
Moving in right direction to reverse outbreaks
Here's how:
At-home frequent rapid tests
10M/day ->
pool 2 ppl/test ->
20M ppl tested/day ->
Ea house tests 1x/wk ->
140M ppl tested/wk!! ->
Herd effects: R << 1 ->
RAPIDLY SLOWS SPREAD in US
1/
medtechdive.com/news/bidens-co…
Here's how:
At-home frequent rapid tests
10M/day ->
pool 2 ppl/test ->
20M ppl tested/day ->
Ea house tests 1x/wk ->
140M ppl tested/wk!! ->
Herd effects: R << 1 ->
RAPIDLY SLOWS SPREAD in US
1/
medtechdive.com/news/bidens-co…
This plan can work with only 10M paper strip antigen tests per day in whole of US
US Govn't can produce / fund these tests. Ship to participating households. 20 paper strip tests per household...
3 are different (but look same) and are for rapidly confirming positives.
2/
US Govn't can produce / fund these tests. Ship to participating households. 20 paper strip tests per household...
3 are different (but look same) and are for rapidly confirming positives.
2/
We do NOT need all people to "buy into" the program. These tests are used in private (think... next to toothbrush) and need only half of a community to decide to participate.
So if 50% of people don't want to - they don't need to. Not mandatory... the plan still works!
3/
So if 50% of people don't want to - they don't need to. Not mandatory... the plan still works!
3/
Those households that do participate - they do so and use the test 1x/week (or for much faster community results - we get 20M tests/day and use 2x/week per house).
The point is to use them FREQUENTLY so people are likely to find themselves BEFORE they transmit to others.
4/
The point is to use them FREQUENTLY so people are likely to find themselves BEFORE they transmit to others.
4/
People have said these tests aren't sensitivity enough compared to PCR. This simply is not true. It's a misunderstanding. These tests ARE PLENTY SENSITIVE to catch almost everyone who is currently transmitting virus.
5/
5/
People have said these tests aren't specific enough and there will be false positives... in most recent BinaxNOW rapid test studies, false positive rate has been ~1/400.
In this plan we add a few confirmatory tests... this will make the rate of false positives miniscule
6/
In this plan we add a few confirmatory tests... this will make the rate of false positives miniscule
6/
People have said we need to ensure reporting... NOT so. Here, we scale up testing first. Once we have a LOT of people tested per week (i.e. 140 million in this plan) then we have "single click" voluntary reporting. If you're positive, simple to report if you want....
7/
7/
We can choose to have i) perfect reporting of a relatively small number of infrequently used tests that have slow turnaround times, OR ii) we can have imperfect reporting of a LOT of rapid tests
Choice (ii) will provide MORE data, not less, to public health authorities
8/
Choice (ii) will provide MORE data, not less, to public health authorities
8/
With nearly half of the country testing themselves weekly, incredibly... we do not need to rely on contact tracing... which is largely to figure out who to test and isolate (And it generally isn't working great).
Here the frequent rapid at-home tests ARE the intervention
9/
Here the frequent rapid at-home tests ARE the intervention
9/
The tests ARE the intervention because they let people know they are infected WHEN they are infectious. And then people isolate for 10 days... or since that's burdensome for many... at LEAST until they have been negative for 48 hours... often < 10d.
10/
10/
Some will say "Some people may not isolate"... yes... that's true - Some won't
But some won't with PCR/Test/Trace/Isolate as well. We don't handcuff people home
Here, this is more personal. They are testing themselves and SEE they are positive. Most POSITIVES will isolate
11/
But some won't with PCR/Test/Trace/Isolate as well. We don't handcuff people home
Here, this is more personal. They are testing themselves and SEE they are positive. Most POSITIVES will isolate
11/
This is NOT an "Entry Screen"... this is a "Public Health Screen"
The goal is NOT to stop every case. The goal is to stop every outbreak. Slow it down, get R << 1, and let the outbreak die out.
So far we've been trying to stop outbreaks by focusing on stopping cases..
12/
The goal is NOT to stop every case. The goal is to stop every outbreak. Slow it down, get R << 1, and let the outbreak die out.
So far we've been trying to stop outbreaks by focusing on stopping cases..
12/
We need to shift our focus - away from thinking of this as a lot of medical problems, to thinking about this as one big public health problem
If we focus on stopping OUTBREAKS and not individual cases, we realize the full power of frequent rapid at home testing...
