📍WORRISOME—Key things on new 🇬🇧 VUI-202012/01 #SARSCoV2 mutation:
—Likely more infectious, possibly up to 70% faster transmission.
—R0 increase of ~ +0.4
—23 unique changes, many in spike protein.
—Comprises 62% of recent London cases, 43-59% E/SE. 🧵
google.com/amp/s/news.sky…
—Likely more infectious, possibly up to 70% faster transmission.
—R0 increase of ~ +0.4
—23 unique changes, many in spike protein.
—Comprises 62% of recent London cases, 43-59% E/SE. 🧵
google.com/amp/s/news.sky…

2) “Professor Whitty said there was "no current evidence to suggest the new strain causes a higher mortality rate or that it affects vaccines and treatments", but work was under way to confirm this.”
3) @JeremyFarrar, director of the Wellcome Trust, said that its existence was still "worrying and a real cause for concern. Research is ongoing to understand more, but acting urgently now is critical.”
➡️”There is **no part of the UK & globally that should not be concerned**.”
➡️”There is **no part of the UK & globally that should not be concerned**.”
4) More on vaccine escape question—“COVID-19 Genomics UK (COG-UK) consortium said it is difficult to predict whether any given mutation is important when it first emerges, but agreed that biggest concern was any changes that lead to increase in reinfections or vaccine failure.”
5) “But Professor Whitty said that, as of now, there was no evidence to suggest the new strain affected vaccines and treatments— "urgent work" was under way to confirm this & warned that it was "more vital than ever" that people continued to take action to reduce the spread”
6) NOMENCLATURE— The new virus strain name is VUI-202012/01. And one of the strain’s changes is known as N501Y mutation. That N501Y is just one of the changes in this UK variant. Hence you might see the mutation referred to that as well.
7) “This variant first appeared in September and by November it was responsible for 28% of the COVID-19 cases in London. By the week of December 9, more than 62% of London's COVID-19 cases were from this new variant, officials said.” ...
8) “"So what this tells us is that this new variant not only moves fast, its increase in terms of its ability to transmit, but it is becoming the dominant variant. It is beating the others in terms of transmission," Vallance said.”
