
I'm now logging into #ISPOREurope live session IP3: The Meaning of Cure – the Search for What? with @NRLatimer, @BettinaRyll, and K. Jack Ishak and Ágnes Benedict from @evideraglobal ispor-europe2020.secure-platform.com/a/gallery/roun… 
Jack Ishak starts by introducing panellists and setting the motivation for this panel: therapies that have raised the potential of cure, given the plateau since in the OS and PFS curves
#ISPOREurope
#ISPOREurope
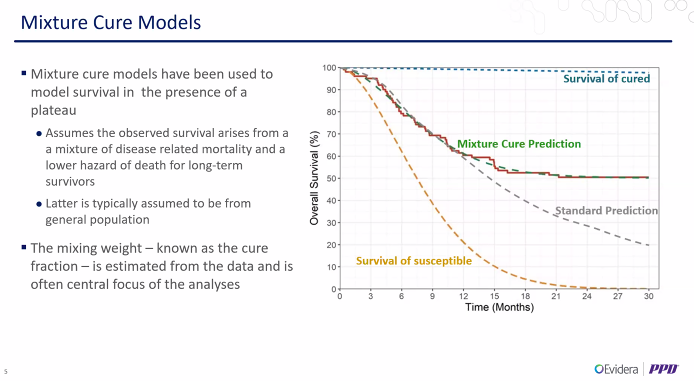
This raises analytical challenges on how to project the OS and PFS curves over the long term. Mixture cure models have been used. Here, the curve is a weighted average of the survival of cured and uncured, where the weight is prop cured.
#ISPOREurope
#ISPOREurope
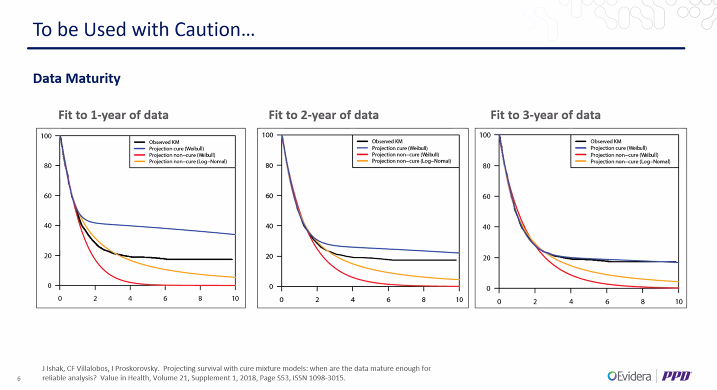
But mixture cure models have limitations and challenges. One impt issue is the impact of data maturity. In simulations re. maturity of data, with early cuts of data, the MCM fit was poorer, with lognormal fit doing a reasonable job --> MCM sensitive to maturity
#ISPOREurope
#ISPOREurope
The focus of this session is how to define cure, as cure in the analysis is really a statistical definition of cure, based on the population rather the individual. There is not necessarily clinical confirmation of cure. So is this curative effect meaningful?
#ISPOREurope
#ISPOREurope
Agnés from @evideraglobal starts with the industry perspective. She interviewed #HEOR colleagues about 3 questions: definition of cure (population vs individual level), value of cure and what data can support cure given the follow-up of the trial.
#ISPOREurope
#ISPOREurope
The def of cure depends on the disease area. From a clinical point of view, and in terms of cancer, clinicians tend to shy away to saying that pts are cured. Cure is discussed in immuno-oncology therapies. Not in the metastatic setting. Term used in the stats context
#ISPOREurope
#ISPOREurope
In genetic diseases, "cure" is avoided, although used in editorials and pt forums, not clinical trials. Functional cure is discussed but in functional terms
#ISPOREurope
#ISPOREurope
In infection diseases, "cure" is defined and standardised as in the example in #HepatitisB. Here, idealistic vs realistic functional cure were defined. Could this approach be applied to other disease areas?
