Based on Run The List 📝 Episode 48, here goes nothing with a #tweetorial on lymphadenopathy (LAD)
Thanks to Kushal (@k_vaishnani) for this week's RTL edition!
Thanks to Kushal (@k_vaishnani) for this week's RTL edition!

What’s 🔑 in narrowing down the etiology of lymphadenopathy?
🔸LOCATION of LAD (axillary, supraclavicular, inguinal)
🔸Detailed HISTORY (including exposures, travel, constitutional symptoms)
Below is a helpful list of exposures & associated LAD 👇
🔸LOCATION of LAD (axillary, supraclavicular, inguinal)
🔸Detailed HISTORY (including exposures, travel, constitutional symptoms)
Below is a helpful list of exposures & associated LAD 👇

Physical characteristics of LAD also provide hints:
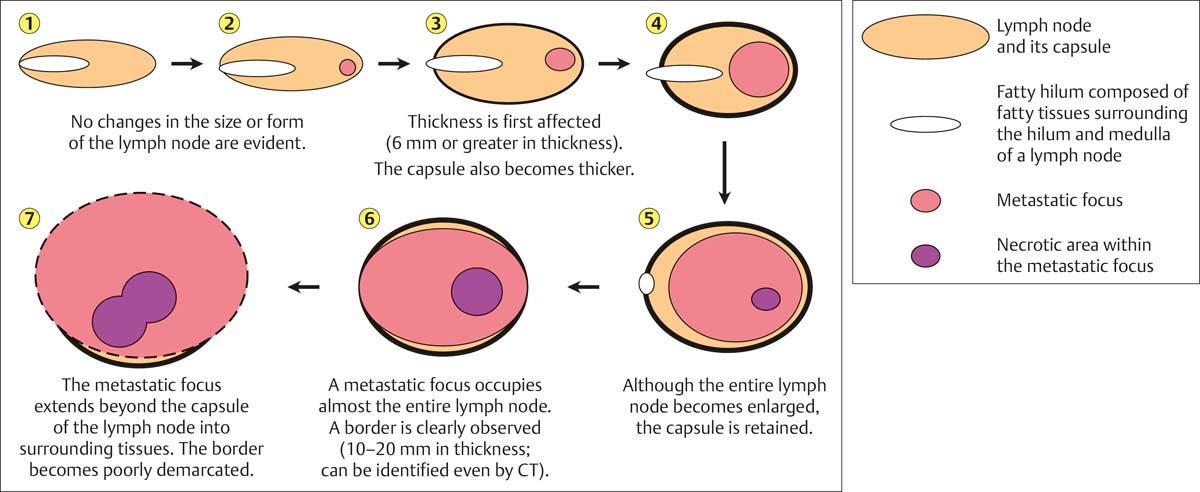
🔹SIZE - greater than size of last phalanx of pinkie is a good rule of 👍; clinically significant!
🔹TENDERNESS - due to inflammatory process, suppuration (pus formation), or hemorrhage into necrotic center of a malignant node
🔹SIZE - greater than size of last phalanx of pinkie is a good rule of 👍; clinically significant!
🔹TENDERNESS - due to inflammatory process, suppuration (pus formation), or hemorrhage into necrotic center of a malignant node
(...cont)
🔹CONSISTENCY
-Stony-hard (cancer 🦀)
-Firm, rubbery nodes (lymphoma)
-“Shotty” (small nodes that feel like buckshot under the skin, in viral illnesses)
🔹MATTED (group of nodes)
-Benign (TB, sarcoidosis, or LGV)
-Malignant (metastatic carcinoma or lymphomas)
🔹CONSISTENCY
-Stony-hard (cancer 🦀)
-Firm, rubbery nodes (lymphoma)
-“Shotty” (small nodes that feel like buckshot under the skin, in viral illnesses)
🔹MATTED (group of nodes)
-Benign (TB, sarcoidosis, or LGV)
-Malignant (metastatic carcinoma or lymphomas)
🔑 points in history taking:
📌 Travel hx (TB endemic areas)
📌 Occupational hx (silicon, beryllium exposure)
📌 Pets (e.g. cats 🐈)
📌 Associated sx (rash, arthralgia, pharyngitis, B-symptoms)
📌 Time course ⏰
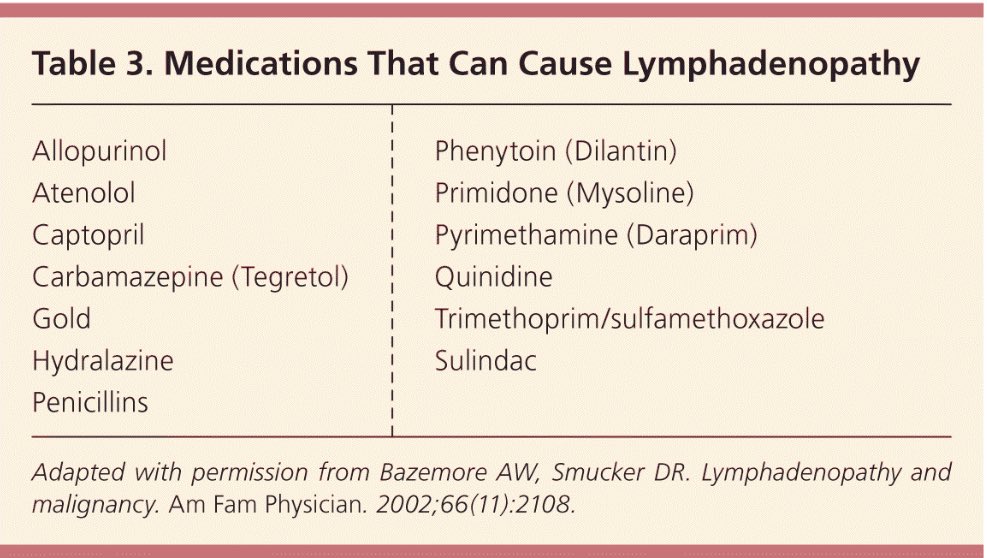
📌 Recent infections, immunizations, & medications (yes, meds too!)
