"Coronavirus: T-cell immunity exists six months after infection, study finds" - Sky
This must come as quite a shock. Who'd have thought there could be more to immunity than antibody levels?
Of course that's not the whole article...
This must come as quite a shock. Who'd have thought there could be more to immunity than antibody levels?
Of course that's not the whole article...

The article goes on to say...
"But the researchers, from Public Health England and the UK Coronavirus Immunity Consortium, warn that it's still not clear whether the T-cell levels were high enough to protect against re-infection."
"But the researchers, from Public Health England and the UK Coronavirus Immunity Consortium, warn that it's still not clear whether the T-cell levels were high enough to protect against re-infection."

I suggest refering to known science as a starting point. There used to be quite a lot of it around, although we seem to have mislaid it recently.
To be cautious though I suggest (seriously) this:
1) Treat as true the commonly declared hypothesis that "only people with measurable levels of antibodies have immunity".
2) Work out what should happen if that is the case.
3) Test your predictions against observed reality.
1) Treat as true the commonly declared hypothesis that "only people with measurable levels of antibodies have immunity".
2) Work out what should happen if that is the case.
3) Test your predictions against observed reality.
4) Do you see what you should see?
If YES: Your hypothesis may be correct (although never 100%; another conversation).
If NO: Your hypothesis regarding immunity from #SARS_CoV_2 is wrong.
This video, half a century old, summarise the idea beautifully.
If YES: Your hypothesis may be correct (although never 100%; another conversation).
If NO: Your hypothesis regarding immunity from #SARS_CoV_2 is wrong.
This video, half a century old, summarise the idea beautifully.
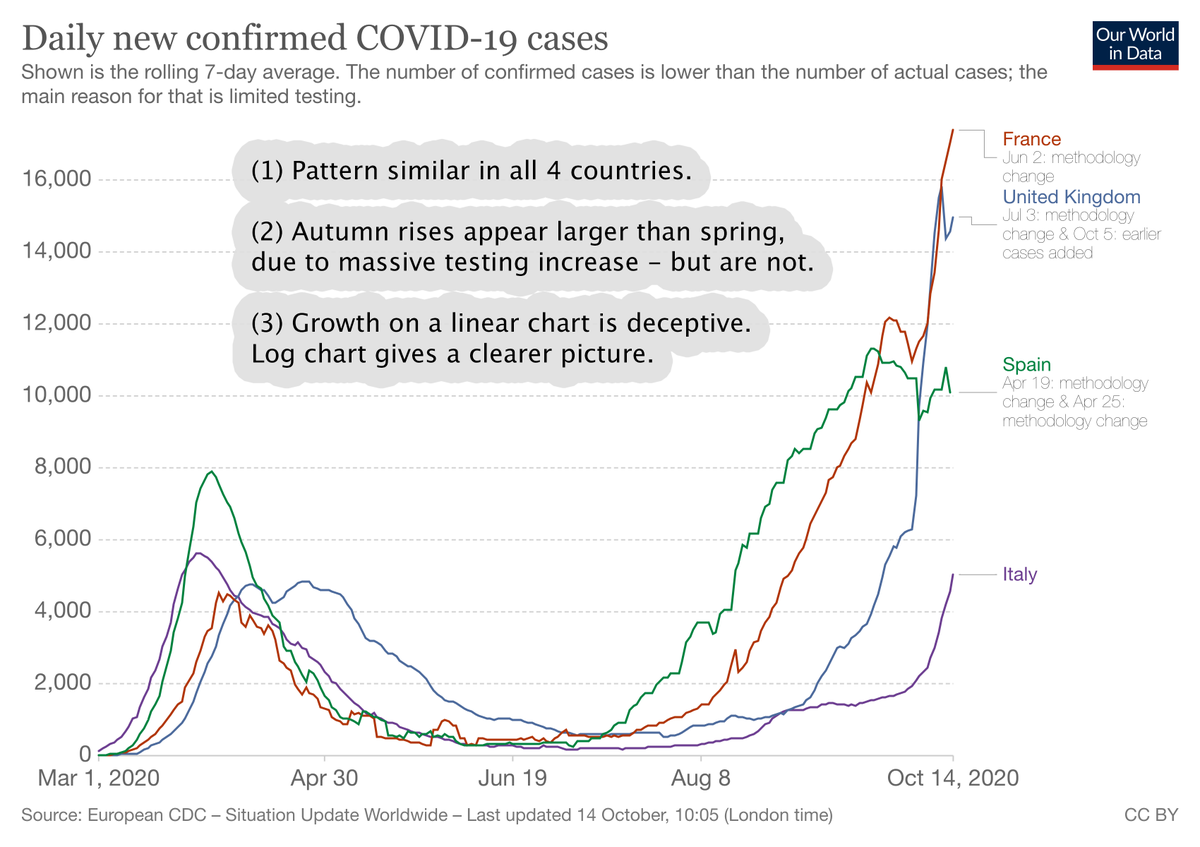
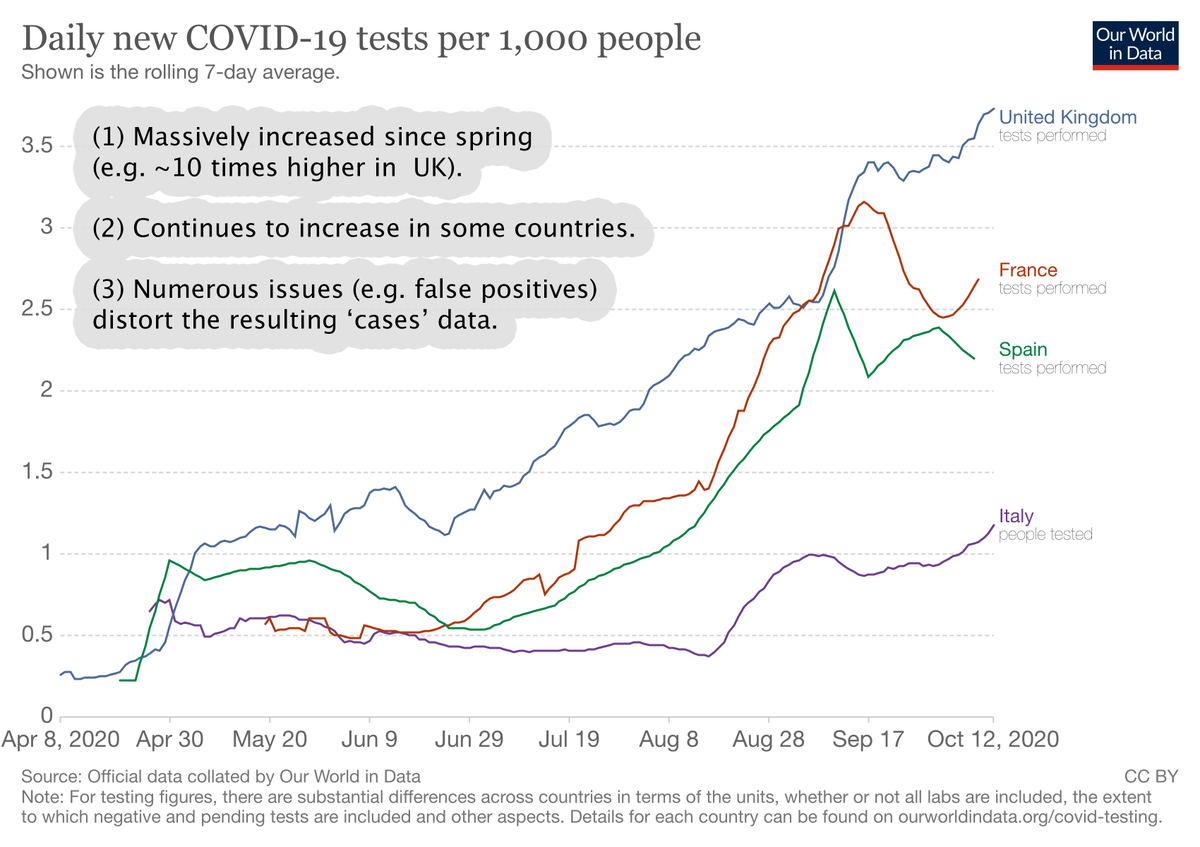
The recent ICL study re declining antibody levels provides an opportunity to examine the hypotheses that only measurable levels of antibodies provide effective immunity. See attached. When checked against reality this hypothesis appear to be wrong.
https://twitter.com/RuminatorDan/status/1321457800724307968?s=19
Link to source Sky News article:
news.sky.com/story/amp/coro…
news.sky.com/story/amp/coro…
@threadreaderapp unroll
• • •
Missing some Tweet in this thread? You can try to
force a refresh