#ISPOREurope
#ISPOREurope
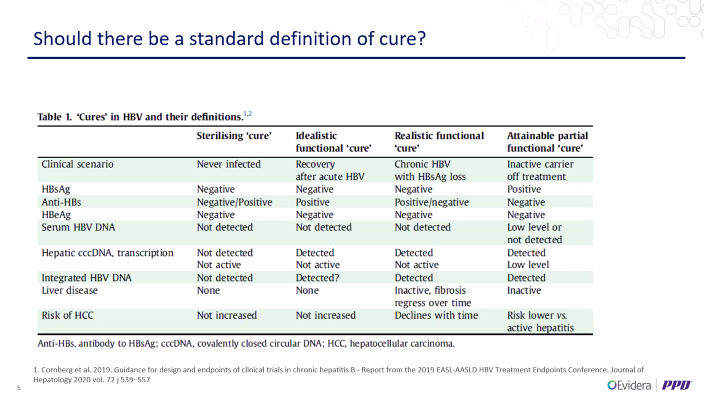
In this example, the cure was defined a priori, is the primary outcome of the trial, it is detectable at the individual, and is based on how good a surrogate outcome is at the population level
#ISPOREurope
#ISPOREurope
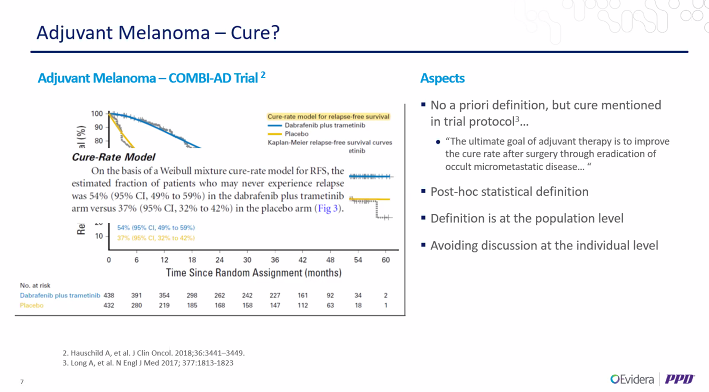
E.g. of adjuvant melanoma, where the authors presented a MCM based on relapse-free survival. Here the authors were careful not using the term "cure" but used the termed "fraction of patients who never experienced the event"
#ISPOREurope
#ISPOREurope
All #HEOR interviews suggested that the value of cure is larger than what is currently measured, but it is difficult to pin down.
This may be due to PROs, which are v reflective of chemotherapy era
#ISPOREurope
This may be due to PROs, which are v reflective of chemotherapy era
#ISPOREurope
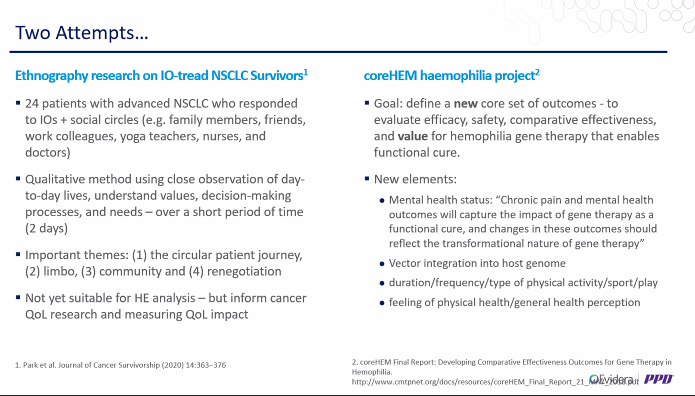
2 attempts to measure the added value of cure: one study in NSCLC, and another on haemophillia, where the goal was to define outcomes to reflect the transformational value of functional cure
#ISPOREurope
#ISPOREurope
Next up @NRLatimer at #ISPOREurope.
We're thinking about cure models because treatments are offering potential cures. If some people are likely to be cured, we should reflect this.
We're thinking about cure models because treatments are offering potential cures. If some people are likely to be cured, we should reflect this.
However, there are perils to this, and @NRLatimer refers us to a movie about this. In the movie, there are plateaus in the KMs, although the numbers at risk are very small. The boss insists that the MCM is used for the HTA model.
#ISPOREurope
#ISPOREurope
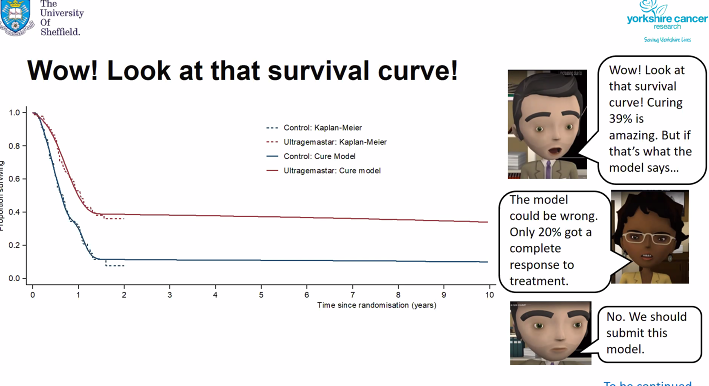
To know the rest of the story, have a look at the movie
How much difference does using a cure model make? A large difference.
Which cure model to use? It can also make a big difference.
If we are to use cure models, need to think carefully about how to specify them
#ISPOREurope
Which cure model to use? It can also make a big difference.
If we are to use cure models, need to think carefully about how to specify them
#ISPOREurope
The cure fraction is crucial. It might not be possible to estimate it based on short-term small RCTs. But we also need to justify the cure fraction.
#ISPOREurope
#ISPOREurope
Another impt aspect is the QoL: is it fully restored? are "cure" people at increased risk of death? what about resource use?
