There are several reasons to think that the new UK #SARSCoV2 variant is an important one as it might be more contagious than other variants, but there are also some uncertainties. So much misinformation is being circulated, so this thread brings key data together. 🧵
1- Genomic data
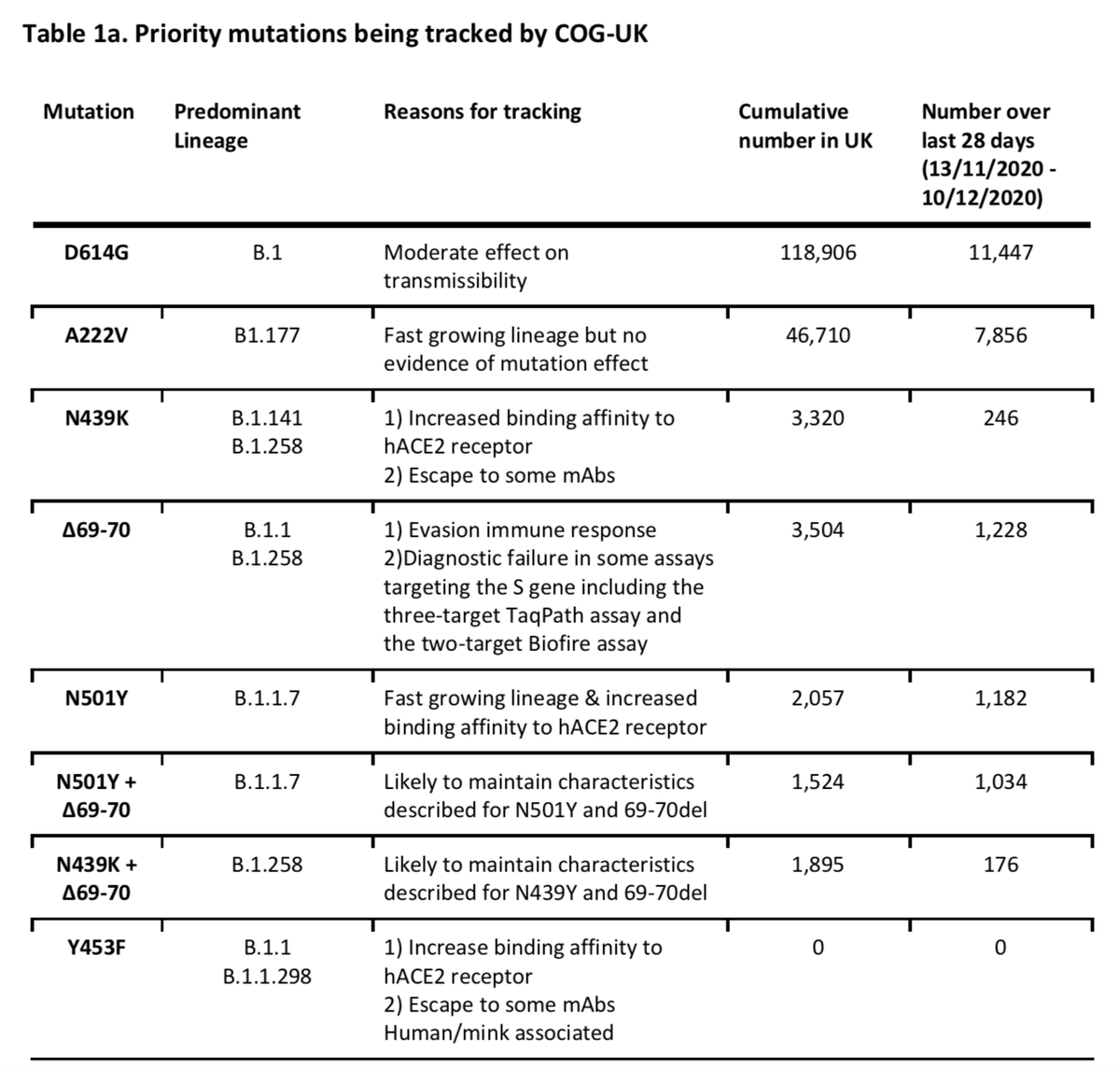
In the UK, COG-UK undertakes sequencing of SARS-CoV-2 samples from ~ 10% of positive cases. This is an enormous effort, and helps scientists to identify mutations and track them over time. Here are some variants being tracked in the UK. 1/ cogconsortium.uk/wp-content/upl…
In the UK, COG-UK undertakes sequencing of SARS-CoV-2 samples from ~ 10% of positive cases. This is an enormous effort, and helps scientists to identify mutations and track them over time. Here are some variants being tracked in the UK. 1/ cogconsortium.uk/wp-content/upl…
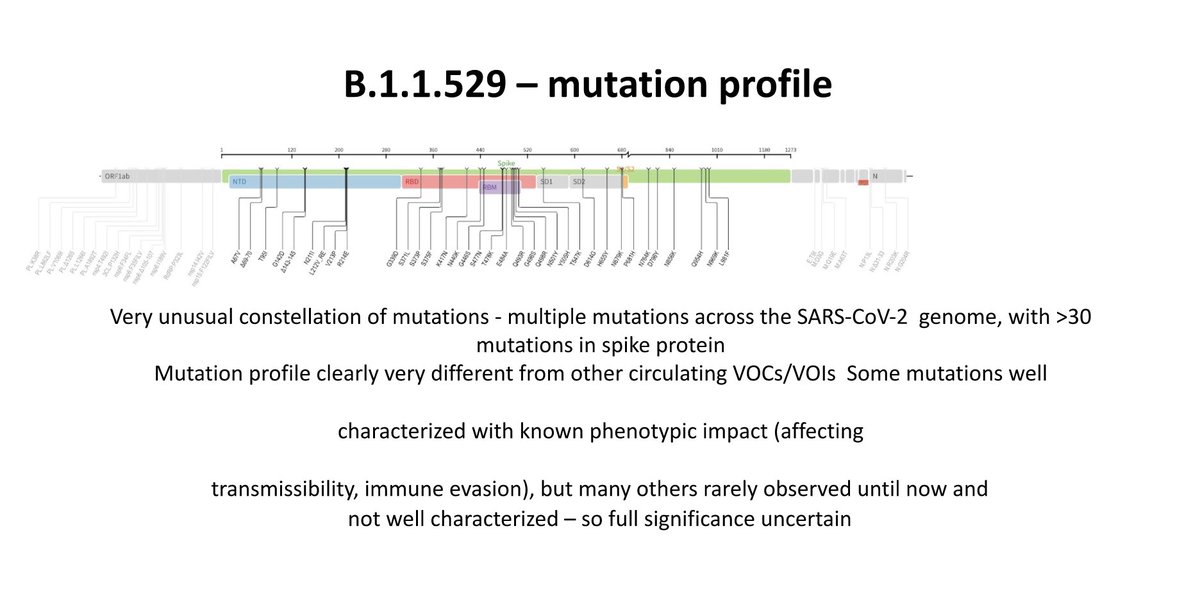
Over time, scientists have identified this new variant, called B.1.1.7 or VUI – 202012/01 (the first Variant Under Investigation in December 2020), which looked different than others. It has acquired 17 mutations compared to its most recent ancestor. 2/ virological.org/t/preliminary-…
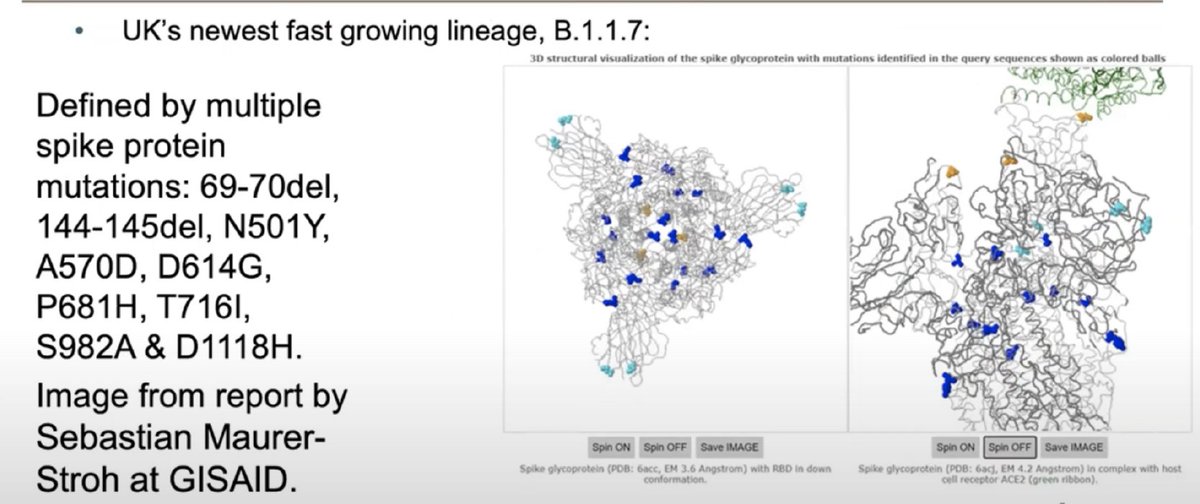
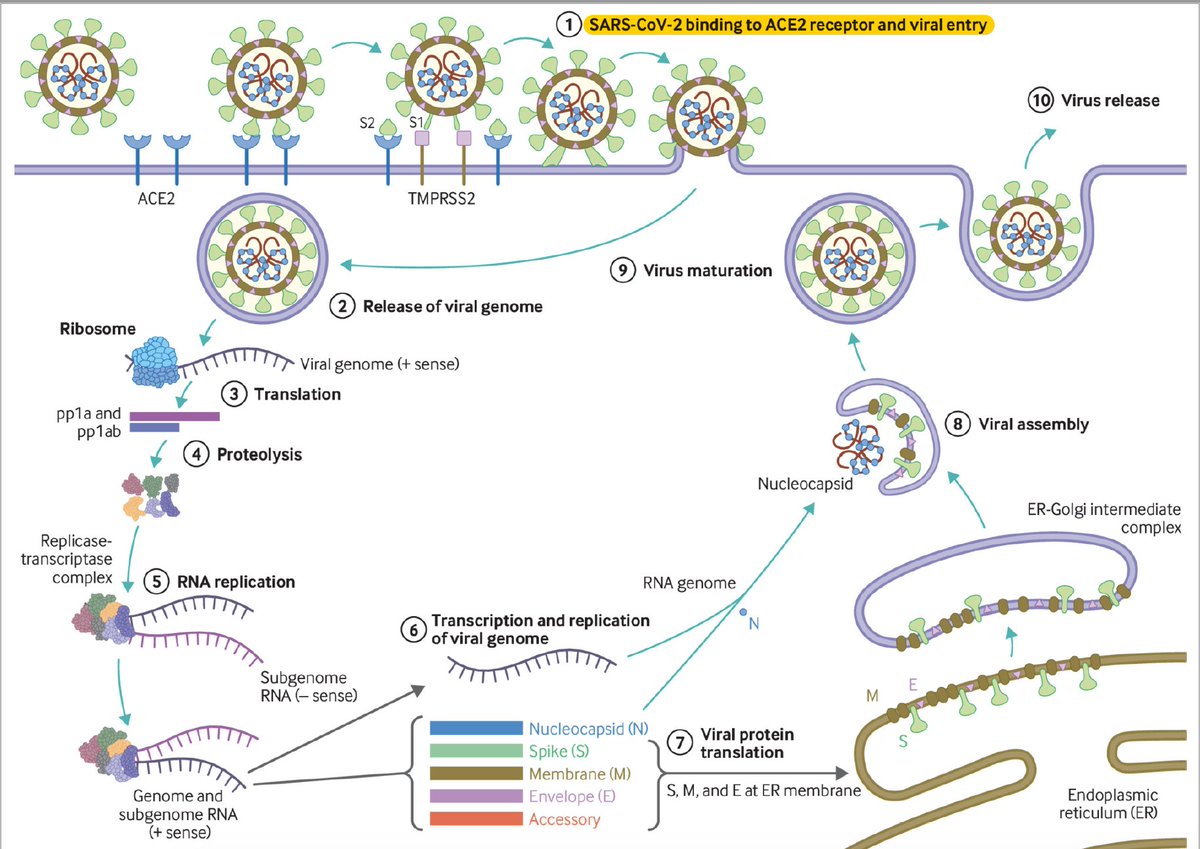
Many of these mutations are on the gene that encodes the spike (S) protein on the surface of SARS-CoV-2, through which the virus binds to and enters human cells, that is the first step in the viral cycle (first step in this diagram) 3/ bmj.com/content/371/bm…
There is experimentally-predicted and plausible biological consequences of some of these mutations seen in this variant but we don't know the combined effect of all these 17 mutations together. Here is a paper detailing this by @arambaut et al. 4/
virological.org/t/preliminary-…
virological.org/t/preliminary-…
2- Epidemiological data