📌 Travel hx (TB endemic areas)
📌 Occupational hx (silicon, beryllium exposure)
📌 Pets (e.g. cats 🐈)
📌 Associated sx (rash, arthralgia, pharyngitis, B-symptoms)
📌 Time course ⏰
📌 Recent infections, immunizations, & medications (yes, meds too!)
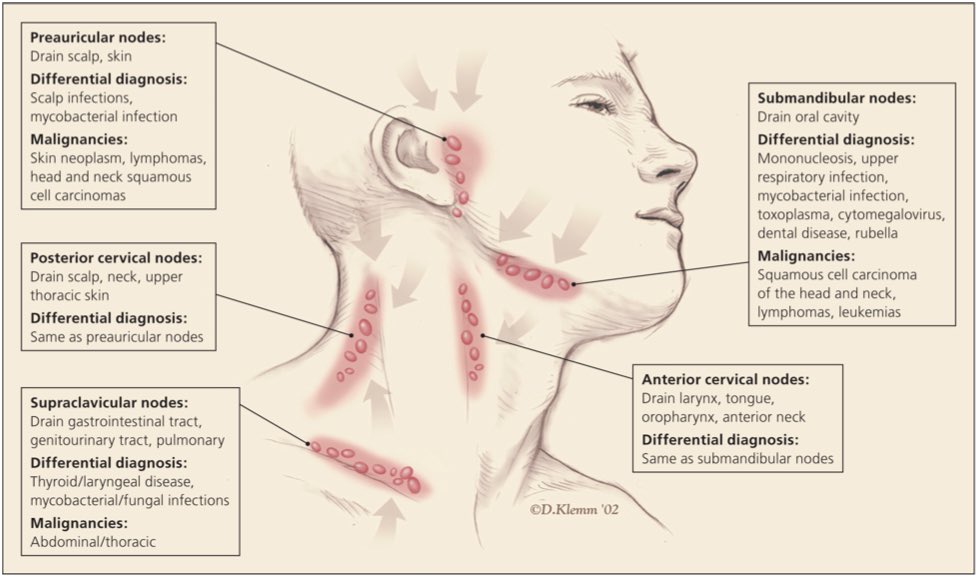
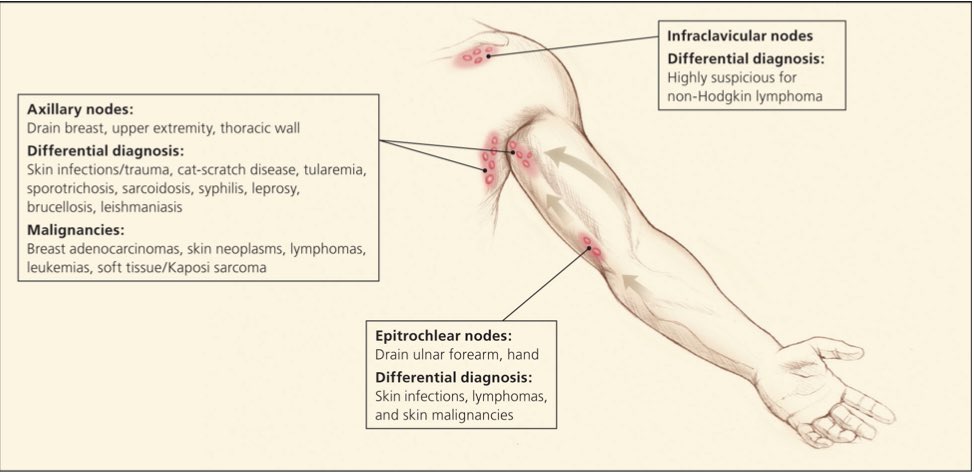
LN location matters 🗺️!
