A few thoughts on these interpretations, that appear to suggest (with caveats) that schools in England haven't necessarily contributed much to transmission. The evidence presented here does not necessarily support this. A thread.
https://twitter.com/apsmunro/status/1324762913631068161
The lower number of cases identified among 0-10 yr olds ignores the fact that we know that children are likely to be asymptomatic and mildly symptomatic, which means that symptom-based testing is likely to vastly underestimate infections in this age group
https://twitter.com/apsmunro/status/1324762918504878081?s=20
There have been significant clusters of infection of COVID-19 identified in schools (both primary and secondary). These form the majority of clusters of acute respiratory incidents identified related to COVID-19 since September.
https://twitter.com/apsmunro/status/1324762923986788355?s=20
While some of this may be down to cluster detection being better in schools than in other settings it does suggest that clustered outbreaks are occurring in schools, suggesting that transmission does occur in the school setting.
ONS survey data (testing a random sample of individuals, so picking up asymptomatic and presymptomatic infection as well) has consistently suggested similar prevalence in children as with adults, as shown in the graph, so children to get infected at similar rates.
The flattening of cases in school age children prior to lockdown is interesting, as this occurs about a wk following half-term suggesting these might be effects related to school closure. But of course correlation is not necessarily causation.
https://twitter.com/apsmunro/status/1324762930613768193?s=20
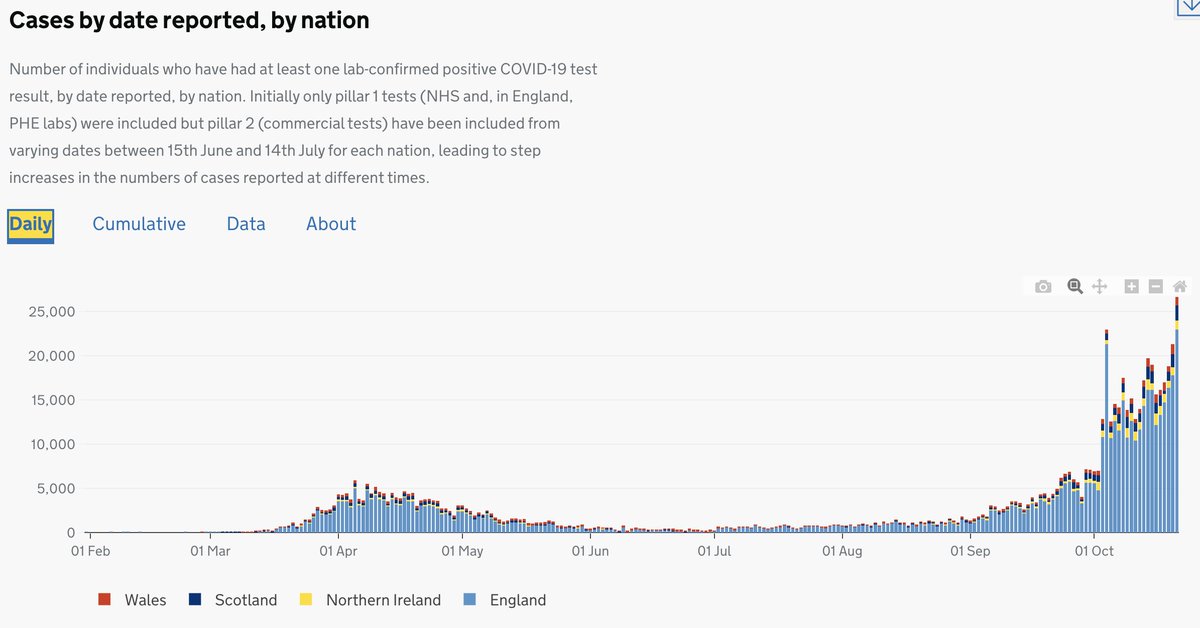
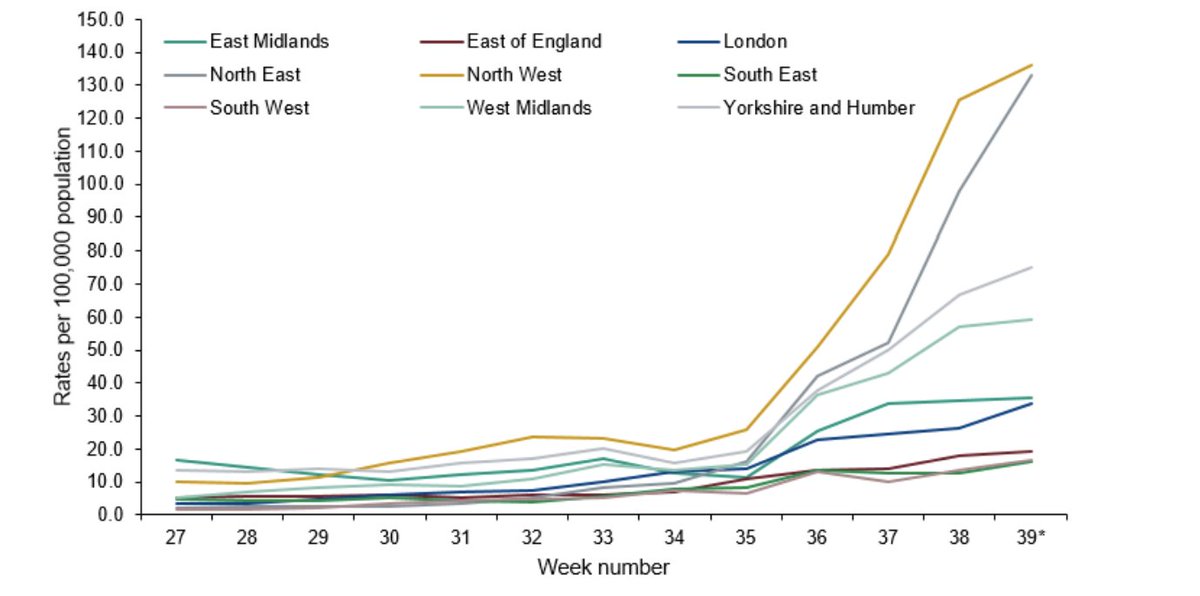
This inference is problematic. Overall cases have been rising in England steadily since August, but the rapidity of rise is important. There is actually fairly strong evidence of transmission in university towns being higher and more rapid across the UK.
https://twitter.com/apsmunro/status/1324762937790238727?s=20
The pandemic appears to accelerate in September. Again correlation is not causation, but it's not appropriate to say that schools did not contribute to transmission. They may well have, and the data showing steady rises prior to school openings certainly doesn't rule this out.