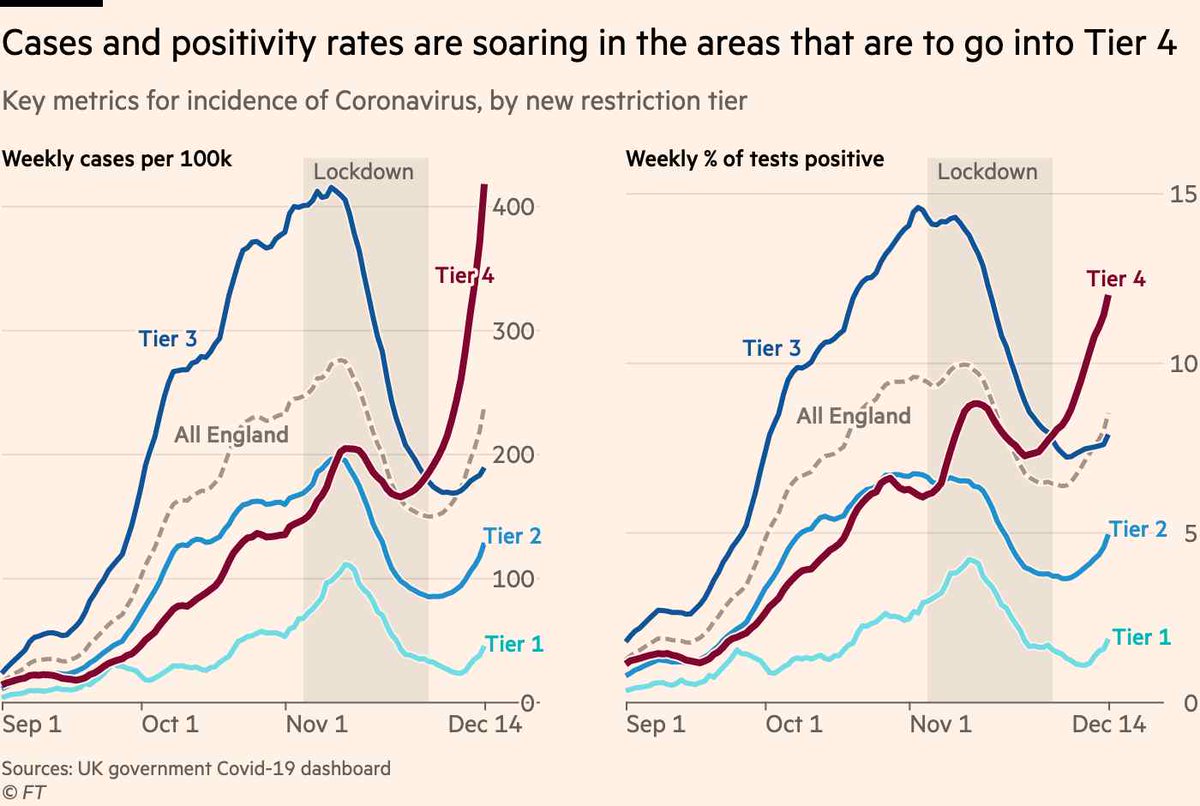
Over the last 3 wks there has been a steep increase in cases in some regions in England, mainly London & East of England & a further increase seen after the end of restrictions in these areas now put into Tier 4. 5/
ft.com/content/538a64…
Over the last 3 wks there has been a steep increase in cases in some regions in England, mainly London & East of England & a further increase seen after the end of restrictions in these areas now put into Tier 4. 5/
ft.com/content/538a64…
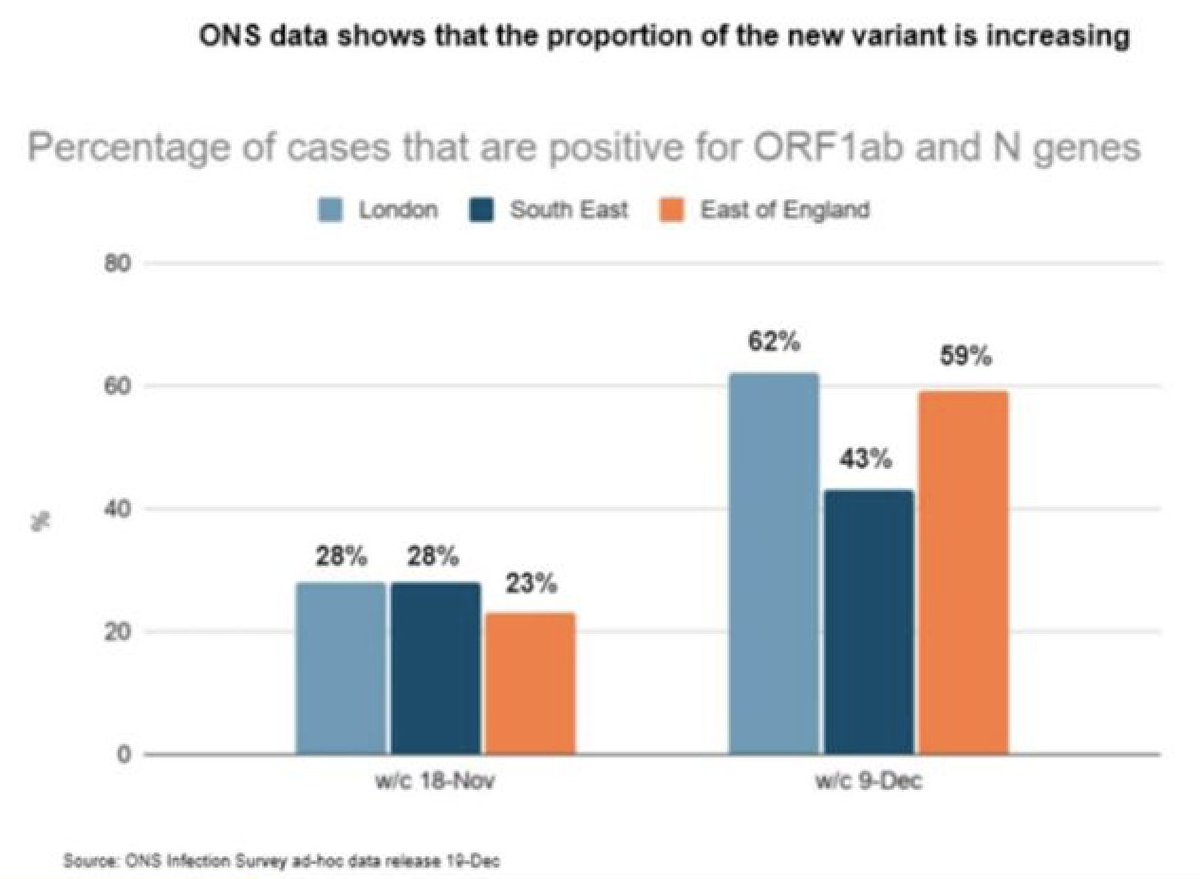
Importantly, the new variant is now dominant in London and the East of England. So, it's rapidly replacing other variants. This figure shows that by w/b of the 9th of December over 60% of all the cases were the new variant compared to 30% in November. 6/
ons.gov.uk/peoplepopulati…
ons.gov.uk/peoplepopulati…
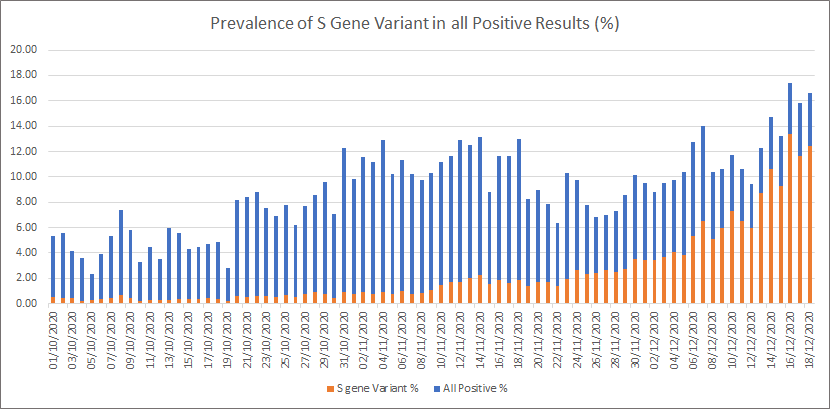
National testing data shows increased prevalence of the variant in positive cases over time. This is detected incidentally by the commonly used 3-gene PCR test because 69-70del leads to a negative signal. But this does not effect the results of the test. 7/
h/t @The_Soup_Dragon
h/t @The_Soup_Dragon
So, putting all these observations together, we can make an assumption that there might be a correlation between the new variant and increased rates of infection. But how can we know whether the increasing frequency reflects the fitness advantage or chance ? 8/
3- Modelling data could help
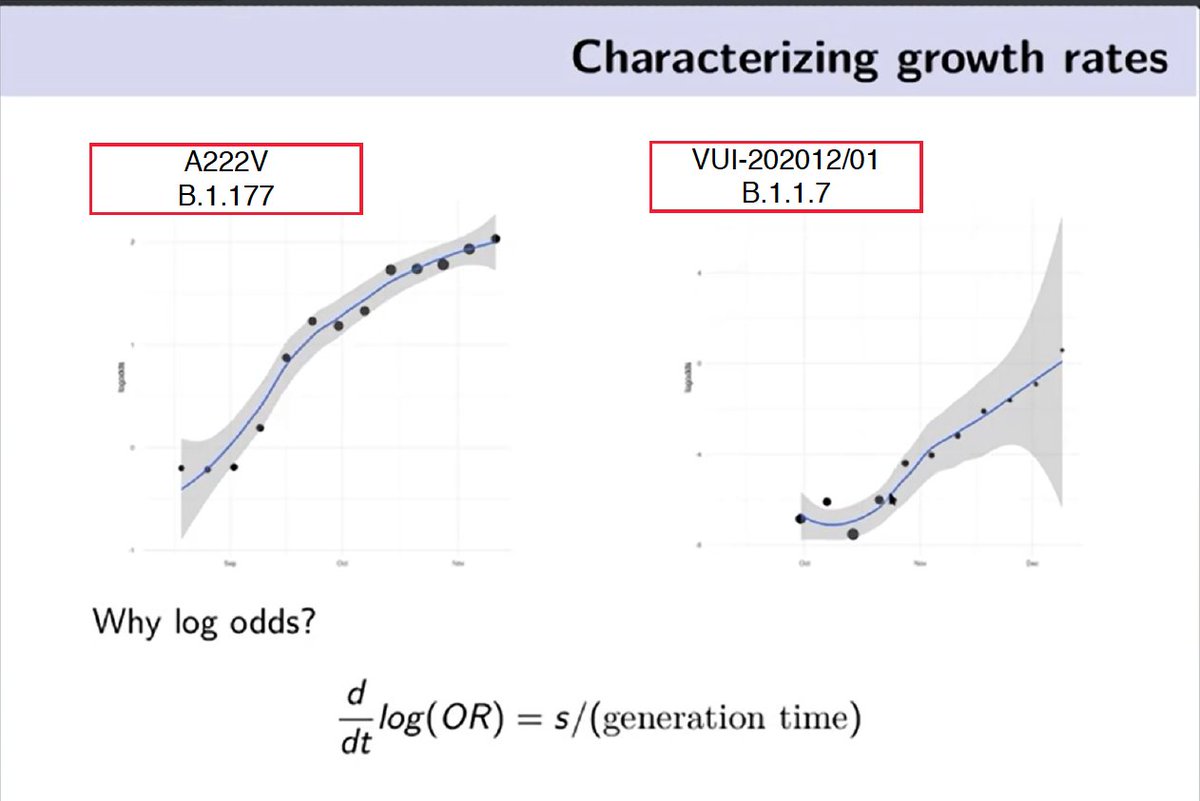
Here you can see growth rates of two different variants based on modelling. A222V (left): rapid rise over summer up to Nov vs. B.1.1.7 (right): the new variant, 1 month data & growth rate seems to be larger. @erikmvolz 9/
