Neuroanatomy TOTD #12
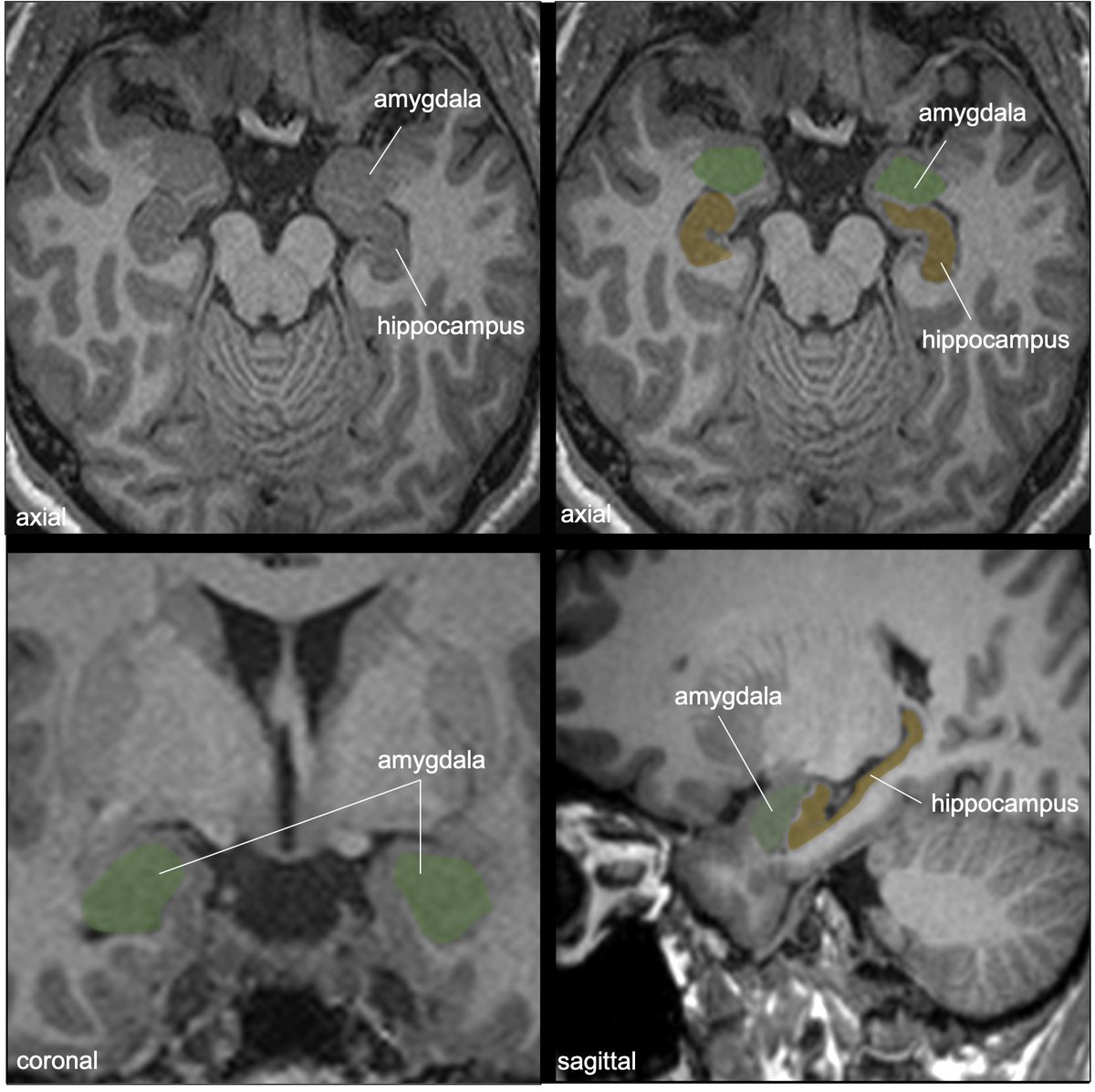
The green structure is the amygdala (amygdaloid body) and the yellow structure is the stria terminalis (ST).
1/18
#meded #FOAMed #FOAMrad #medtwitter #medstudents #radiology #neurorad #radres #neurology #neurosurgery #neuroanatomy #neuroanatomyTOTD
The green structure is the amygdala (amygdaloid body) and the yellow structure is the stria terminalis (ST).
1/18
#meded #FOAMed #FOAMrad #medtwitter #medstudents #radiology #neurorad #radres #neurology #neurosurgery #neuroanatomy #neuroanatomyTOTD