🟡Cervical - EBV, CMV, HIV, Toxo, MTB, squamous cell ca, melanoma
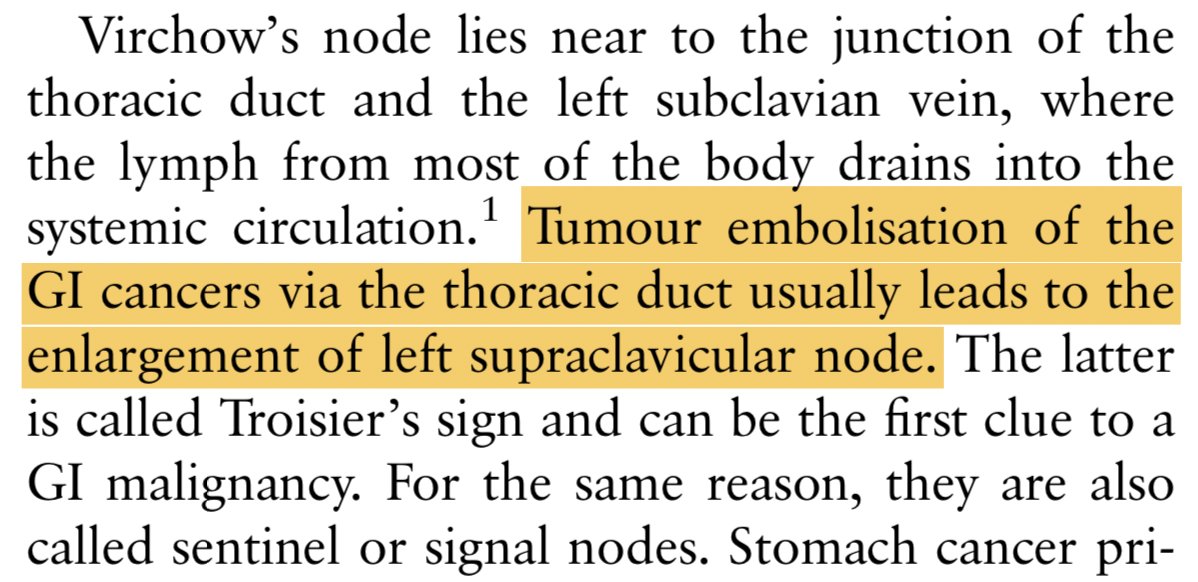
🟠Supraclavicular - highest malignancy risk:
🔵RIGHT supra. - mediastinum, lungs, esophagus
🟢LEFT supra. (Virchow's) - testes, ovaries, kidneys, pancreas, prostate, stomach, gallbladder
🟡Cervical - EBV, CMV, HIV, Toxo, MTB, squamous cell ca, melanoma
🟠Supraclavicular - highest malignancy risk:
🔵RIGHT supra. - mediastinum, lungs, esophagus
🟢LEFT supra. (Virchow's) - testes, ovaries, kidneys, pancreas, prostate, stomach, gallbladder

(...cont)
🔴Paraumbilical (Sister Mary Joseph's node) - abdominal or pelvic neoplasm 🦀
🟣Axillary LAD - breast cancer (often 1st site of breast cancer metastasis 🚨!)
🟤Inguinal - STI 🦠
🔴Paraumbilical (Sister Mary Joseph's node) - abdominal or pelvic neoplasm 🦀
🟣Axillary LAD - breast cancer (often 1st site of breast cancer metastasis 🚨!)
🟤Inguinal - STI 🦠

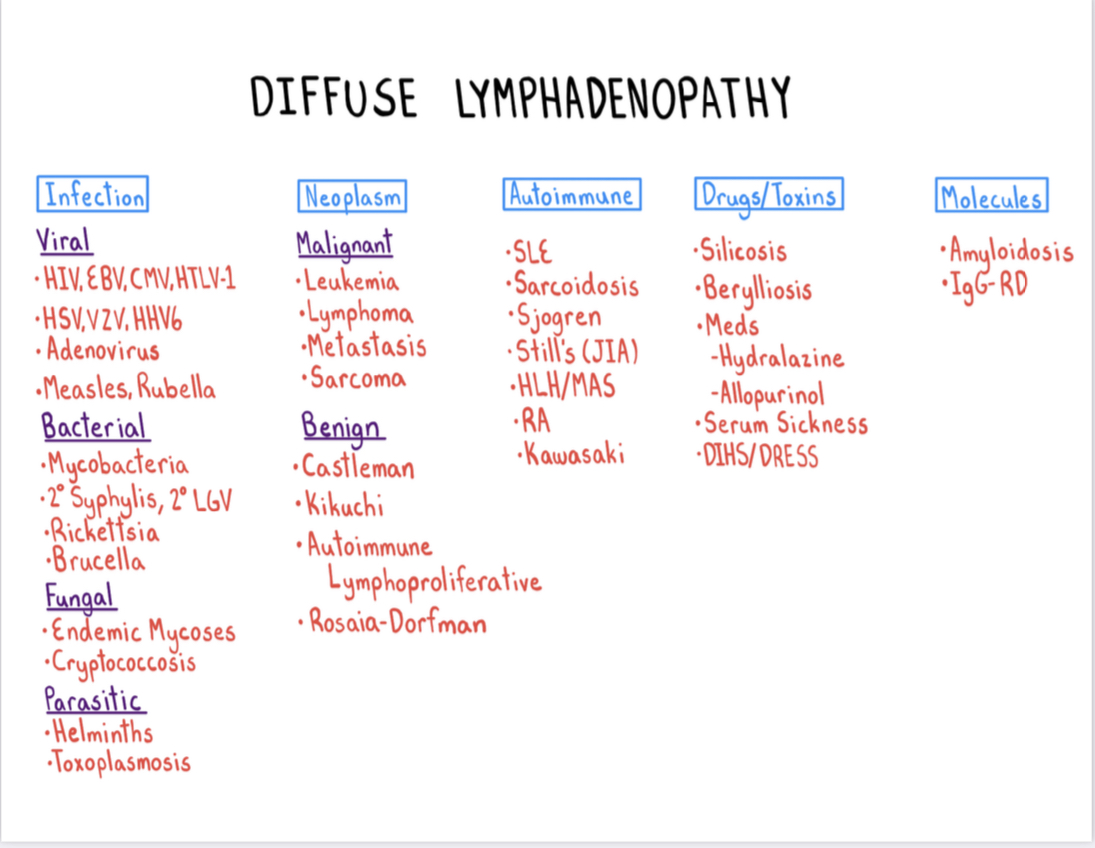
Now let’s go over the CAUSES of LAD 📝
5 main categories (iMADE):
📌Infection
📌Malignancy
