1/16
Why do B12 and folate deficiencies lead to HUGE red blood cells?
And, if the issue is DNA synthesis, why are red blood cells (which don't have DNA) the key cell line affected?
For answers, we'll have to go back a few billion years.
Why do B12 and folate deficiencies lead to HUGE red blood cells?
And, if the issue is DNA synthesis, why are red blood cells (which don't have DNA) the key cell line affected?
For answers, we'll have to go back a few billion years.
2/
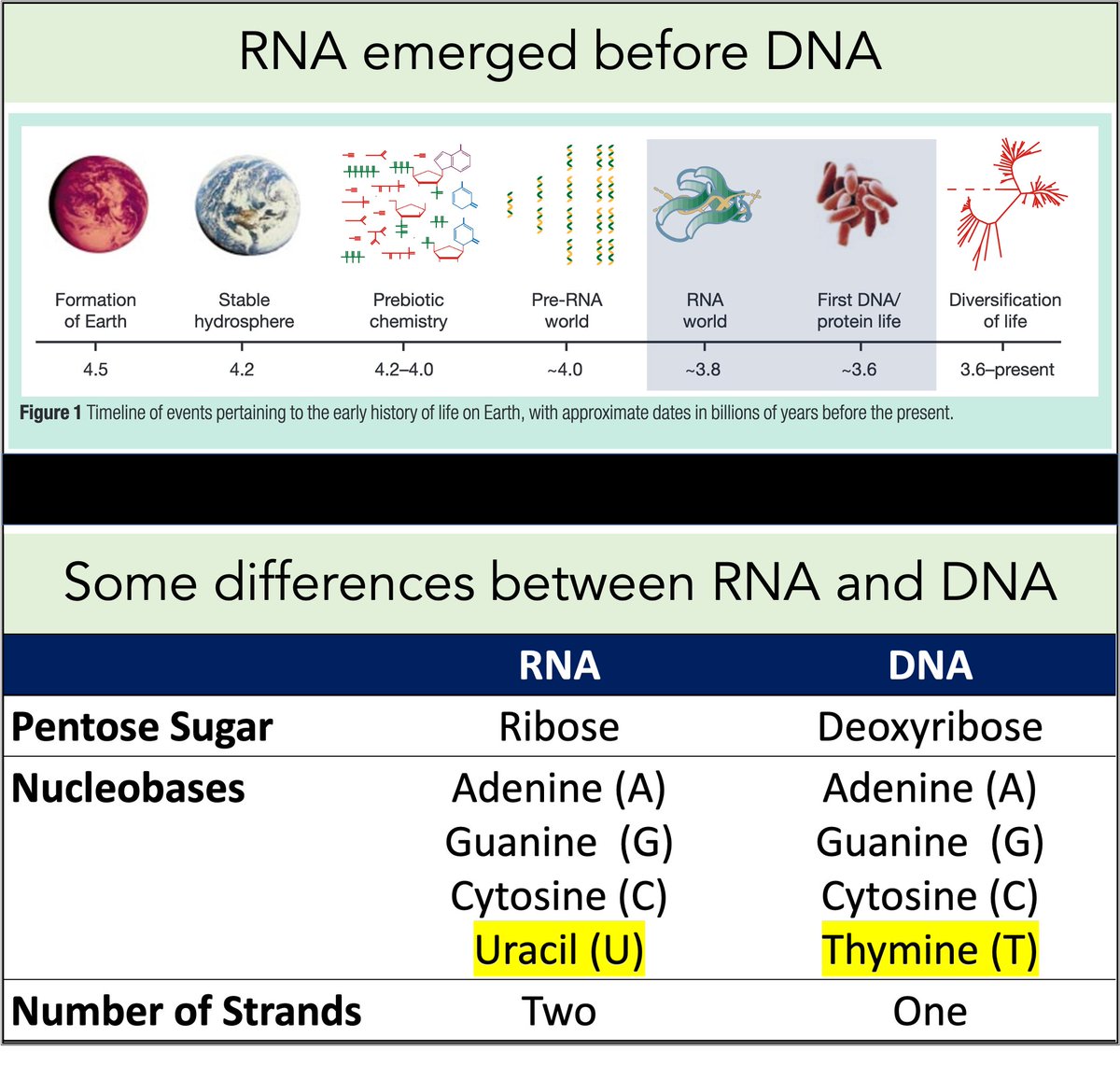
RNA came first. Then, ~3-4 billion years ago, DNA emerged.