Time for a deep dive into limbic networks. Bear with me—this is a fun subject. I got carried away preparing slides—it’s hard to know when to stop!
2/18
2/18
The amygdala is an almond-shaped collection of gray nuclei/subnuclei deep to the uncus and ant to hippocampus in the med temporal lobe. Involved in multiple functions: memory modulation, emotional learning and responses, +important connections w/ the olfactory bulb/cortex.
3/18
3/18
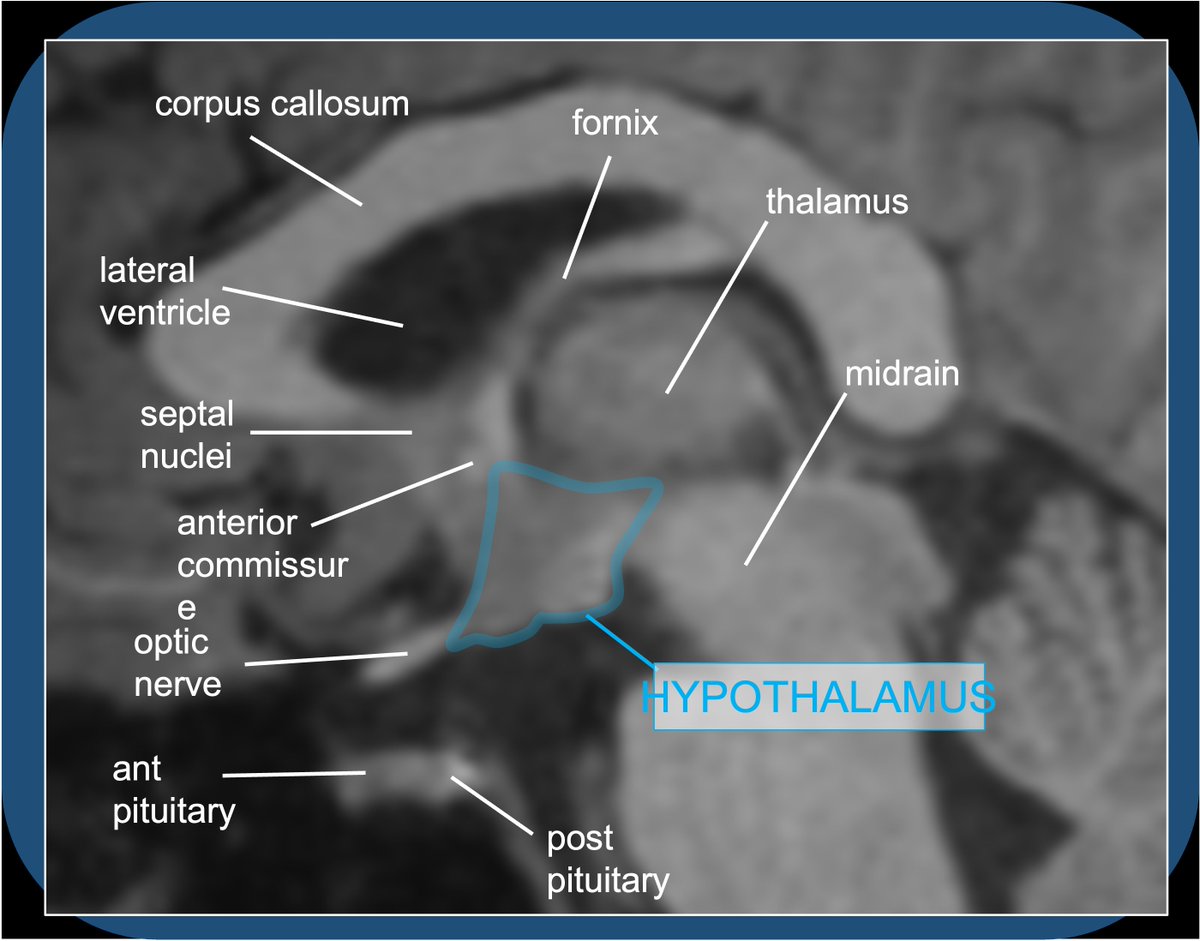
The stria terminalis (ST) is mainly an efferent pathway connecting amygdala to the septal area/basal forebrain and hypothalamus. It is poorly myelinated (notice it’s gray on T1 imaging), 2-4 mm in diameter. It also caries some afferents from the hypothalamus to amygdala.
4/18
4/18