📌Autoimmune/rheumatologic
📌Drugs
📌MolEcules (amyloidosis, IgG4-related disease)
Excellent schema from @CPSolvers & their iMADE mnemonic:
5 main categories (iMADE):
📌Infection
📌Malignancy
📌Autoimmune/rheumatologic
📌Drugs
📌MolEcules (amyloidosis, IgG4-related disease)
Excellent schema from @CPSolvers & their iMADE mnemonic:
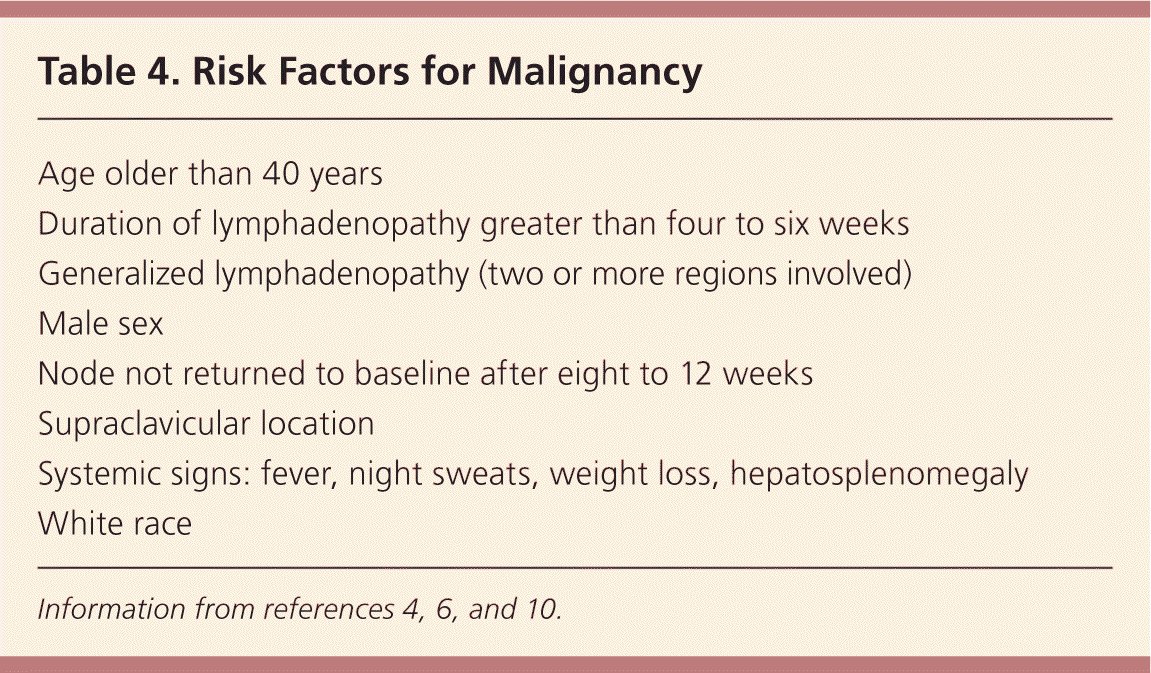
⛳️Red flags⛳️ associated w/ malignancy 🚨:
📌 Age >40 y/o
📌 Male sex, white race
📌 Supraclavicular location of the node(s)
📌 B-symptoms (fever, night sweats, unexplained weight loss)
📌 Age >40 y/o
📌 Male sex, white race
📌 Supraclavicular location of the node(s)
📌 B-symptoms (fever, night sweats, unexplained weight loss)
Now let's cover one of my favorite topics 🏆
🦠Infective lymphadenitis🦠!
DDx can be broken down like this:
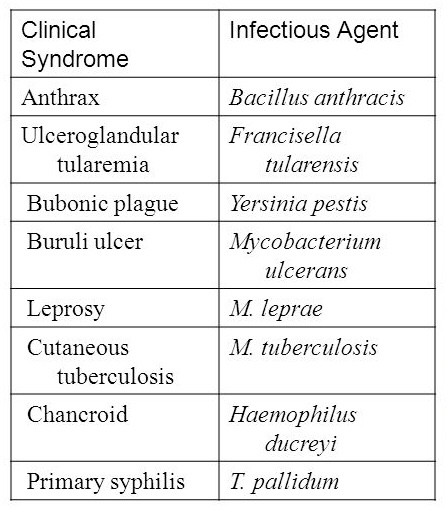
💥Regional LAD
💥Inguinal bubo formation
💥Ulceroglandular syndrome (ulcer+LAD - see table👇)
💥Oculoglandular syndrome (👁️+LAD - see tweet 👇)
💥Generalized LAD
🦠Infective lymphadenitis🦠!
