN6). 

 ICA segments: C1 (cervical) becomes C2 (petrous) in the carotid canal of the petrous bone. Becomes C3 (lacerum) as it exits the carotid canal above the foramen lacerum. Becomes C4 (cavernous segment above the petrolingual ligament through the cavernous sinus.
ICA segments: C1 (cervical) becomes C2 (petrous) in the carotid canal of the petrous bone. Becomes C3 (lacerum) as it exits the carotid canal above the foramen lacerum. Becomes C4 (cavernous segment above the petrolingual ligament through the cavernous sinus. 
 The AC runs across the midline in front of the anterior columns of the fornix, behind the basal forebrain and beneath the anterior limb internal capsule and basal ganglia, surrounded by the bed nucleus of the stria terminalis.
The AC runs across the midline in front of the anterior columns of the fornix, behind the basal forebrain and beneath the anterior limb internal capsule and basal ganglia, surrounded by the bed nucleus of the stria terminalis.
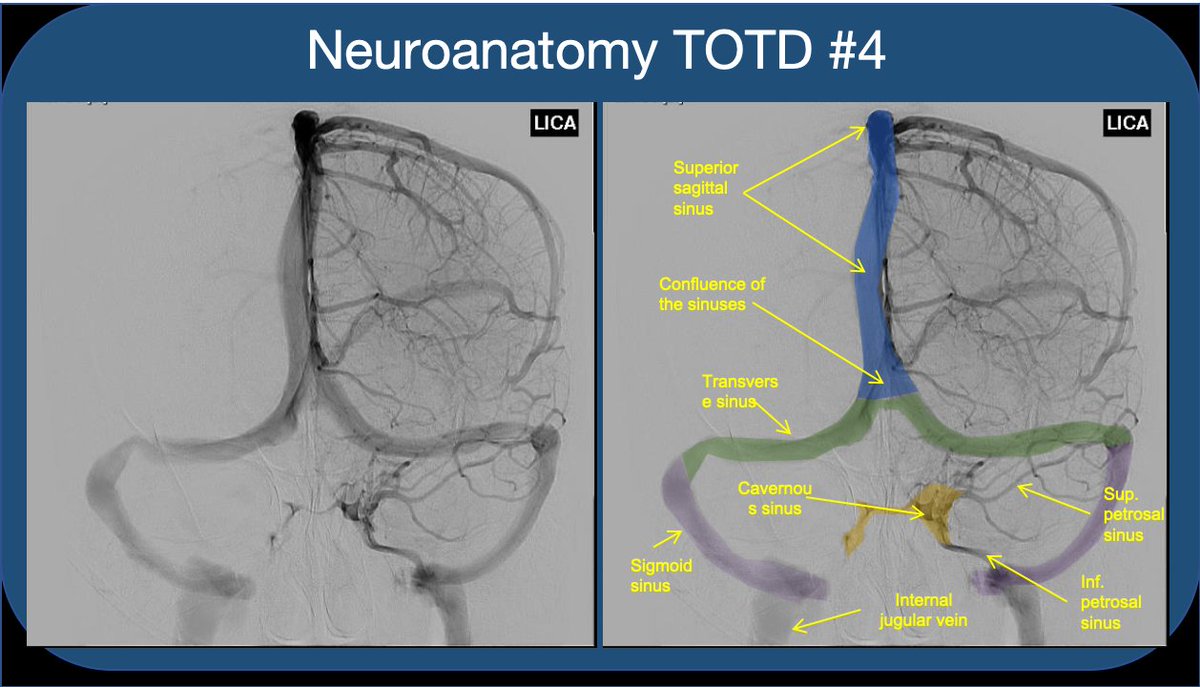 2/5 Note that the paired sinuses are often variably connected by “intercavernous sinuses”. While the CS is often taught for its relationship to the ICA and cranial nerves, I find that medical students and residents rarely understand the flow of blood through the sinus.
2/5 Note that the paired sinuses are often variably connected by “intercavernous sinuses”. While the CS is often taught for its relationship to the ICA and cranial nerves, I find that medical students and residents rarely understand the flow of blood through the sinus.
 2/6 "Upper T sign" or "L sign"
2/6 "Upper T sign" or "L sign"
 2/3 The term is used variably, when the bulk of PCA flow comes from the anterior circulation (internal carotids) via a robust post. communicating artery. Some reserve the term for when there is no connection to the posterior circulation (absent P1 segment from the basilar art.),
2/3 The term is used variably, when the bulk of PCA flow comes from the anterior circulation (internal carotids) via a robust post. communicating artery. Some reserve the term for when there is no connection to the posterior circulation (absent P1 segment from the basilar art.), 
 2/7 Preganglionic parasympathetic cell bodies are located in the superior salivatory nucleus of the pontine tegmentum, and exit the brainstem with CNVII (facial nerve) at the cerebellopontine angle (-->IAC-->temp bone).
2/7 Preganglionic parasympathetic cell bodies are located in the superior salivatory nucleus of the pontine tegmentum, and exit the brainstem with CNVII (facial nerve) at the cerebellopontine angle (-->IAC-->temp bone).