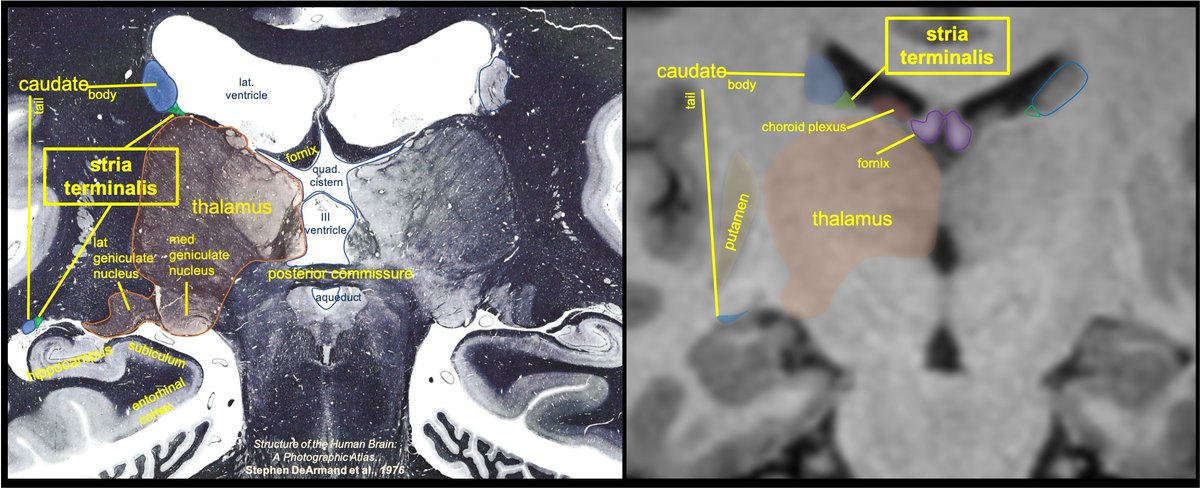
ST emanates from the amygdala adjacent to the hippocampal fimbria, and extends posteriorly along the roof of the temporal horn medial to the caudate tail. The proximal ST is not well seen on imaging--not distinguished from the fimbria, caudate tail, and choroid plexus.
5/18
5/18

Have seen residents mistake this periventricular gray matter for abnormal GM heterotopia when prominent. Nope—this is normal caudate tail/ST along roof of the temp horn of lat ventricle-variable in size across patients, some subtle (like this image), some more prominent.
6/18
6/18

ST curves around with the caudate, and then courses anteriorly in the thalamostriate sulcus (groove between the thalamus and caudate). It is intimately associated with the thalamostriate (terminal) vein, which will drain to the int cerebral vein.
7/18
7/18

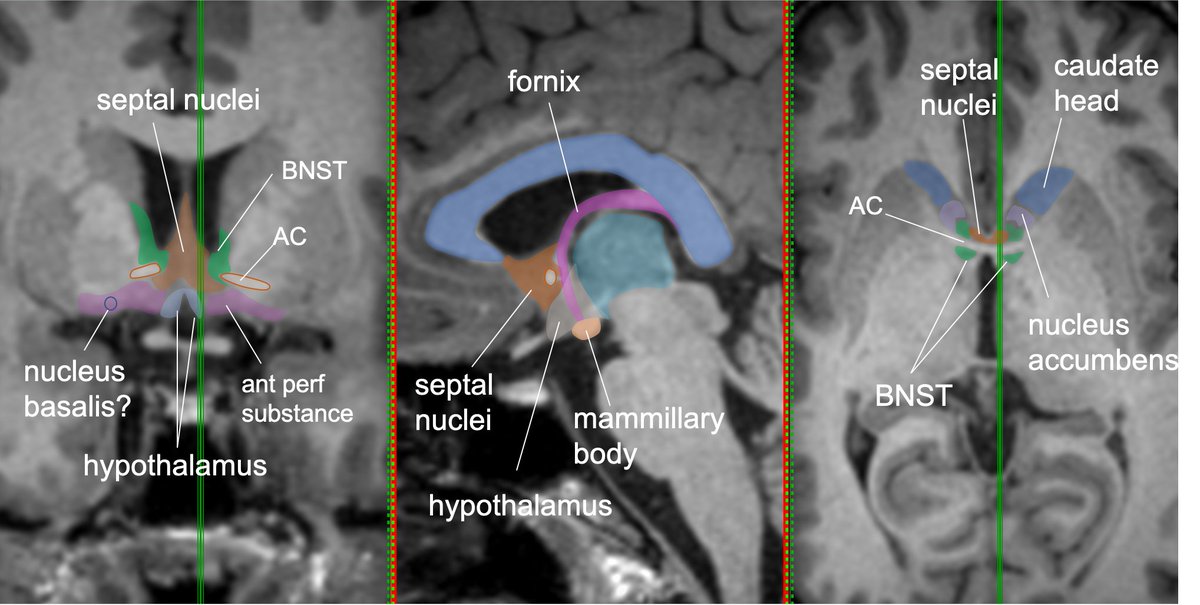
Coursing anterior, the ST appears to enlarge just post to ant commissure—this is the bed nucleus of the stria terminalis (BNST), a functional extension of the amygdala-an integration hub for limbic functions & valence-important in stress response,fear states,social behavior
8/18
8/18