DDx can be broken down like this:
💥Regional LAD
💥Inguinal bubo formation
💥Ulceroglandular syndrome (ulcer+LAD - see table👇)
💥Oculoglandular syndrome (👁️+LAD - see tweet 👇)
💥Generalized LAD
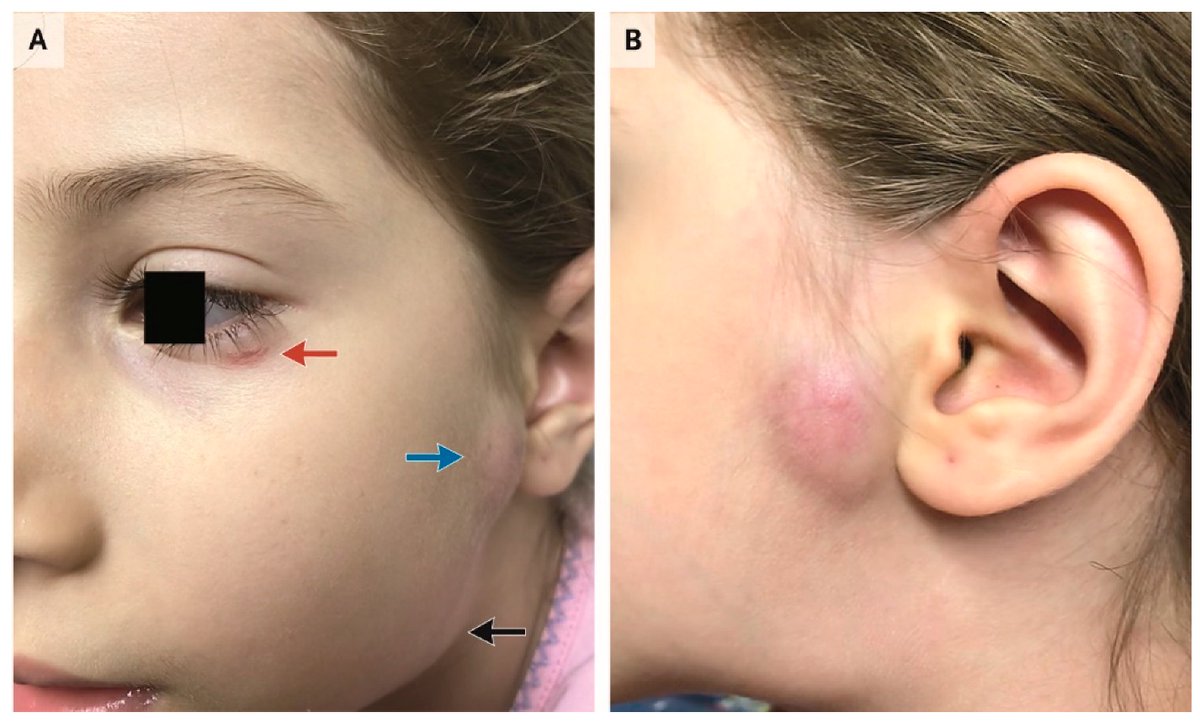
What is oculoglandular syndrome?
👁 findings + LAD seen in:
🔸Tularemia (Francisella) 🐇
🔸Cat-scratch disease (Bartonella) 🐈
🔸Listeriosis 🧀
🔸Sporotrichosis 🌹
🔸Adenovirus infection 👁️
🔸Murine typhus (Rickettsia) 🦟
🔸Lymphogranuloma venereum (LGV; Chlamydia) 🦠
👁 findings + LAD seen in:
🔸Tularemia (Francisella) 🐇
🔸Cat-scratch disease (Bartonella) 🐈
🔸Listeriosis 🧀
🔸Sporotrichosis 🌹
🔸Adenovirus infection 👁️
🔸Murine typhus (Rickettsia) 🦟
🔸Lymphogranuloma venereum (LGV; Chlamydia) 🦠
Let’s focus 🔍 on our approach to cervical lymphadenitis:
📝 history & ⏳ tempo help w/ the DDx!
🔸Recent tonsillitis / pharyngitis? think Streptococcal
🔸Recent facial / neck infection? think Staphylococcal
🔸More indolent course? think TB
🔸Cat exposure? think Bartonella
📝 history & ⏳ tempo help w/ the DDx!
🔸Recent tonsillitis / pharyngitis? think Streptococcal
🔸Recent facial / neck infection? think Staphylococcal
🔸More indolent course? think TB
🔸Cat exposure? think Bartonella
Cervical lymphadenitis in TB is also known as:
💥Scrofula💥
🔹Insidious; fever, systemic sx (wt loss, malaise)
🔹Several enlarged LNs, matted together ➡️ prominent mass
Etio?