#ISPOREurope
#ISPOREurope
Also not just about "cure" models. For HTA, we wnat to accurately model long-term survival. If there are long-term QALY benefits, they will accrue even if we don't classify them as arising from cure
#ISPOREurope
#ISPOREurope
We do need to define the characteristics of "long-term survivors", namely QoL, risk of death and resource use. Modelling these long-term benefits doesn't necessarily need a cure model
#ISPOREurope
#ISPOREurope
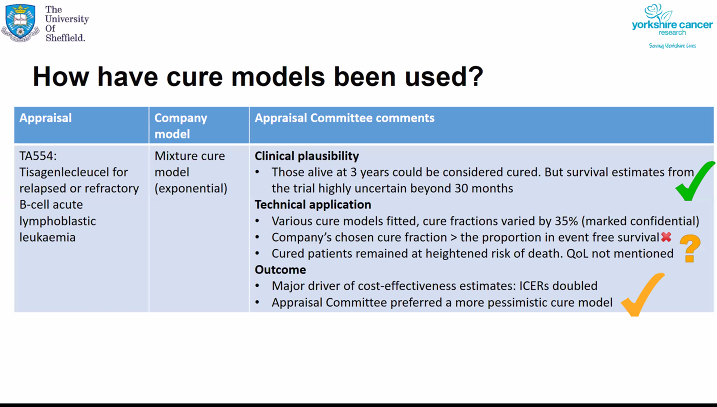
How have cured models been used? E.g. TA554 on a CAR T-cell therapy. The committee thought that cure was plausible, but different cure models gave different cure fractions, and preferred a model which gave a lower cure fraction than submitted by the manufacturer
#ISPOREurope
#ISPOREurope
To sum up: it makes sense to think about cure models, but cure does not need to be assumed to model large QALY gains. Cure or long-term survivorship always needs the definition of what it means for QoL and resource use.
#ISPOREurope
#ISPOREurope
It might not be possible to fit standard cure models reliably given the data, so potential for Bayesian framework. For NICE TAs, clinical plausibility is crucial
#ISPOREurope
#ISPOREurope
Next up at #ISPOREurope is @BettinaRyll with the patients' perspective.
In 2011, melanoma 5-year OS was v low, whereas nowadays treatments that offer high OS at 5 years is close to a miracle.
In 2011, melanoma 5-year OS was v low, whereas nowadays treatments that offer high OS at 5 years is close to a miracle.
Immunotherapies are different from the traditional chemotherapy, because it targets the cancer indirectly via the immune system. Immune system is highly complex and its response depends on many factors
#ISPOREurope
#ISPOREurope
Back in 2010, ipilimumab for metastatic melanoma was an exciting new therapy, with a tail at around 20% OS. It might not look impressive from HTA viewpoint, but it is valuable to patients
#ISPOREurope
#ISPOREurope
There is a lot of discussion calling for mature OS data, rather than thinking about the patients' perspective. Patients need to chose a therapy today, given the information available today
#ISPOREurope
#ISPOREurope
We tend to look at "cure" as it was outcome of a single intervention, while the cure is the result of the treatment pathway. Bettina would like to see a more accurate reflection of the impact of pathway on the outcome.
#ISPOREurope
#ISPOREurope
In sum, we need early scientific - HTA dialogues, we need effective models combining access with evidence generation, and it is time to future proof HTA #ISPOREurope
Now at #ISPOREurope, it is time for the audience's questions!
Q: What are the panel's thoughts about Bayesian model averaging?
A: @NRLatimer thinks it's a good idea to incorporate structural uncertainty in the model distribution but the question is how to weight the models
Q: What are the panel's thoughts about Bayesian model averaging?
A: @NRLatimer thinks it's a good idea to incorporate structural uncertainty in the model distribution but the question is how to weight the models
Sometimes it is done based only on stats measures of fits, which is unlikely to be appropriate as the question is in the extrapolation.
#ISPOREurope
#ISPOREurope
Q: Rather than thinking about cure vs no cure, would it be better to think in terms of poor or better prognosis
A: @NRLatimer considers that this is related to having a MCM or a mixture model, which depends on the specific case
#ISPOREurope
A: @NRLatimer considers that this is related to having a MCM or a mixture model, which depends on the specific case
#ISPOREurope
Q: In a MCM, we assume that cured patients are cured at day zero. What are the implications?
A: @BettinaRyll says it depends on context & what else influences the model.
#ISPOREurope
A: @BettinaRyll says it depends on context & what else influences the model.
#ISPOREurope
A: @NRLatimer says that #RWD may help with estimating more realistic models to give a better idea of the shape of the survival distribution
The cure assumption in MCM from day zero is unlikely to be appropriate as doesn't reflect the pts' experience
#ISPOREurope
The cure assumption in MCM from day zero is unlikely to be appropriate as doesn't reflect the pts' experience
#ISPOREurope
My take: MCM not miracle cure for our statistical woes in extrapolating OS. Key to understand what long-term survival means in risk of death, progression, QoL and resource use. Dialogue with pts essential in getting this right
#ISPOREurope
#ISPOREurope
• • •
Missing some Tweet in this thread? You can try to
force a refresh