That teachers may be at similar risk to other key workers is not reassuring. Other key workers here include patient facing HCWs. If anything, this suggests that teachers are at high risk. Also these data come with high levels of uncertainty (large CIs)
https://twitter.com/apsmunro/status/1324767835508408324?s=20
Global evidence supports the role of children in transmission & schools are a setting that shouldn't be overlooked. Minimising this risk despite accruing evidence prevents us putting in place important measures to deal with this.
mja.com.au/journal/2020/c…
mja.com.au/journal/2020/c…
We all want to ensure children's education and wellbeing. The best way to do this is not to minimise the potential risk, but rather respond to it with clear guidance to ensure children, staff and communities are safe, as other countries have done.
Sorry just to clarify, by 'minimise', I meant 'dismiss' rather than minimising transmission and risk, which we do really want to do!!
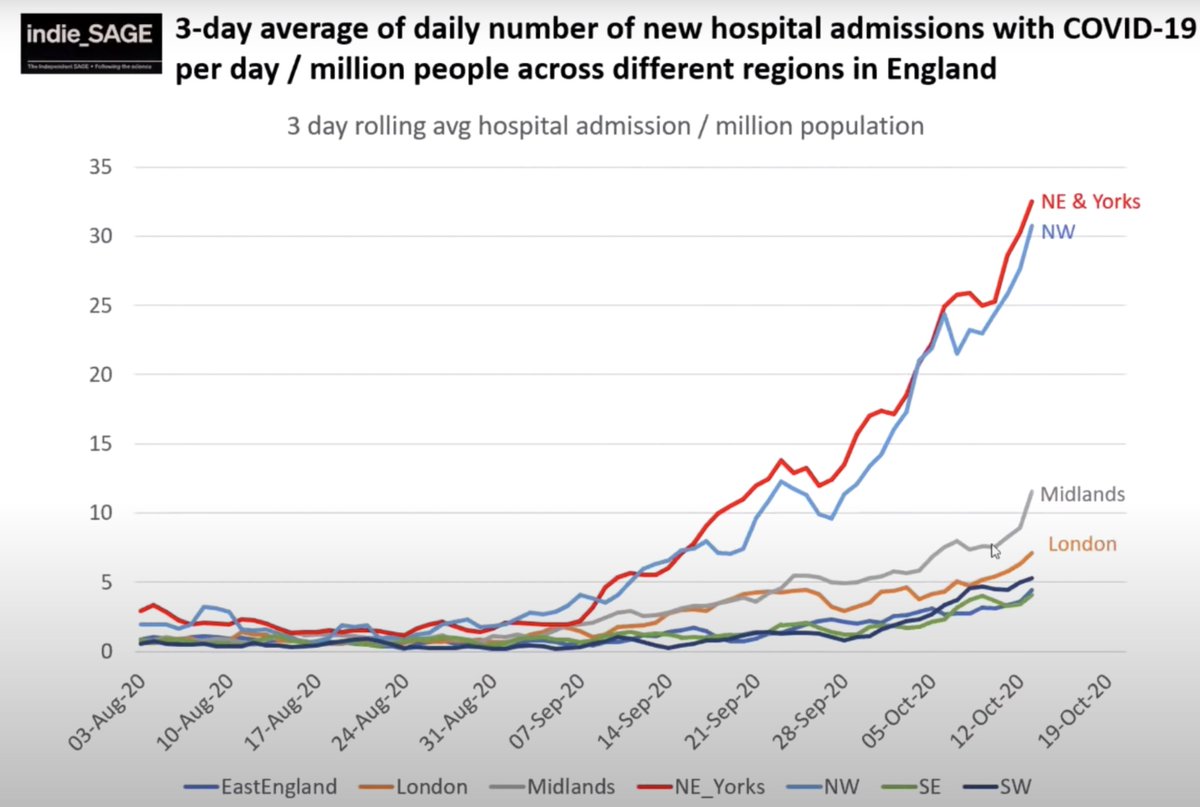
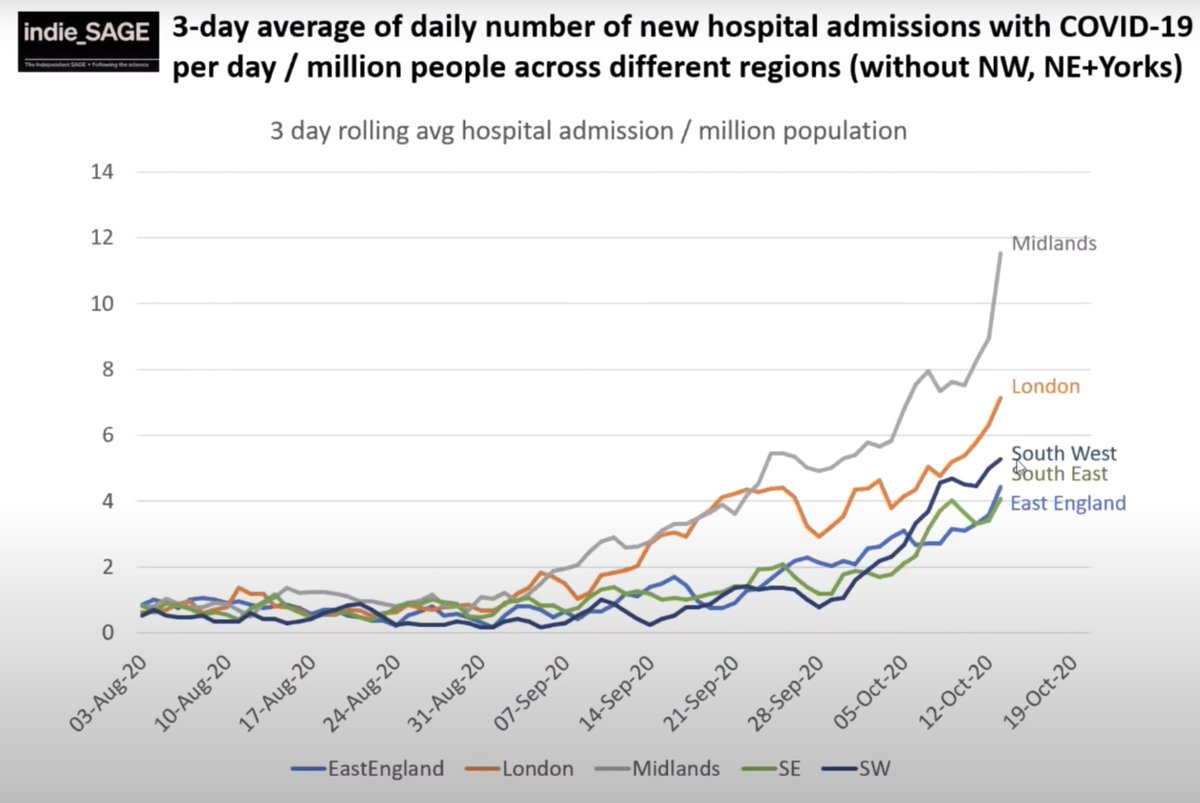
Also, want to point out that we don't expect a 2-3 wk lag between school openings and increases in transmission. We expect to see this in a week or two. 2-3 wks is the time from infection to hospitalisation, not symptoms.
• • •
Missing some Tweet in this thread? You can try to
force a refresh