Among their differences:
🔹RNA contains uracil
🔹DNA contains thymine
But why does DNA contains thymine (T) instead of uracil (U)?
pubmed.ncbi.nlm.nih.gov/12110897/
RNA came first. Then, ~3-4 billion years ago, DNA emerged.
Among their differences:
🔹RNA contains uracil
🔹DNA contains thymine
But why does DNA contains thymine (T) instead of uracil (U)?
pubmed.ncbi.nlm.nih.gov/12110897/
3/
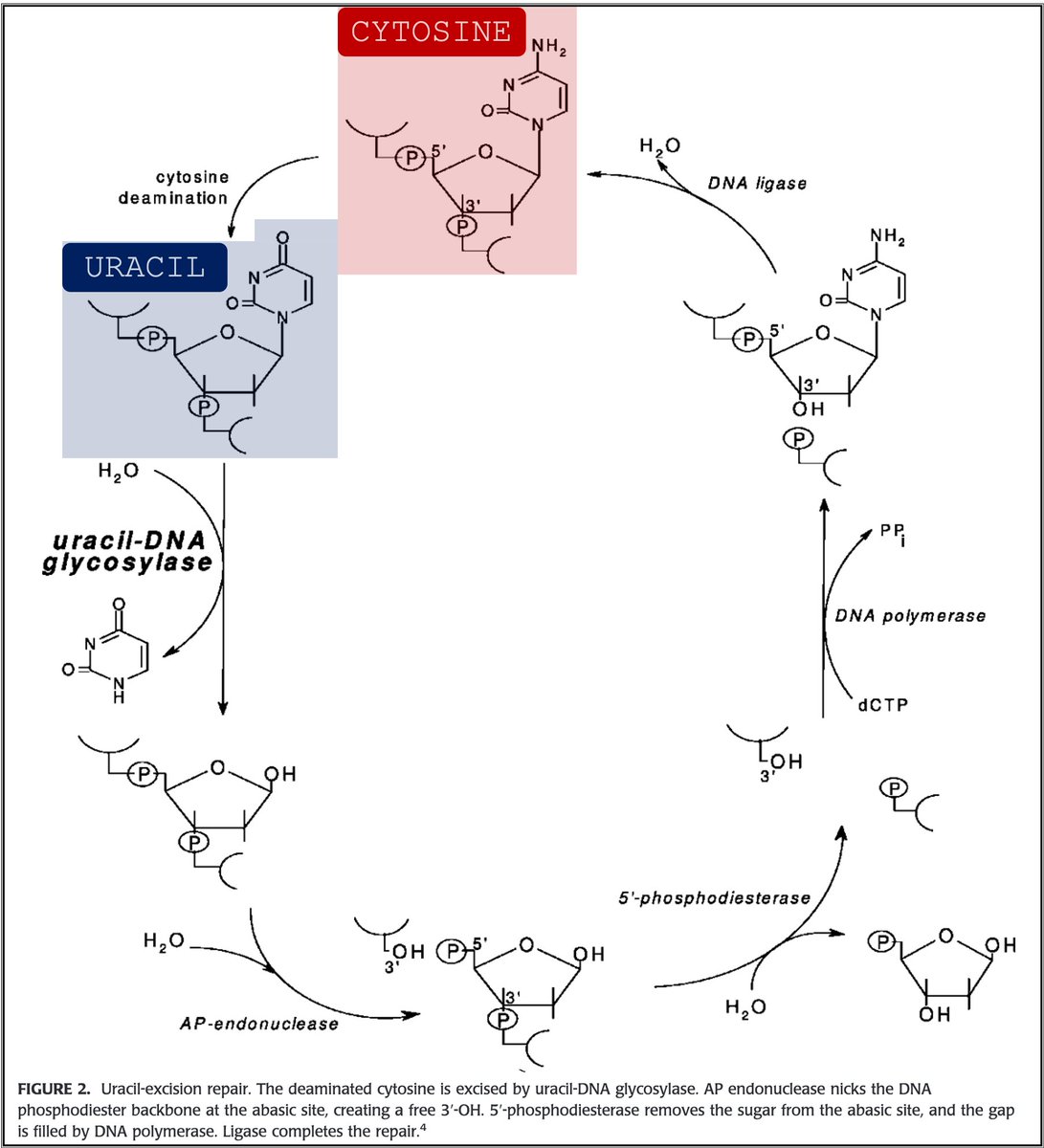
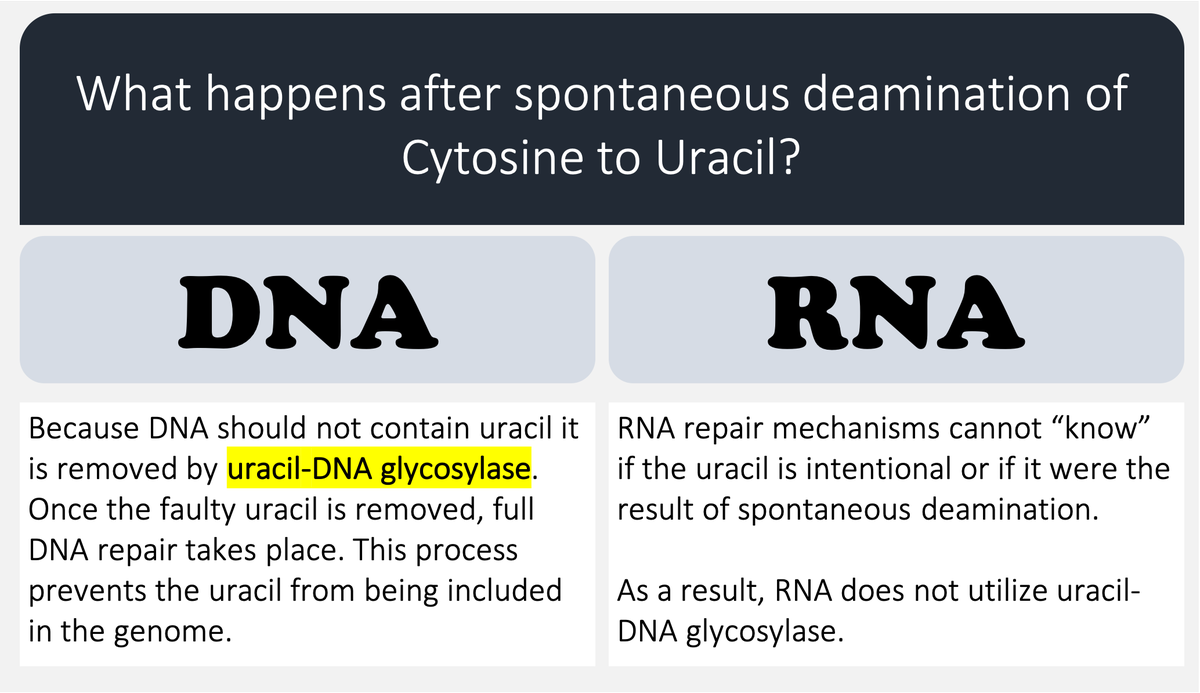
🔑Cytosine (C) can undergo spontaneous deamination to uracil (U).