Here you can see growth rates of two different variants based on modelling. A222V (left): rapid rise over summer up to Nov vs. B.1.1.7 (right): the new variant, 1 month data & growth rate seems to be larger. @erikmvolz 9/
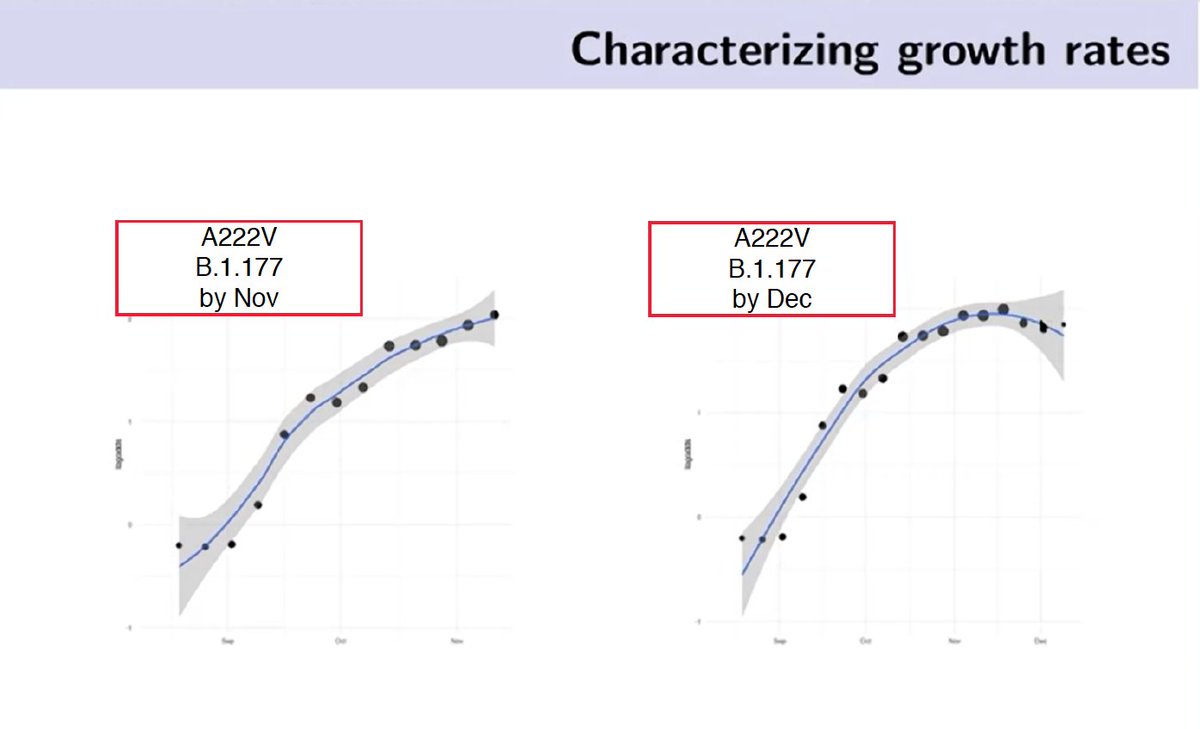
However, the trend observed early on may not pan out later on. For example, A222V showed a steep increase initially over summer but then this increase settled by December. Details in this COG-UK event presented by @erikmvolz
10/
10/
But does it mean the new variant (B.1.1.7) is circulating faster (more transmissible)? In this logistic regression model, comparing the rate of increase of B.1.1.7 vs other variants, B.1.1.7 is estimated to grow faster. Although data is too noisy. 11/
Further modelling studies of correlation between R-values and detection of the variant estimates an increase in the R between 0.39 to 0.93. So, time varying reproduction number is correlated with the increase in fraction of new variant. 12/
khub.net/documents/1359…
khub.net/documents/1359…
4- Virology data
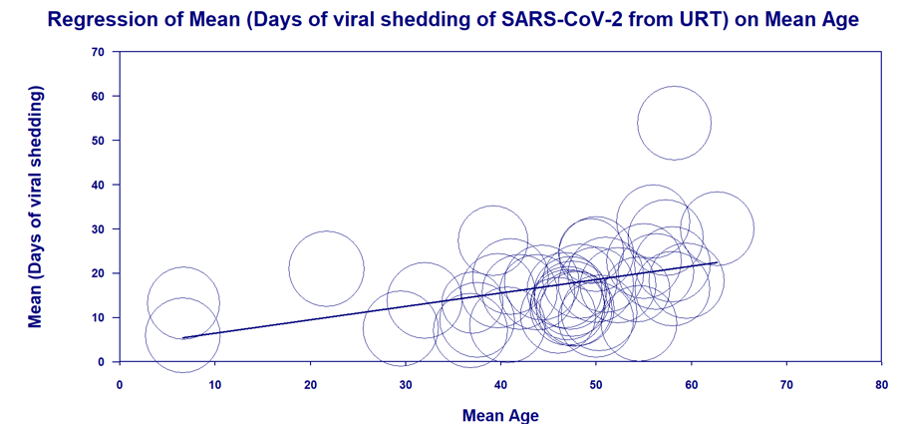
Early virological studies suggest a decrease in Ct value of ~ 2 (higher viral load) associated with the new variant. Viral load inferred from number of unique genome reads suggests increase in viral load (0.5 increase in median log10) in Y501 vs N501. 13/
Early virological studies suggest a decrease in Ct value of ~ 2 (higher viral load) associated with the new variant. Viral load inferred from number of unique genome reads suggests increase in viral load (0.5 increase in median log10) in Y501 vs N501. 13/
In summary: these data suggest that there are lineages with this variant associated with more rapid spread. The concern is that the mutations may be causing this. Although it is possible that this variant may be more transmissible, we don't know how much w/absolute certainty. 14/