This BNST hub has connections with 3 main pathways: supracommissural, commissural, and subcommisural.
Supracommisural passes above and in front of AC, terminates in septal nuclei and nucleus accumbens (pleasure and reward circuit).
9/18
Supracommisural passes above and in front of AC, terminates in septal nuclei and nucleus accumbens (pleasure and reward circuit).
9/18

Commissural pathway joins AC➡️communications between hemispheres and bilateral amygdalae.
Subcommisural pathway➡️hypothalamus--important connections to hypothalamic-pituitary-adrenal axis (important in emotional/fear response).
10/18
Subcommisural pathway➡️hypothalamus--important connections to hypothalamic-pituitary-adrenal axis (important in emotional/fear response).
10/18

BNST functions have important implications in stress response, addiction, social behaviors, and mood disorders.
11/18
11/18
Note: lots of confusion about structures of basal forebrain ant/inf/about the AC—for good reason! Mixed GM/WM of ant perforated substance, substantia innominata/nuc Basalis, septal nuclei/BNST, nuc accumbens, subcallosal cortex-all in close proximity, similar MR intensity
12/18
12/18
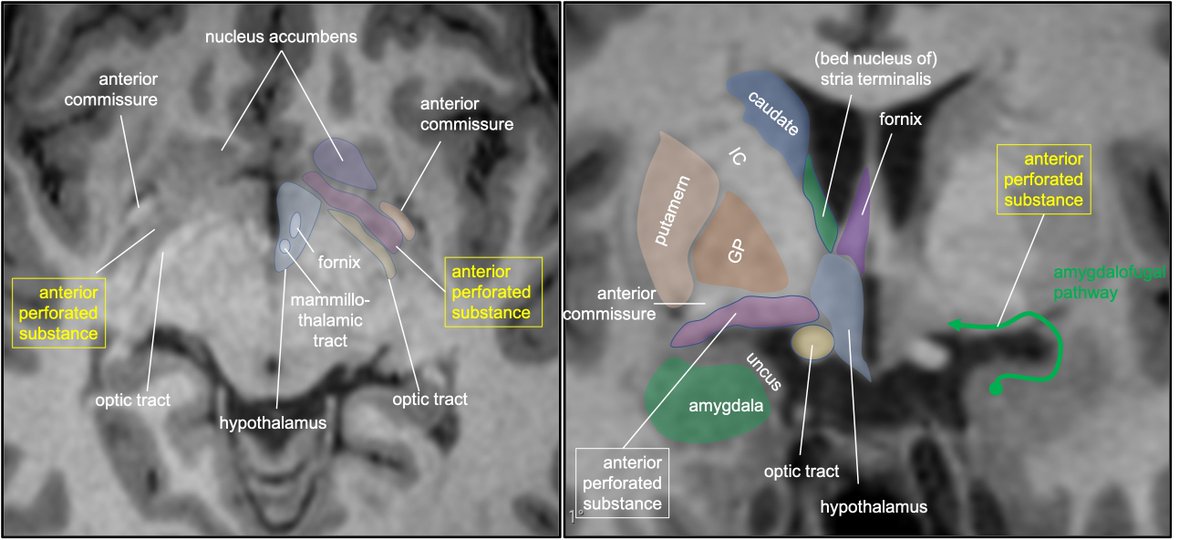
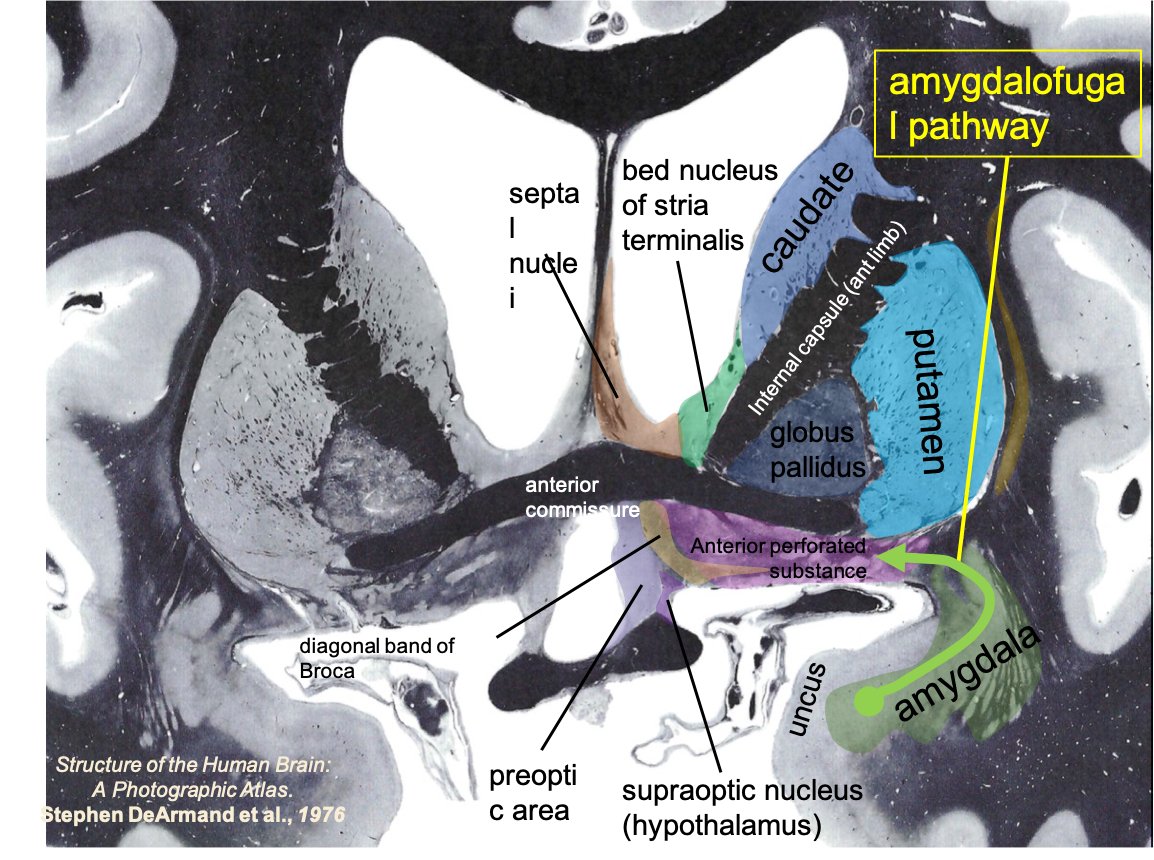
Other pathways from the amygdala (other than ST) include the ventral amygdalofugal (AF) pathway and anterior commissure.
AF path takes more direct route➡️efferents/afferents to septal area, hypothalamus, thalamus, course medially through anterior perforated substance.
13/18