13/
If we focus on stopping OUTBREAKS and not individual cases, we realize the full power of frequent rapid at home testing...
13/
In this program, it is not a big deal if the test misses someone - remember, 50% of people are choosing not to participate at all!!
Here, the goal is to suppress the outbreaks by driving R <<1. So that in weeks outbreaks have dropped dramatically and everyone becomes safer
14/
Here, the goal is to suppress the outbreaks by driving R <<1. So that in weeks outbreaks have dropped dramatically and everyone becomes safer
14/
We see a TREMENDOUS example of the power of frequent rapid tests in Slovakia
Slovakia is testing ~50% ppl 1x/wk
In the first week alone the incidence of #COVID19 dropped ~50%!
We CAN do this in the US too!!
It takes a plan, strategy, coordination, and funding.
15/
Slovakia is testing ~50% ppl 1x/wk
In the first week alone the incidence of #COVID19 dropped ~50%!
We CAN do this in the US too!!
It takes a plan, strategy, coordination, and funding.
15/
Also -we must ensure income for anyone who needs to isolate. This is an absolute must.
We must have a LOT of high quality messaging - on web/tv/radio - like wartime messaging to make sure everyone understands the purpose, goals, how to test, etc
We can do this!
16/16
We must have a LOT of high quality messaging - on web/tv/radio - like wartime messaging to make sure everyone understands the purpose, goals, how to test, etc
We can do this!
16/16
Finally - to clarify - this is the plan I envision. I HOPE the Biden team will take it and run with it - or some version of it.
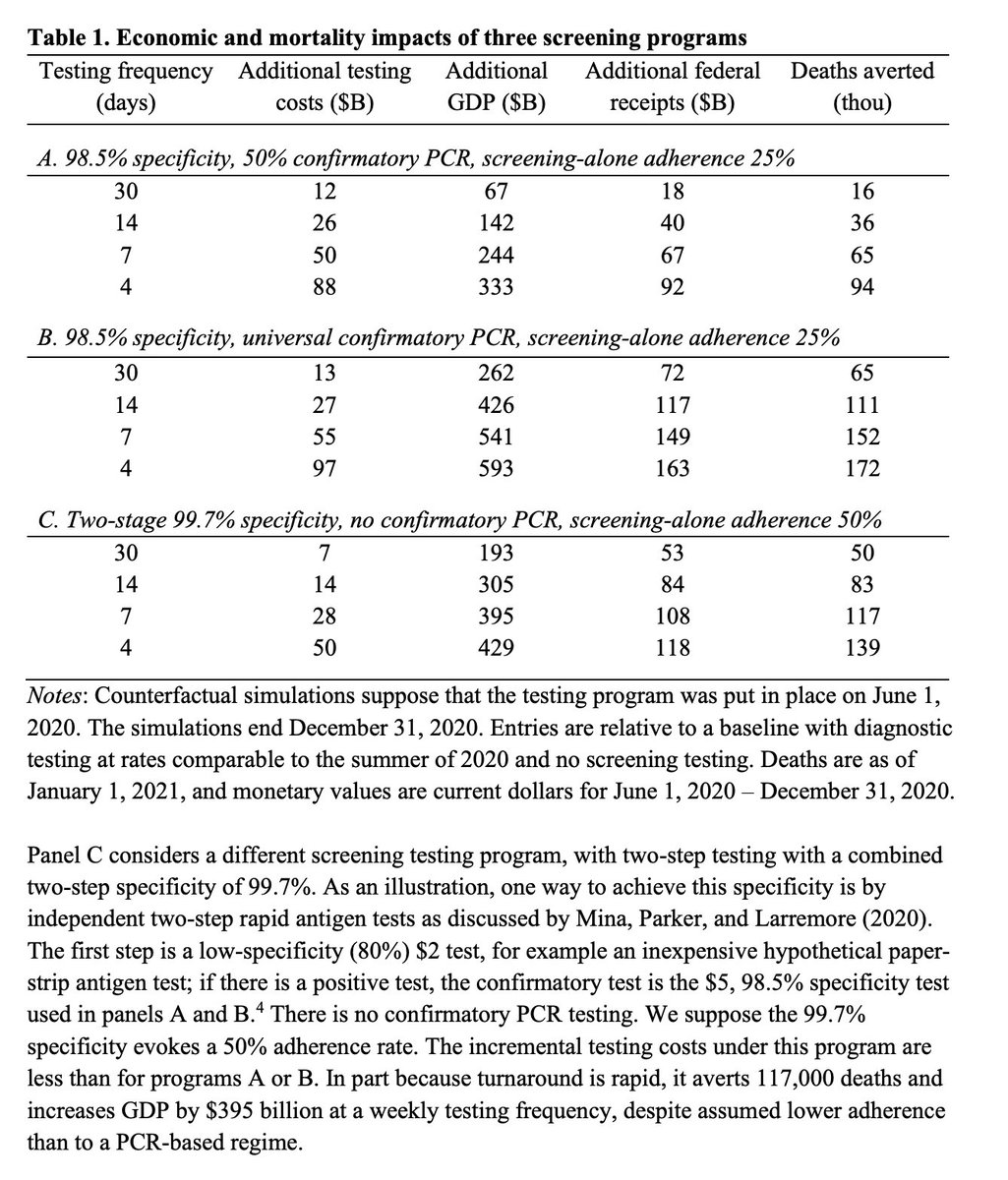
Also - Here is what would happen if we implemented this program! (Note, we mistakenly labeled this "surveillance" but it should be "screening".