Whilst the full significance of the mutations is yet to be determined, the main concern is the rapid rise in infections alongside this distinct variant, which has a previously unseen combination of mutations that are known or likely to have biological effects. 15/
And it's important to note that this variant has also been identified in other European countries. In addition, in South Africa, scientists also identified a lineage separate from the U.K. variant that also has the N501Y mutation. @Tuliodna et al. 16/
krisp.org.za/publications.p…
krisp.org.za/publications.p…
However, there are many unknowns. We don't know if it will influence the severity of illness, reinfection, effectiveness of vaccines and treatments. So, there’s still a lot of work to be done, inclung lab experiments, contact tracing studies & genomic surveillance. 17/
For instance, we don't know how it may influence transmission in kids. If it's more transmissible overall, we would of course expect more transmission across all age groups. However, key unknown is relative effect on transmission among children (if any). 18/
Another worry, of course, is that the virus may mutate to become resistant to the vaccines. But for that to happen, it will likely take years & more mutations - a good discussion by @apoorva_nyc contributions from @firefoxx66 @GuptaR_lab @trvrb & me. 19/ nytimes.com/2020/12/20/hea…
But according to what we already know, it does not alter the effectiveness of social distancing, face masks, hand washing, hand sanitisers and ventilation. Important to continue following these measures. #HandsFaceSpace 20/
https://twitter.com/mugecevik/status/1308080056384843777?s=20
We’ve got to be really careful especially as scientists and doctors because there’s already a lot of speculation and misinformation about this particular variant and getting answers may take a few weeks or months. I will update this thread as more data becomes available 21/