-Ingestion of infected milk
-Lymphohematogenous spread from pulmonary focus
-Newer strains of BCG vax
💥Scrofula💥
🔹Insidious; fever, systemic sx (wt loss, malaise)
🔹Several enlarged LNs, matted together ➡️ prominent mass
Etio?
-Ingestion of infected milk
-Lymphohematogenous spread from pulmonary focus
-Newer strains of BCG vax
(Scrofula cont)
🔸Excisional biopsy:
-Dx in ~90% cases
-In MTB endemic regions, FNA provides Dx in >60%
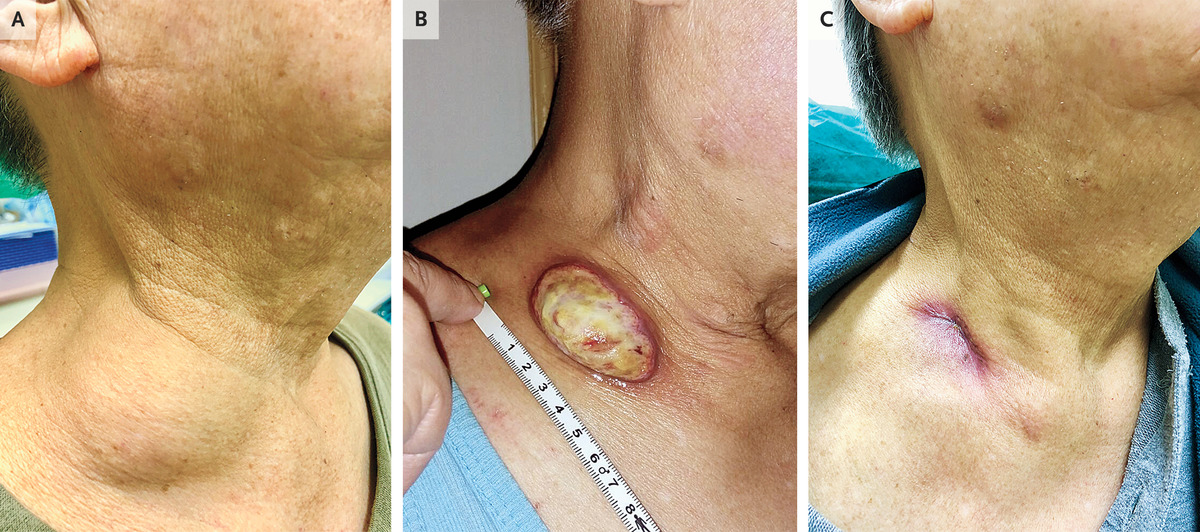
🔺Paradoxical reaction seen in HIV-negative pts receiving MTB lymphadenitis tx 🚨:
-Initial favorable response ➡️ subsequent fever & apparent progression 🤔
🔸Excisional biopsy:
-Dx in ~90% cases
-In MTB endemic regions, FNA provides Dx in >60%
🔺Paradoxical reaction seen in HIV-negative pts receiving MTB lymphadenitis tx 🚨:
-Initial favorable response ➡️ subsequent fever & apparent progression 🤔
Be careful!
MTB lymphadenitis in HIV-positive pts differs from HIV-negative pts
HIV-pos pt (relative to HIV-neg pt):
💥⬆️ frequency of fever 🌡️
💥Concomitant parenchymal (lung) infection
💥Frequent *negative* PPD (anergy)
💥⬆️ frequency of AFB +ve smears on LN biopsy 👇
MTB lymphadenitis in HIV-positive pts differs from HIV-negative pts
HIV-pos pt (relative to HIV-neg pt):
💥⬆️ frequency of fever 🌡️
💥Concomitant parenchymal (lung) infection
💥Frequent *negative* PPD (anergy)
💥⬆️ frequency of AFB +ve smears on LN biopsy 👇

Now that we've covered *infectious* causes of cervical lymphadenitis, let’s do a rapid review of some *NON*-infectious causes of cervical LAD:
💥 Kikuchi-Fujimoto disease
💥 Rosai-Dorfman disease
💥 Kimura disease
💥 Kikuchi-Fujimoto disease
💥 Rosai-Dorfman disease
💥 Kimura disease
⚡️Kikuchi-Fujimoto disease⚡️
Etiology?
🔹Viral
🔸Autoimmune (unknown)
Presentation?
🔹Localized, *tender* cervical LAD
🔸Upper respiratory prodrome +/- fever or rash
🔹Rare! Women <40 y/o
🔸Mild leukopenia
🔹Resolves spontaneously in 1-2 months
Etiology?
🔹Viral
🔸Autoimmune (unknown)
Presentation?
🔹Localized, *tender* cervical LAD
🔸Upper respiratory prodrome +/- fever or rash
🔹Rare! Women <40 y/o
🔸Mild leukopenia
🔹Resolves spontaneously in 1-2 months

⚡️Rosai-Dorfman disease⚡️
Etiology?
🔹Unknown 😭
Presentation?
🔸Extensive, *painless* cervical LAD
🔹Age ~20 y/o
🔸*Fever, neutrophilic leukocytosis, & polyclonal hypergammaglobulinemia*!
