Will vaccination of health care workers (HCWs) lead to accidental silent spreading of COVID-19?
Big possible downside to vaccine allocation recommendations w/out data on whether vaccines reduce infectiousness.
Thread
Big possible downside to vaccine allocation recommendations w/out data on whether vaccines reduce infectiousness.
Thread
The justification for vaccinating HCWs is that they are at high risk of exposure from patients & if infected, removing them from workforce has huge impact on care for patients. So vaccinating them 1st seems like an obvious choice, right? Not w/ available data.
We currently know that 2 vaccines (Pfizer/BioNTech, Moderna) reduce symptomatic infections by ~95%. But we have zero data on whether they reduce infectiousness (& primate studies indicate vaccine didn't eliminate it: nejm.org/doi/pdf/10.105…; biorxiv.org/content/10.110…) 


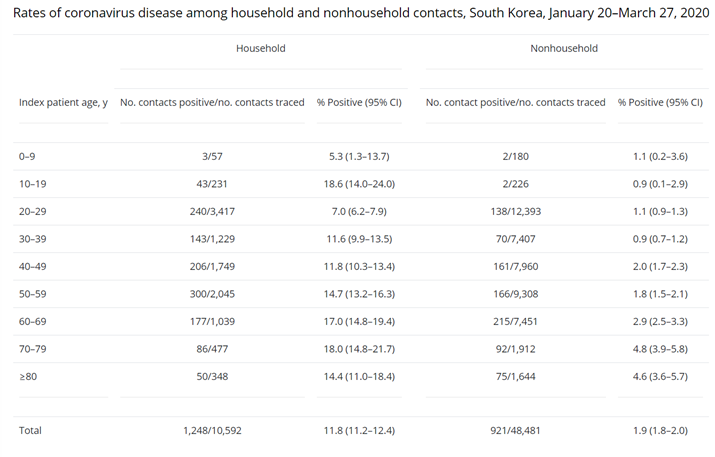
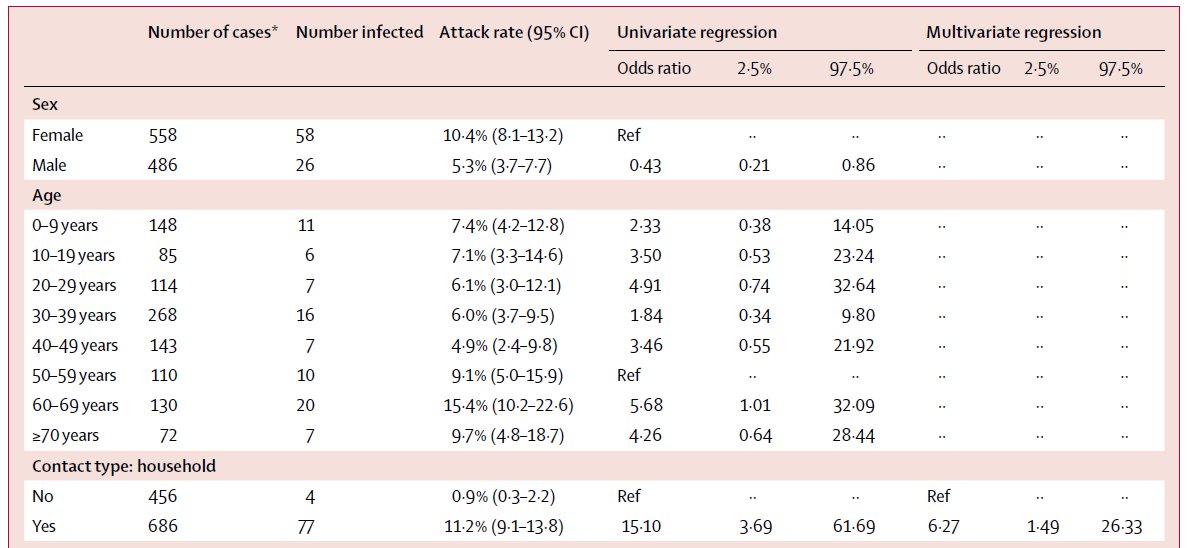
What might happen if we vaccinate HCWs? Vaccination might prevent disease/symptoms but not infection/infectiousness & this could lead to them silently spreading virus to co-workers or non-COVID patients or their families.
Is this worse than what is currently happening? In a few states: No - nurses testing positive for SARS-CoV-2 that are asymptomatic can keep working.
nbcnews.com/news/us-news/n…
nbcnews.com/news/us-news/n…
But in places where this isn't done, vaccination could mask symptoms & lead to infected health care worker infecting others (family, patients, other HCW). Essentially, vaccination could lead to more asymptomatic infections that are transmissible.
What can we do about this?
What can we do about this?
1) Make data on vaccine efficacy on infection & viral loads available to assess importance of this issue. If vaccines greatly reduce viral loads or duration infectious, then issue is minor.
2) Test all vaccinated (& unvaccinated!) health care workers daily to catch infections.
2) Test all vaccinated (& unvaccinated!) health care workers daily to catch infections.
Daily testing of HCW is of no use if results aren't immediately available so need rapid tests & is a substantial ask (~2M people). This is huge issue @michaelmina_lab has been trying to address.
If we don't have tests to prevent silent spreading, then data on infectiousness is critical, especially in HCWs that work in nursing homes.
Clarification: Yes, HCWs are always trying to avoid transmitting the virus to their patients, coworkers & family. But it happens nonetheless.
Infection is often detected by HCWs developing symptoms. If symptoms are masked by vaccination, more chance for asymptomatic spread.
Infection is often detected by HCWs developing symptoms. If symptoms are masked by vaccination, more chance for asymptomatic spread.
Some unfortunate spread by HCWs despite efforts to avoid doing so:
nytimes.com/2020/09/10/us/…
chcf.org/blog/why-nursi…
nytimes.com/2020/09/10/us/…
chcf.org/blog/why-nursi…
• • •
Missing some Tweet in this thread? You can try to
force a refresh