In the RNA world, this meant that U could appear intensionally or unintentionally. This is clearly problematic. How can you repair RNA when you can't tell if something is an error?
pubmed.ncbi.nlm.nih.gov/18837522/
🔑Cytosine (C) can undergo spontaneous deamination to uracil (U).
In the RNA world, this meant that U could appear intensionally or unintentionally. This is clearly problematic. How can you repair RNA when you can't tell if something is an error?
pubmed.ncbi.nlm.nih.gov/18837522/
4/
DNA's use of T instead of U means that spontaneous C → U deamination can be corrected without worry that an intentional U is being removed.
DNA requires greater stability than RNA so the transition to a thymine-based structure was beneficial.
pubmed.ncbi.nlm.nih.gov/18837522/
DNA's use of T instead of U means that spontaneous C → U deamination can be corrected without worry that an intentional U is being removed.
DNA requires greater stability than RNA so the transition to a thymine-based structure was beneficial.
pubmed.ncbi.nlm.nih.gov/18837522/
5/
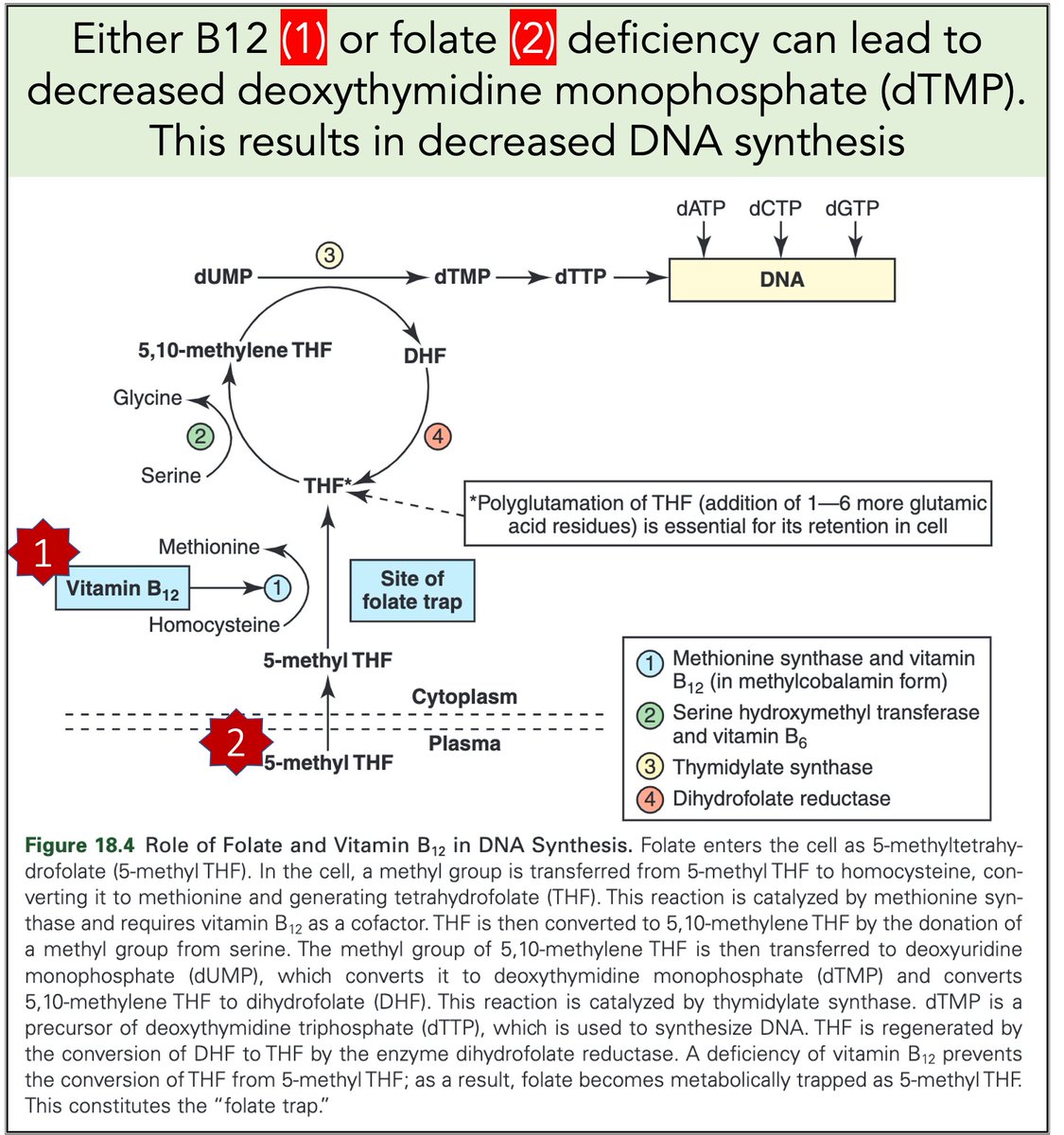
Let's return to megaloblastic anemia secondary to B12 or folate deficiency.