🔹Spontaneous remission in ~50% of all pts
🔸Excision of LNs if obstructive complications
Etiology?
🔹Unknown 😭
Presentation?
🔸Extensive, *painless* cervical LAD
🔹Age ~20 y/o
🔸*Fever, neutrophilic leukocytosis, & polyclonal hypergammaglobulinemia*!
🔹Spontaneous remission in ~50% of all pts
🔸Excision of LNs if obstructive complications
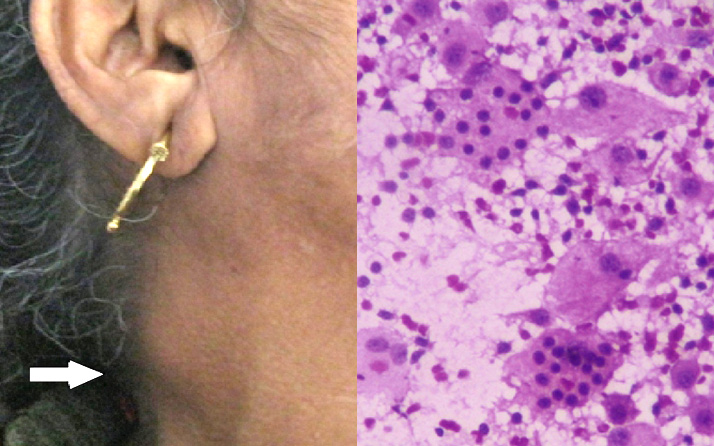
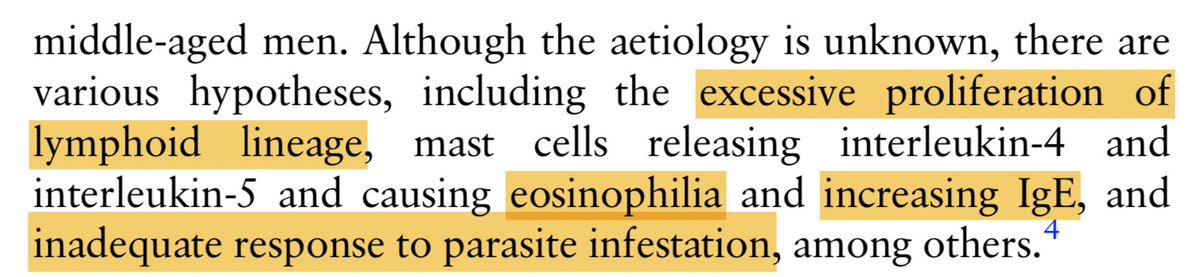
⚡️Kimura disease⚡️
Etiology?
🔹Unknown; hypotheses 👇
Presentation?
🔸Pruritic infiltrative eosinophilic process of soft tissue
🔹Painless cervical LAD
🔸Laboratory findings (*eosinophilia & hyper-IgE*!)
🔹Cytologic abnormalities on FNA confirm the Dx
Etiology?
🔹Unknown; hypotheses 👇
Presentation?
🔸Pruritic infiltrative eosinophilic process of soft tissue
🔹Painless cervical LAD
🔸Laboratory findings (*eosinophilia & hyper-IgE*!)
🔹Cytologic abnormalities on FNA confirm the Dx

Phew, that was a lot!
Thanks for sticking with us til the end 🙂
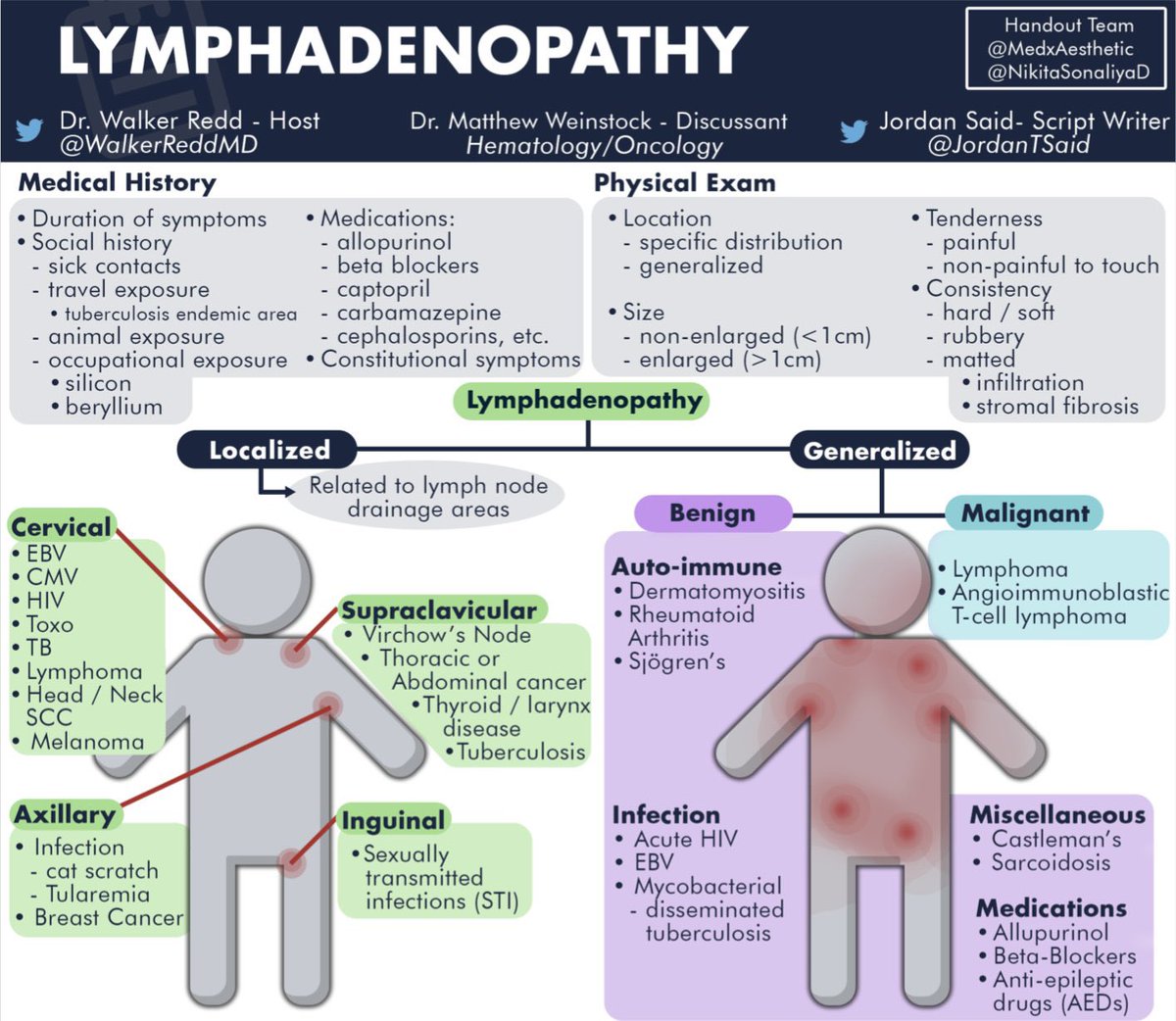
Let’s wrap up this tweetorial with the Run The List infographic on LAD:
Thanks for sticking with us til the end 🙂
Let’s wrap up this tweetorial with the Run The List infographic on LAD:
ICYMI:
Listen to "Episode 48: Lymphadenopathy" on 🍎 pods: apple.co/2XhpRIU
Download the RTL LAD handout (free!) here: runthelistpodcast.com/hematologyonco…
Listen to "Episode 48: Lymphadenopathy" on 🍎 pods: apple.co/2XhpRIU
Download the RTL LAD handout (free!) here: runthelistpodcast.com/hematologyonco…

REFs:
[1-7, 9] aafp.org/afp/2016/1201/…