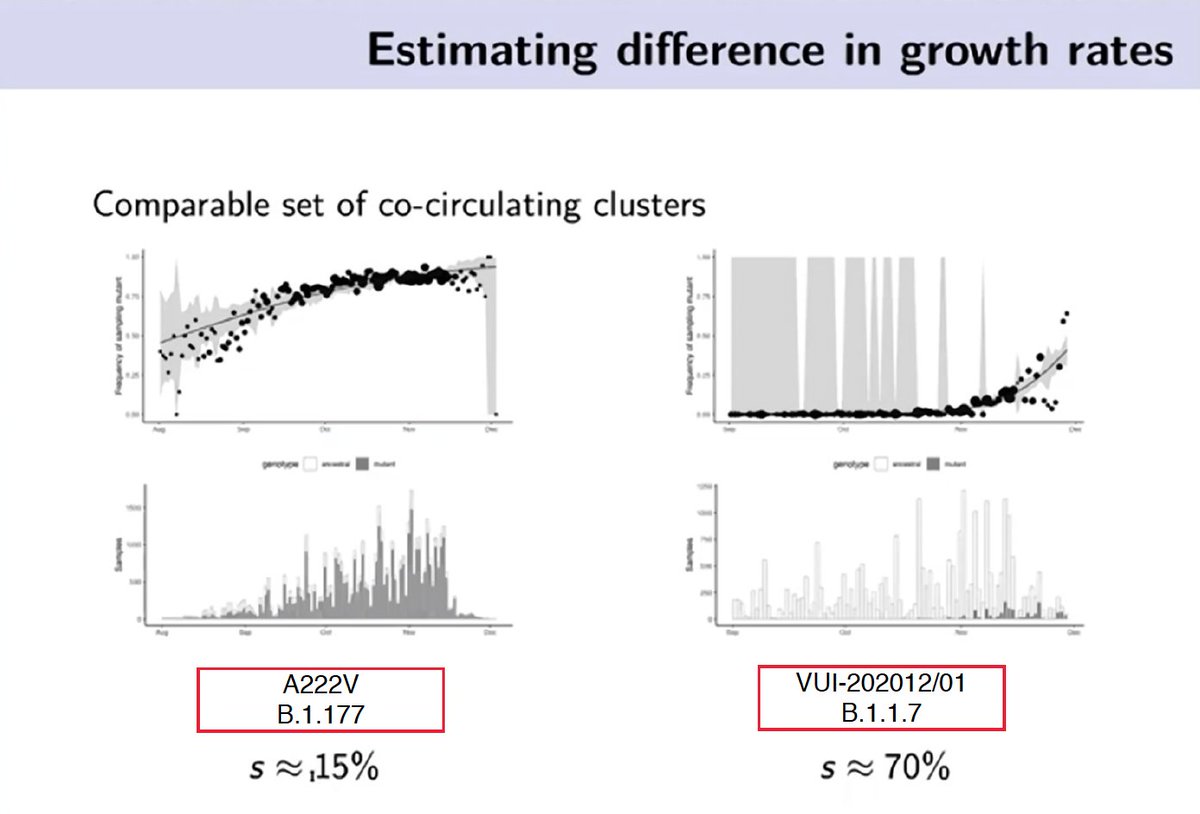
Lots of questions about where that “up to 70% more transmissible” number comes from. It’s in tweet 11#. Important to note this is an early estimate based on logistic growth model. Selection coefficient (S below) is a measure of differences in relative fitness. 22/
https://twitter.com/mugecevik/status/1341094888792858625
New epidemiological data published by the PHE.
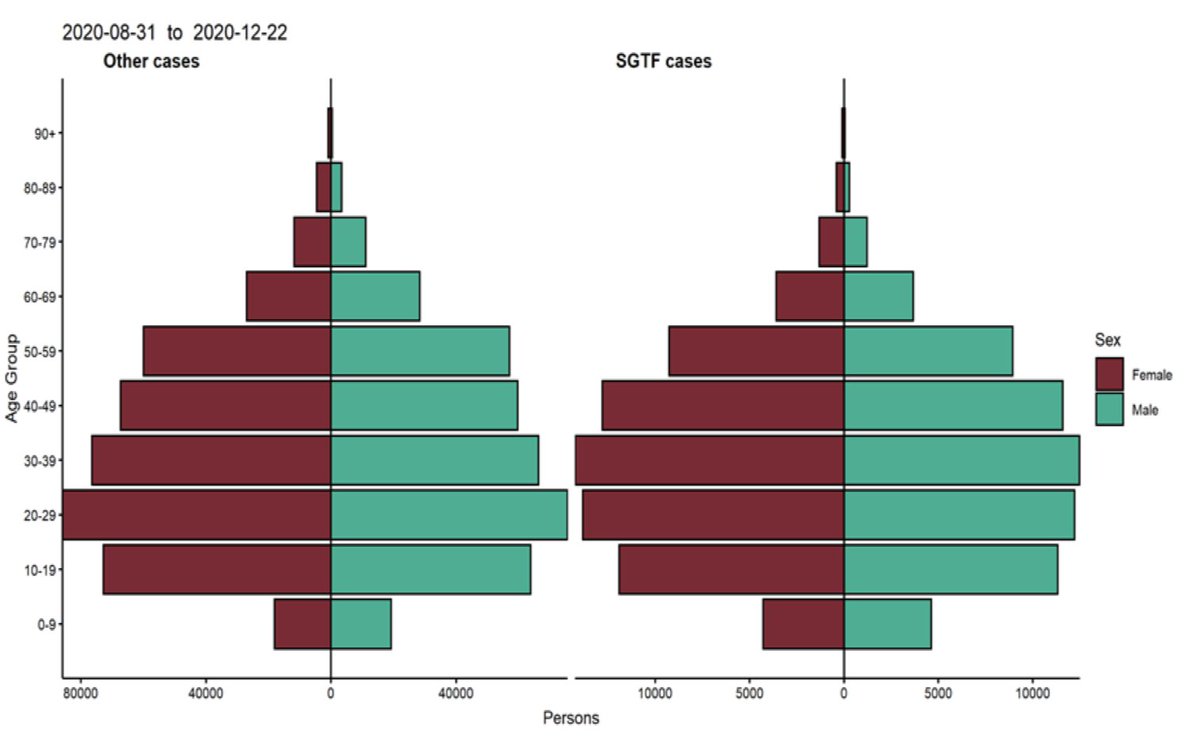
Looking at age-sex distribution of cases from 31/08 to 22/12 (based on S-drop out - SGTF), distribution of cases are similar across age groups for other variants (left) vs. the new variant (right). 23/ gov.uk/government/pub…
Looking at age-sex distribution of cases from 31/08 to 22/12 (based on S-drop out - SGTF), distribution of cases are similar across age groups for other variants (left) vs. the new variant (right). 23/ gov.uk/government/pub…
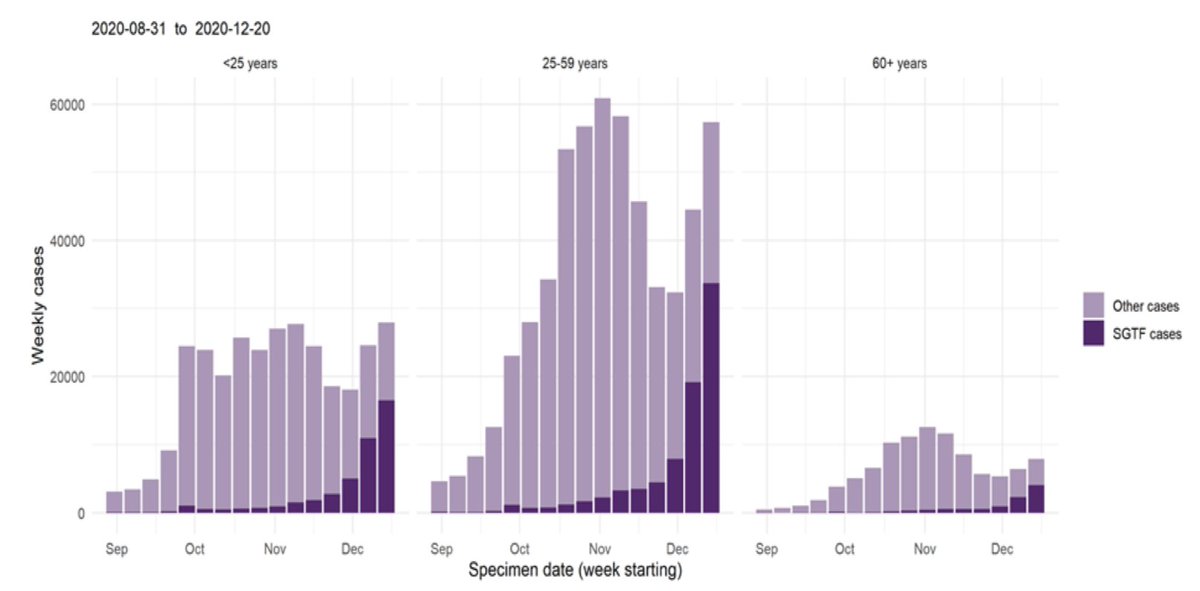
Weekly number of cases by age group and S-drop out (SGTF) shows the distribution of cases w/ other variants vs. B.1.1.7 (new variant). New variant (darker purple bar) is increasing across all ages, sharper increase is seen in the 25-59 age group including total # of cases. 24/
Based on the ONS data (up to 9/12), patterns by age demonstrated no evidence to suggest that B.1.1.7 was more common in certain age groups. There was some variation by age in the whole sample, including London, but this was compatible w/ chance. 25/ (gov.uk/government/col…\)
In a matched-control study, new variant cases were matched to other variants (by age, sex, local authority, specimen date) on a 1:1 (1,769 cases). Majority were living in private house. Interestingly, B.1.1.7 cases were more likely to be part of a residential cluster. 26/