9) The paper on the new UK strain is now published. It’s very troubling. The virus’s mutations are not just in the spike protein (latches human cells), but many of the mutations are in critical **receptor binding domain** of the spike that latches human cells. And in/near furin.
https://twitter.com/alinouriphd/status/1340505791841841152
10) And mutations in the furin cleavage site of the virus is also critical for processing the virus for virus entry into the cell. Furin has been previously shown to also be critical for human cell entry.
https://twitter.com/alinouriphd/status/1340505795906199552
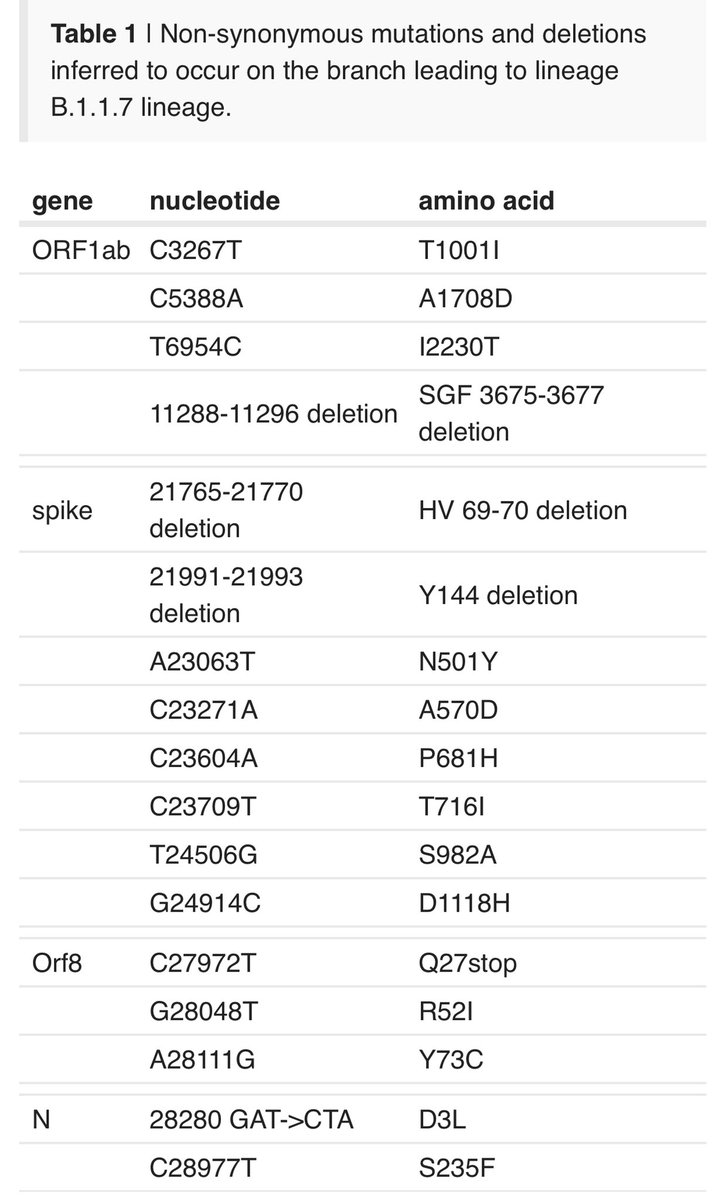
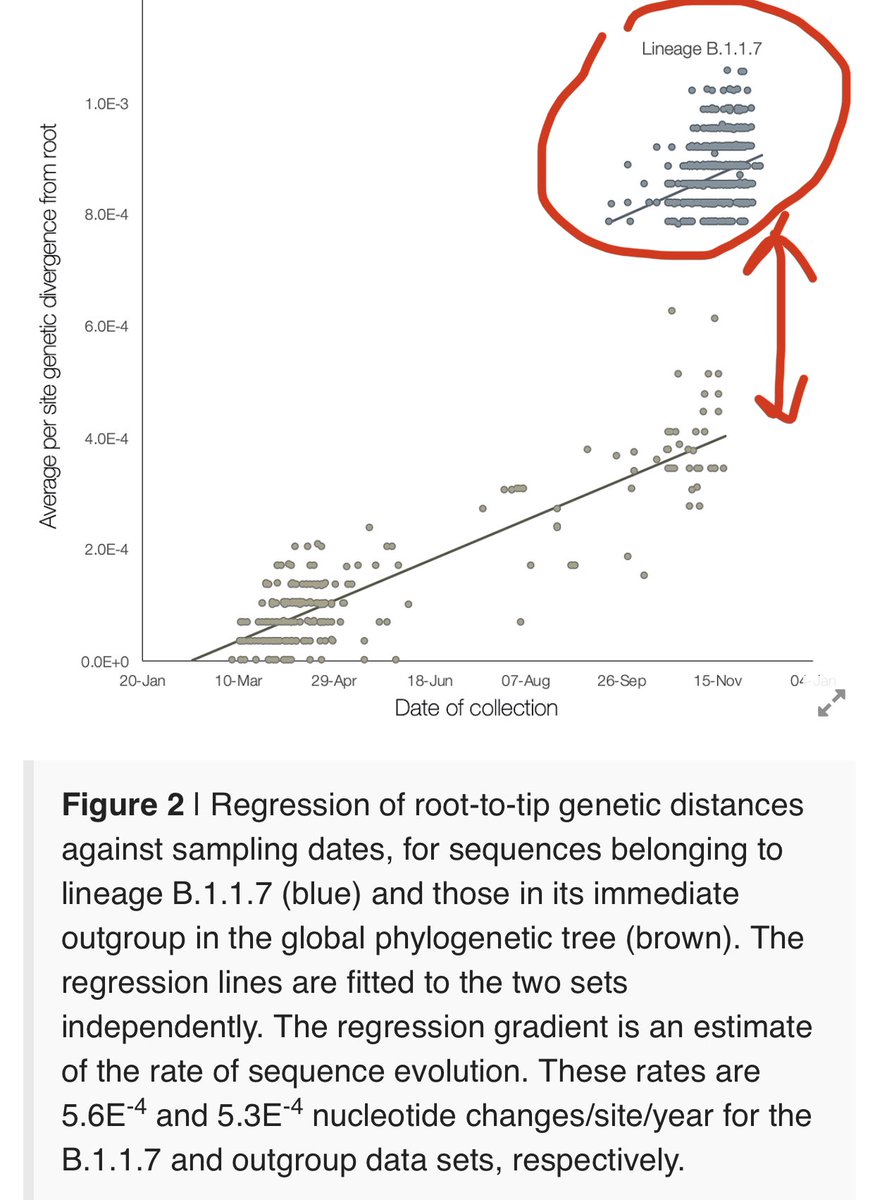
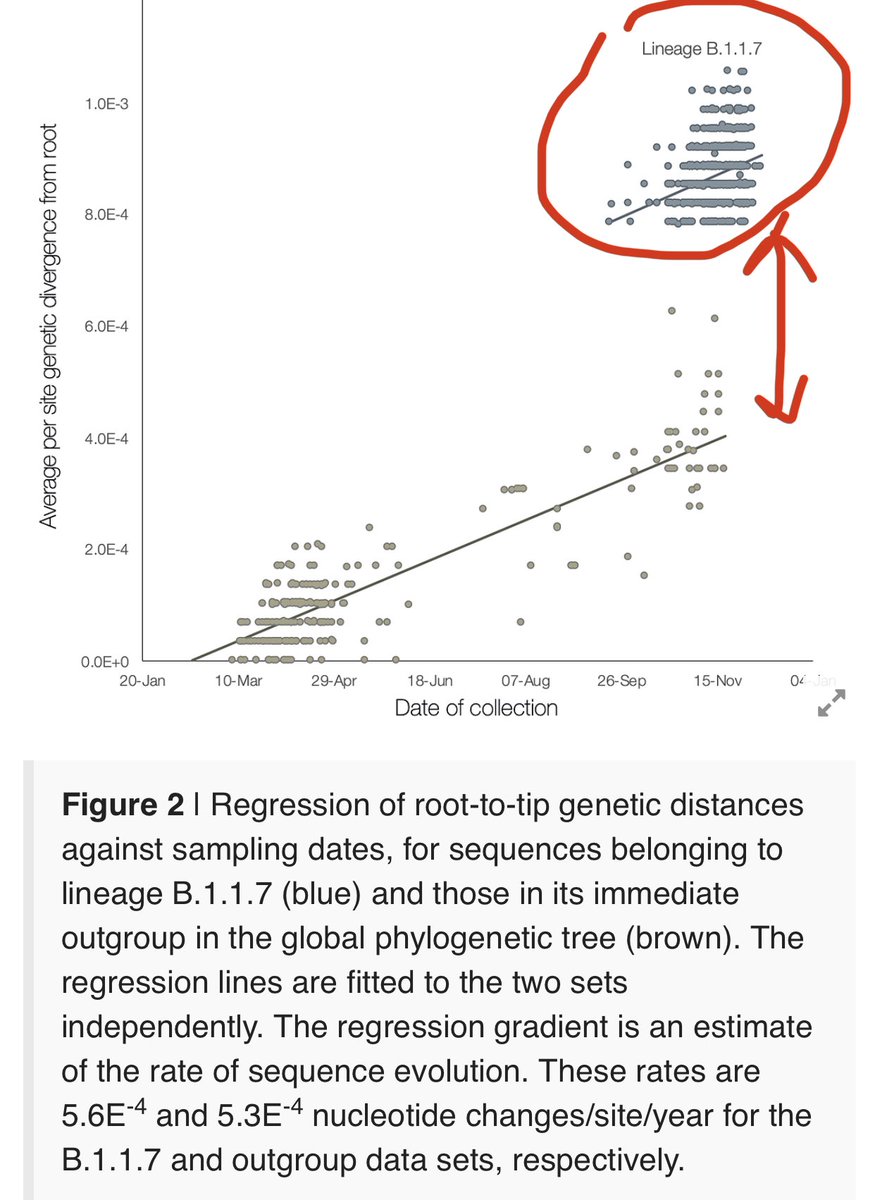
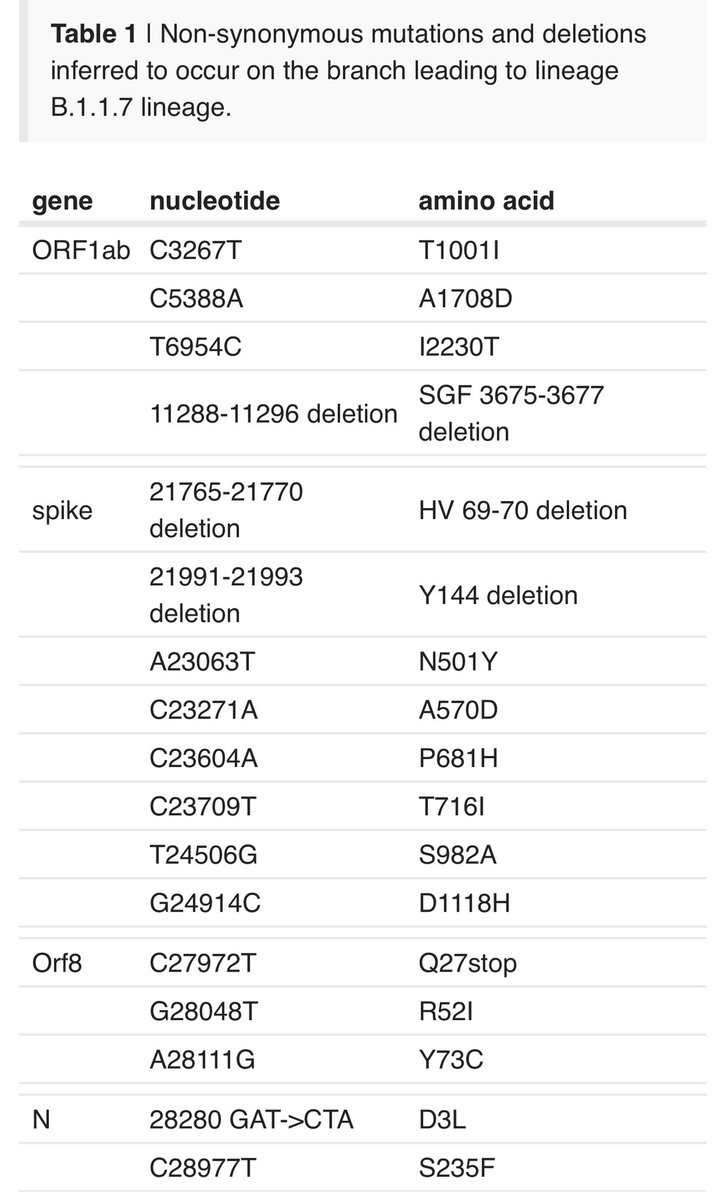
11) The new UK variant’s lineage somehow experienced a sudden jump in mutation number. “lineage B.1.1.7 is more divergent from the phylogenetic root of the pandemic, indicating a *higher rate of molecular evolution on the phylogenetic branch* immediately ancestral to B.1.1.7.”
12) “Further, inferred nucleotide changes on this (new) branch are predominantly amino acid-altering (14 non-synonymous mutations and 3 deletions).”
**AMINO ACID ALTERING** means the mutation changes likely shape of the spike protein, which could mean functional change.
**AMINO ACID ALTERING** means the mutation changes likely shape of the spike protein, which could mean functional change.
13) How could such a sudden increase in mutations happen? Again, it far exceeded the normal rate of accumulated mutations (the global average line).
➡️ likely a chronically infected individual or an immunocompromised individual who couldn’t clear their virus quickly...
➡️ likely a chronically infected individual or an immunocompromised individual who couldn’t clear their virus quickly...
14) “High rates of mutation accumulation over short time periods have been reported previously in studies of immunodeficient or immunosuppressed patients who are chronically infected with SARS-CoV-2”
These infections exhibit detectable SARS-CoV-2 RNA for 2-4 months or longer...
These infections exhibit detectable SARS-CoV-2 RNA for 2-4 months or longer...