This comes from a soon to be formally published pre-print:
medrxiv.org/content/10.110…
This comes from a soon to be formally published pre-print:
medrxiv.org/content/10.110…

Here, we evaluated the economic return on investment of this plan had we started in June - Dec 2020.
The version described above is shown in panel C
Costs (all included) $28B
Would have increased GDP by $395B!
Would have saved >100,000 lives in 2020!
medrxiv.org/content/10.110…
The version described above is shown in panel C
Costs (all included) $28B
Would have increased GDP by $395B!
Would have saved >100,000 lives in 2020!
medrxiv.org/content/10.110…
Here is a news report on the efforts in Slovakia to drop incidence by 50% through widescale testing of their population in a short amount of time.
usnews.com/news/world/art…
usnews.com/news/world/art…
And here is a paper we wrote describing why, for a program like this, we needn't worry about low analytical sensitivity and instead must prioritize sensitivity to detect infectious people....
nejm.org/doi/full/10.10…
nejm.org/doi/full/10.10…
If worrying that rapid tests miss a lot of people at start of infection - This paper tracked regular people over time to see if they turn positive. Note incredibly fast upswing in virus titers! Frequency, not sensitivity at the limit of PCR is needed.
medrxiv.org/content/10.110…
medrxiv.org/content/10.110…
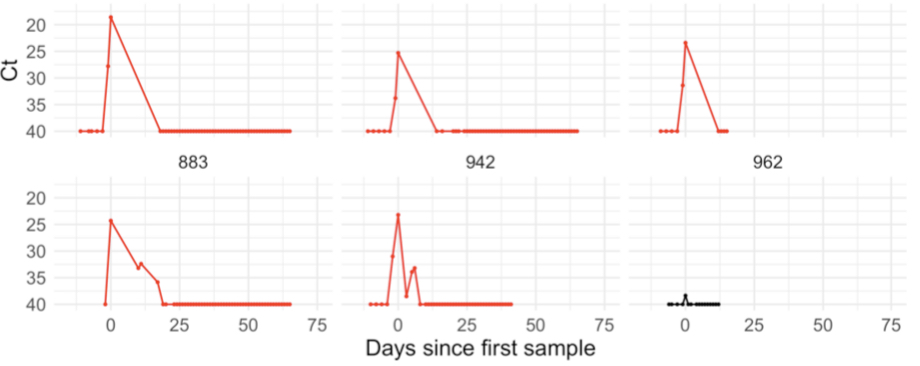
In other words, the time difference is minimal between when ppl 1st turn PCR pos and when they turn rapid antigen positive.
It is MUCH better to prioritize frequency and turnaround time over PCR type sensitivity b/c within hours of PCR turning pos, the viral load is sky high.
It is MUCH better to prioritize frequency and turnaround time over PCR type sensitivity b/c within hours of PCR turning pos, the viral load is sky high.
Oh. Also recognize that that plot of virus titers is a log scale. Every 3.3 Ct values is a 10-fold change. So 40-30 is a 1000x increase in virus titers.
• • •
Missing some Tweet in this thread? You can try to
force a refresh