In the same study, 42 (out of 3,538) had a record of hospital admission. Out of this, 16 (0.9%) new variant cases were admitted to hospital compared to 26 (1.5%) other cases. So, no significant difference was seen in hospitalisations (p=0.162). (limited # of observations.) 27/
In the same study, 28-day case fatality rate analysis was restricted to 2,700 cases. 12 of 1,340 (0.89%) variant cases died within 28 days compared with 10 of 1,360 (0.73%) comparator cases. No significant difference was seen in mortality rates (Odds ratio:1.21, p=0.65). 28/
Summary: Based on this preliminary matched-control study, B.1.1.7 does not seem to be associated w/ more hospitalisations or increased 28-d mortality. However, important to note that overall increase in cases in the population could lead to increased hospitalisations. 29/
What about the secondary attack rates (SAR) - the likelihood of infection occurring among susceptible contacts? Based on TTI data, higher SAR was observed for B.1.1.7. Attack rate was 15.1% among those whose index case was confirmed to have B.1.1.7 vs. 9.8% for other variants 30/
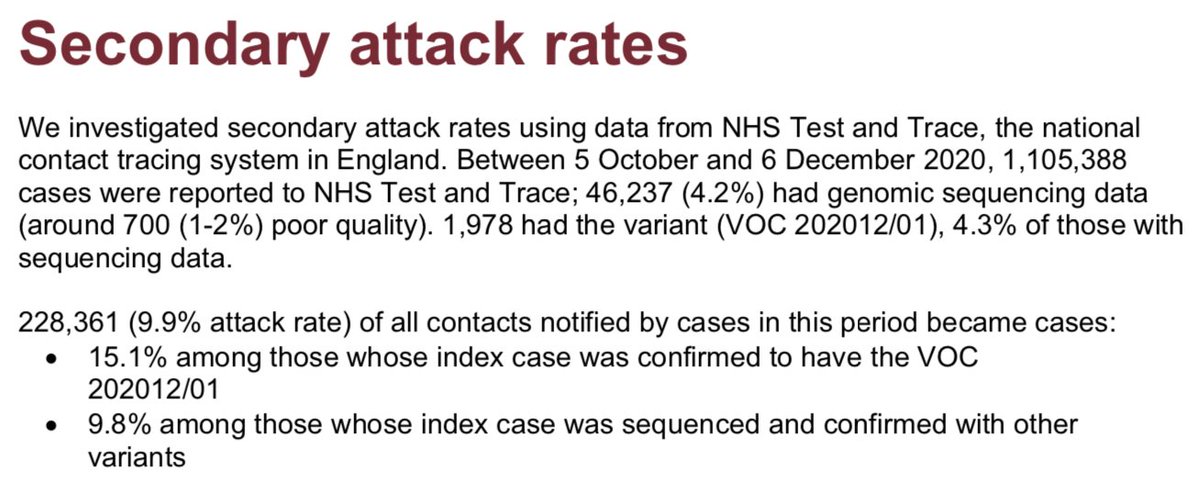
Caveats: While this preliminary data is very useful, it is presented descriptively w/o comparative analysis and confidence intervals, and sampling for sequencing is not random. Further analysis is needed as SAR is influenced by epidemic & population dynamics and clustering. 31/
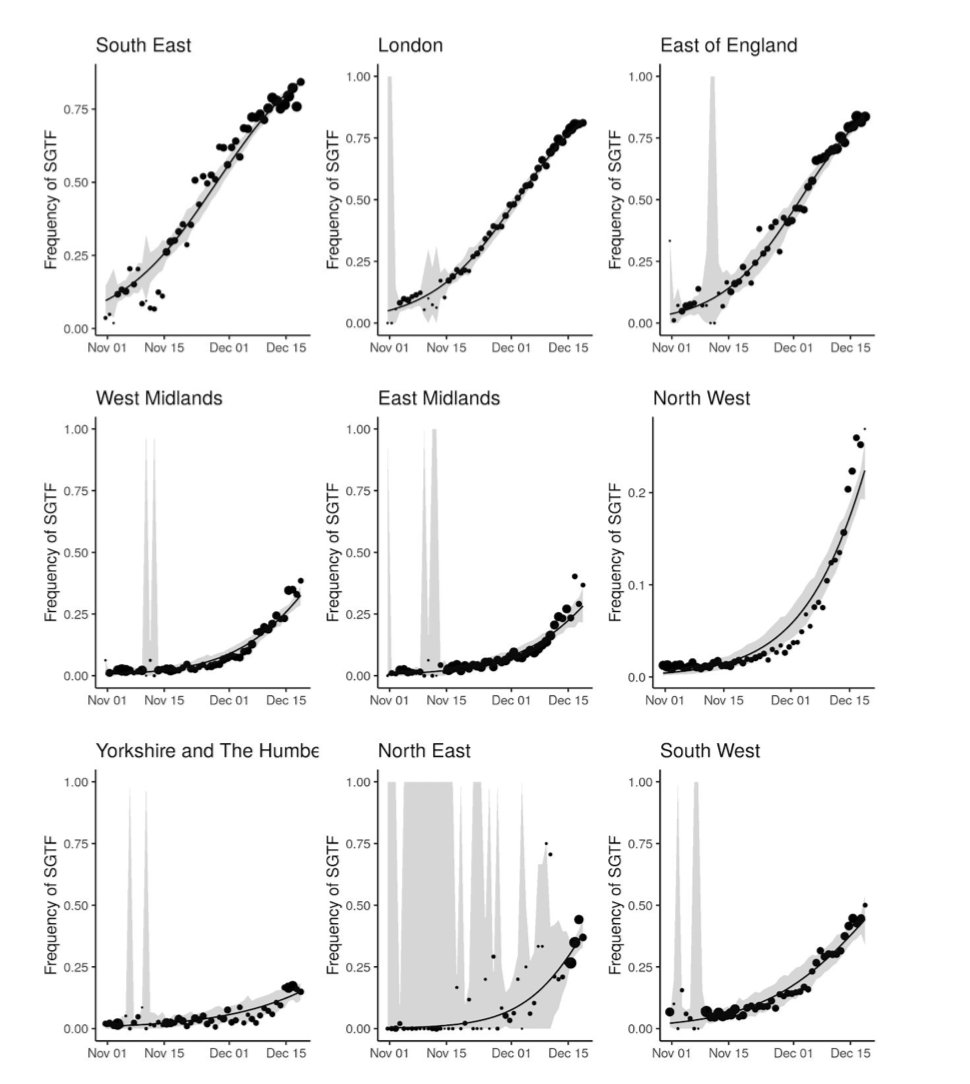
B1.1.7 variant report from Imperial (early results of this analysis was already published in Nervtag minutes 18/12 - tweets #9-12 in this thread). This figure shows new variant is rapidly growing in all regions, estimated increase by 0.4 to 0.7. 32/
(imperial.ac.uk/mrc-global-inf…\)
(imperial.ac.uk/mrc-global-inf…\)
Here is the most misinterpreted result. This analysis is based on S drop out and shows age distribution of cases *only in Nov*. Cases are low in <10, graph (right) shows age share of the variant is higher in <20. Does this mean variant is circulating more in kids? Not really..33/