aafp.org/afp/1998/1015/…
[4] radiologykey.com/neck-lymph-nod…
[6] ncbi.nlm.nih.gov/pmc/articles/P…
teachmeanatomy.info/the-basics/ult…
[7] stanfordmedicine25.stanford.edu/blog/archive/2…
[10-19] Mandell Douglas and Bennett's Principles and Practice of Infectious Diseases, 9th Edition
[1-7, 9] aafp.org/afp/2016/1201/…
aafp.org/afp/1998/1015/…
[4] radiologykey.com/neck-lymph-nod…
[6] ncbi.nlm.nih.gov/pmc/articles/P…
teachmeanatomy.info/the-basics/ult…
[7] stanfordmedicine25.stanford.edu/blog/archive/2…
[10-19] Mandell Douglas and Bennett's Principles and Practice of Infectious Diseases, 9th Edition
REFs (cont):
[11] mdpi.com/2414-6366/5/3/…
[13-15] nejm.org/doi/pdf/10.105…
nejm.org/doi/full/10.10…
pubmed.ncbi.nlm.nih.gov/29135395/
ncbi.nlm.nih.gov/pmc/articles/P…
[17] pubmed.ncbi.nlm.nih.gov/25500707/
ncbi.nlm.nih.gov/pmc/articles/P…
[11] mdpi.com/2414-6366/5/3/…
[13-15] nejm.org/doi/pdf/10.105…
nejm.org/doi/full/10.10…
pubmed.ncbi.nlm.nih.gov/29135395/
ncbi.nlm.nih.gov/pmc/articles/P…
[17] pubmed.ncbi.nlm.nih.gov/25500707/
ncbi.nlm.nih.gov/pmc/articles/P…
REFs (cont):
[18] pubmed.ncbi.nlm.nih.gov/29720485/
hindawi.com/journals/cripa…
[19] ncbi.nlm.nih.gov/pmc/articles/P…
pubmed.ncbi.nlm.nih.gov/26831431/
[18] pubmed.ncbi.nlm.nih.gov/29720485/
hindawi.com/journals/cripa…
[19] ncbi.nlm.nih.gov/pmc/articles/P…
pubmed.ncbi.nlm.nih.gov/26831431/
@MedTweetorials @CPSolvers @COREIMpodcast @CuriousClinPod @DxRxEdu @rabihmgeha @tony_breu @medrants @DavidSteensma
• • •
Missing some Tweet in this thread? You can try to
force a refresh