AF path takes more direct route➡️efferents/afferents to septal area, hypothalamus, thalamus, course medially through anterior perforated substance.
13/18

Extensive AF pathway connections to cortex/brainstem are not well defined in humans.
Of note, the amygdaloid networks are intimately tied to olfactory inputs and processing, and the amygdala has been shown to be important in olfactory memory.
14/18
Of note, the amygdaloid networks are intimately tied to olfactory inputs and processing, and the amygdala has been shown to be important in olfactory memory.
14/18
Note on confusing location: The anterior perforated substance is at the basal forebrain ant to the optic tract, and behind the ant commissure & olfactory trigone; it’s continuous with the subcallosal gyrus medially and uncus inferiorly.
15/18
15/18
Main interest in understanding limbic networks for the radiologist is ability to accurately describe location of lesions, whether neoplastic/vascular/demyelinating/etc. May lead to subtle symptoms affecting memory and complex behaviors.
16/18
16/18
I often see lesions of the basal forebrain/septal area and hypothalamus described as “inferior frontal lobe” which does not help the neurologist focus their exam.
17/18
17/18
Relevant path: epileptogenic focus commonly within/involving amygdala in temporal lobe seizures, and likely responsible for the emotional instability, dysphoria, irritability, aggression seen in some of these pts. Tx: medial temporal lobectomy, or laser ablation.
18/18
18/18

• • •
Missing some Tweet in this thread? You can try to
force a refresh