15) “Virus genome sequencing of these infections reveals unusually large numbers of nucleotide changes and deletion mutations and often high ratios of non-synonymous to synonymous changes.” (Translation: lot more mutations have yield amino acid changes that could be functional)
16) This is also maybe tied to convalescent plasma.. “Convalescent plasma is often given when patient viral loads are high, and Kemp et al. (2020) report that intra-patient **virus genetic diversity increased after plasma treatment was given**.” 👀
17) Note: this UK 🇬🇧 variant in #SARSCoV2 is different from the South Africa 🇿🇦 variant 501.V2 just announced. That said, both share one of the same mutation in spike: N501Y (N->Y at position 501). However, they seem to have evolved this independently.
https://twitter.com/drericding/status/1340517608643317761?s=21
18) However what the South Africa strain has are 2 other mutations that seem to yield lower virus sensitivity to some antibodies—could mean that previously adapted antibodies may not be as effective against new variant. These 2 mutations were *not* seen in new 🇬🇧 variant though.
19) The “vaccine escape” issue is the #1 most asked question, for good reason. We don’t know yet (scientists are furiously trying to find out via experiments), but vaccine unlikely to be rendered completely ineffective. The current vaccine ‘trains’ you on entire spike protein...
20) ...thus, because you’re trained on the entire spike protein, in terms of antibodies and T cells, you’ll likely still recognize other parts of the spike even if you don’t recognize one part. If your mom has a facial scar on 1 side, you still recognize her from rest of body!
21) But maybe your own facial scar makes your Apple Facial recognition software try more times to recognize you—lower % success rate. Could mean thus lower efficacy.
(Aside—Asian faces recognized by Apple facial software less—i hate it. Bring back home button fingerprint ID!)
(Aside—Asian faces recognized by Apple facial software less—i hate it. Bring back home button fingerprint ID!)
22) But again, the vaccine trains your body to recognize the whole spike protein, not just one spot. Your immune system can still try to recognize other parts of the spike for binding and attack. So you’ll likely be okay. But % efficacy could shift slightly.
23) Back to topic of convalescent plasma therapy... the UK scientists hypothesize it could be a possible read for the rise of the sudden mutations... it’s not that the CP is bad for patients... but it could set up the perfect conditions for genetically steering the virus...
24) “the selection (for new UK variant) arising from antibody therapy may be strong due to high antibody concentrations...” virological.org/t/preliminary-…
25) “Third, if antibody therapy is administered after many weeks of chronic infection, the virus population may be unusually large and genetically diverse at the time that antibody-mediated selective pressure is applied...”
26) ...”creating suitable circumstances for the rapid fixation of multiple virus genetic changes through direct selection and genetic hitchhiking.
These considerations lead us to hypothesise that the unusual genetic divergence of lineage B.1.1.7...”
These considerations lead us to hypothesise that the unusual genetic divergence of lineage B.1.1.7...”
27) “may have resulted, at least in part, from virus evolution with a chronically-infected individual. Although such infections are rare, and onward transmission from them presumably even rarer, they are not improbable given the ongoing large number of new infections.”
28) What about monoclonal antibody drugs? Good question. We don’t know yet. But researchers’ same hypothesis would presumably implicate both antibodies in CP & synthetic antibodies in MAB drugs. It’s a lil akin to antibiotic resistance, but in this case driving virus evolution.
29) BOTTOMLINE: We need more research to confirm. But this virus’s mutation and evolution teaches us we need to stop this pandemic ASAP. Longer it lingers in nature, the greater the chance of unlucky mutations. Take your vaccines now. End this pandemic before it gets worse.
30) Mutations happen all the time, most inert. But the longer we let the pandemic linger in nature, the greater the chance of these mutations emerge. Mink example of human to mink to humans. We need to stop the pandemic and eradicate the virus ASAP. #COVID19
https://twitter.com/drericding/status/1335419078446551041
31) here is a great analogy explanation on the spike protein mutation and what it means for affecting the “key” for entry via the human ACE2 receptor.
https://twitter.com/drkiki/status/1340393570876854272
32) Here is the latest mapping of the new mutations on nextstrain.org. Dr Hodcroft @firefoxx66 is an excellent resource for the latest genetic updates of the mutations.
https://twitter.com/firefoxx66/status/1340359989395861506
33) my favorite vaccine cartoon. Vaccines represent hope. And our children’s future.
https://twitter.com/drericding/status/1340571393700876293
34) Update to the #SARSCoV2 UK mutation thread with the latest info.
https://twitter.com/drericding/status/1340911632147488768
• • •
Missing some Tweet in this thread? You can try to
force a refresh