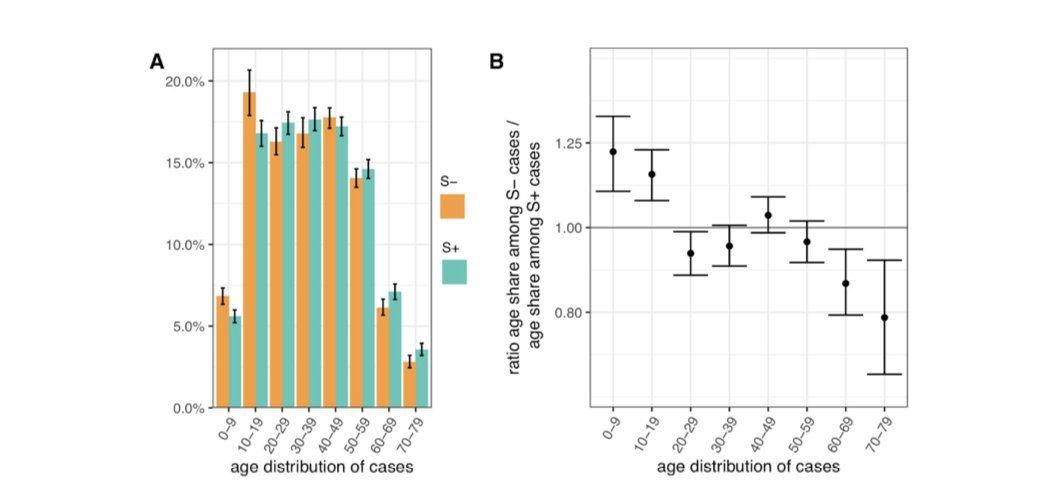
Ratio age share is higher in <20 yo in Nov because as the authors have noted this is due to this variant circulating during a time where lockdown was in force but schools were open. So, this was a transient effect & does not mean variant is circulating more in kids. 34/
And in fact a further analysis by the LSHTM team led by @_nickdavies suggests that over Nov, under 20s were overrepresented in the analysis due to the exact same reason, and as you can see the variant is increasing equally across all age groups. 35/
cmmid.github.io/topics/covid19…
cmmid.github.io/topics/covid19…
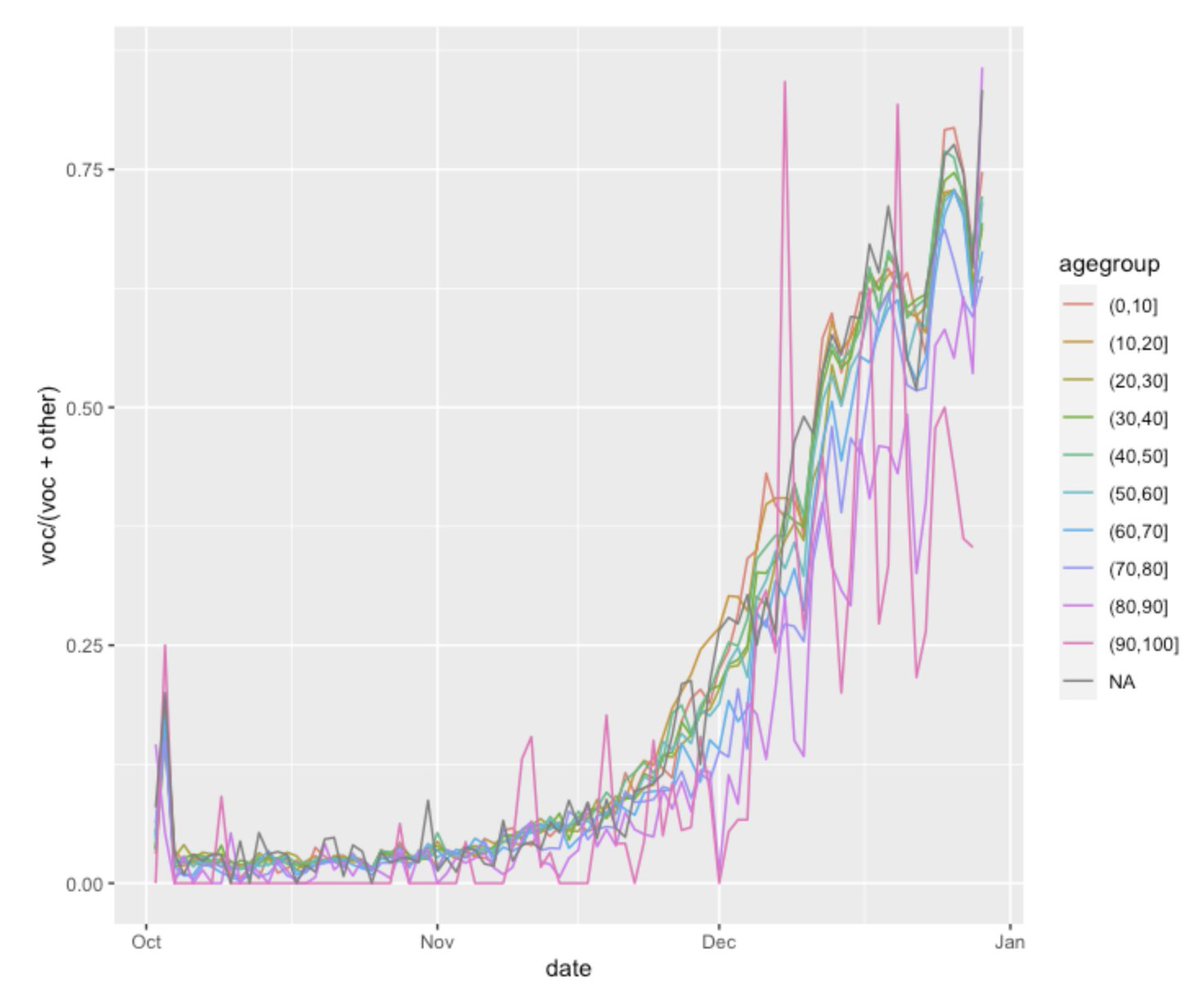
In summary, there are currently 3 analyses (PHE, ONS, LSHTM -tweets #23-25 & 35) that show the new variant has the same age-related transmissibility as other variants. Imperial data showed age share of the variant is higher in kids but this is a transient effect of lockdown. 36/
To clarify: as presented in this thread, evidence suggests that B.1.1.7 is more transmissible overall, which means more transmission across all age groups. But there is no evidence so far to suggest that it favors certain age groups more than others. 37/
https://twitter.com/mugecevik/status/1341094894757171208?s=20
We are still learning and need to look at this data as accumulating evidence. There are still many unknowns, but worryingly infections associated w/B.1.1.7 & hospitalisations are rapidly increasing, so we urgently need to limit community transmission. 38/
https://twitter.com/mugecevik/status/1308080103407132673?s=20
New update about B.1.1.7
Weekly proportion of cases up to Jan 4 with S-drop out (dark purple) is increasing in all regions and all age groups. Mainly concentrated in London and East of England, but 50% of cases are now the variant in Midlands, South West & North. 39/
Weekly proportion of cases up to Jan 4 with S-drop out (dark purple) is increasing in all regions and all age groups. Mainly concentrated in London and East of England, but 50% of cases are now the variant in Midlands, South West & North. 39/


As of 4 January 2021, a total of 6,008 cases with this variant (VOC/202012-01 or B.1.1.7) have been identified in England, via routine genomic surveillance. Age breakdown of cases demonstrates no particular accumulation in any age group. 40/ assets.publishing.service.gov.uk/government/upl…

Contact tracing data looking at the secondary attack rates from index cases with the new variant (B.1.1.7) vs other variants based on genomic data shows higher attack rates with B.1.1.7 in all regions except East Midlands (which has small number of people with genomic data). 41/

Higher secondary attack rates w/ B.1.1.7 are seen across all age groups, but age-related transmissibility looks similar to old variants; i.e. lower SAR in children than adults. So, there is no evidence that this new variant spreads preferentially more efficiently in children. 42/

Similar results are seen based on PCR data with S-drop out. Estimated attack rates are higher in cases with SGTF than cases without SGTF for most regions and age groups, which is proportionate to age related transmissibility. Lower SAR observed in children than adults. 43/
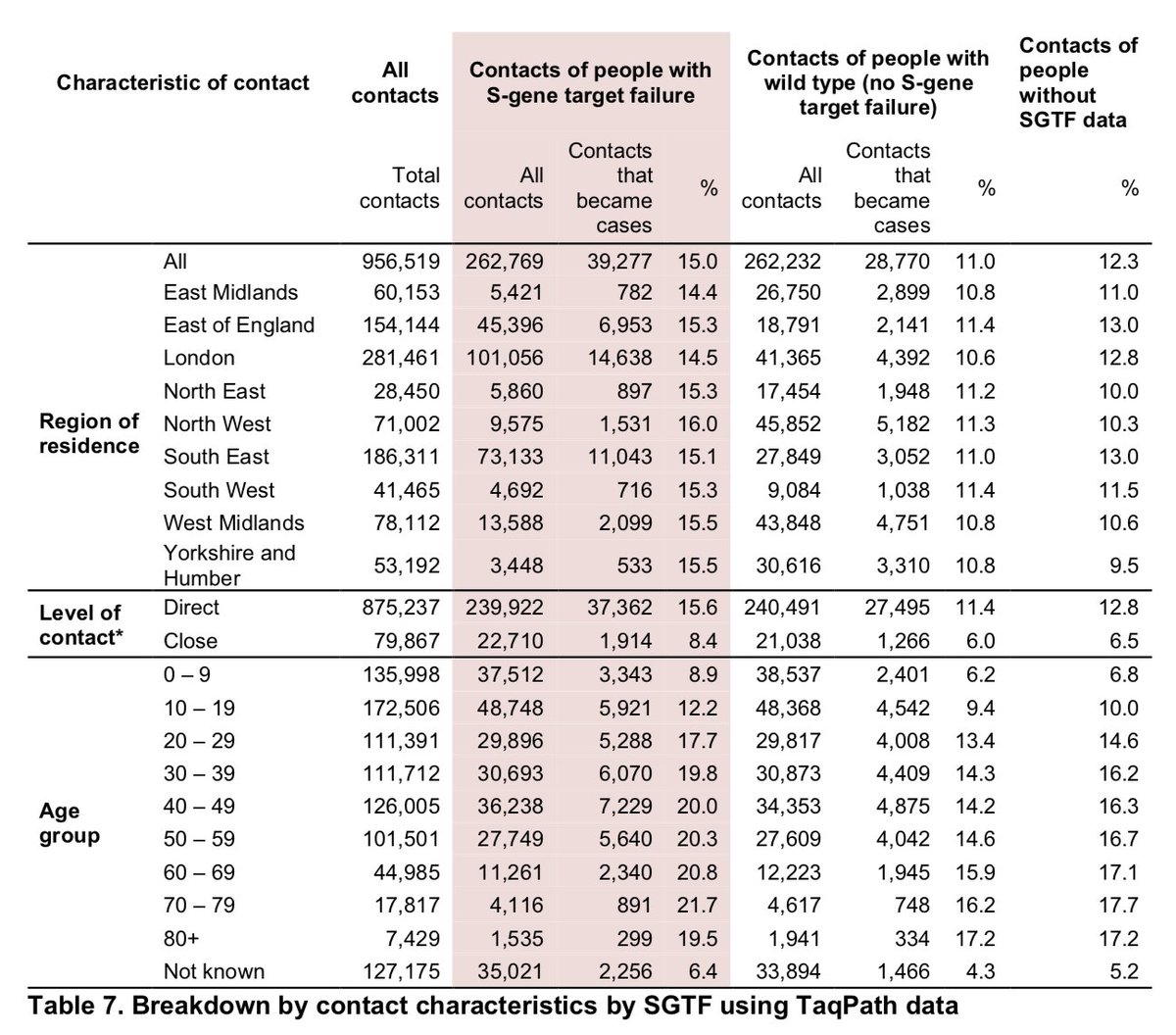
Summary: based on contact tracing data, B.1.1.7 is approx 1.5x transmissible, consistent across different regions. Based on multiple analysis, there is now expert consensus that there is no evidence to suggest it spreads particularly more in children 44/(assets.publishing.service.gov.uk/government/upl…\)
• • •
Missing some Tweet in this thread? You can try to
force a refresh