When either is severely deficient deoxythymidine monophosphate (dTMP*) production is hindered. With less dTMP, DNA synthesis is abnormal.
[*Note: thymine is the base in dTMP]
sciencedirect.com/science/articl…
Let's return to megaloblastic anemia secondary to B12 or folate deficiency.
When either is severely deficient deoxythymidine monophosphate (dTMP*) production is hindered. With less dTMP, DNA synthesis is abnormal.
[*Note: thymine is the base in dTMP]
sciencedirect.com/science/articl…
6/
So one hypothesis is that megaloblastic anemia results from a deficiency in dTMP leading to an issue with DNA elongation (i.e., addition of nucleotides)
Some (#1) but not all (#2) data support this.
There is more to it.
1. pubmed.ncbi.nlm.nih.gov/5657159/
2. pubmed.ncbi.nlm.nih.gov/6277361/
So one hypothesis is that megaloblastic anemia results from a deficiency in dTMP leading to an issue with DNA elongation (i.e., addition of nucleotides)
Some (#1) but not all (#2) data support this.
There is more to it.
1. pubmed.ncbi.nlm.nih.gov/5657159/
2. pubmed.ncbi.nlm.nih.gov/6277361/
7/
To add to our explanation for how B12 and folate deficiencies hinder DNA synthesis, look back at the figure in tweet 5.
What would you anticipate increases in concentration in the setting of B12 or folate deficiency?
To add to our explanation for how B12 and folate deficiencies hinder DNA synthesis, look back at the figure in tweet 5.
What would you anticipate increases in concentration in the setting of B12 or folate deficiency?
8/
B12 and/or folate deficiency result in issues with dTMP production. As dUMP is the precursor, the ratio of dUMP/dTMP rises.
Result: dUTP (uracil + deoxyribose triphosphate) is incorporated into DNA where dTTP should be!
pubmed.ncbi.nlm.nih.gov/2705438/
B12 and/or folate deficiency result in issues with dTMP production. As dUMP is the precursor, the ratio of dUMP/dTMP rises.
Result: dUTP (uracil + deoxyribose triphosphate) is incorporated into DNA where dTTP should be!
pubmed.ncbi.nlm.nih.gov/2705438/

9/
But uracil doesn't belong in DNA!
In response to this misincorporation, attempts are made to repair these strands. U is removed but there isn't enough T to fill the gaps. Single and double-stranded breaks form resulting in non-functional DNA.
pubmed.ncbi.nlm.nih.gov/9096386/
But uracil doesn't belong in DNA!
In response to this misincorporation, attempts are made to repair these strands. U is removed but there isn't enough T to fill the gaps. Single and double-stranded breaks form resulting in non-functional DNA.
pubmed.ncbi.nlm.nih.gov/9096386/

10/
Without functional DNA, cell division is halted. RBC precursors undergo apoptosis.
Result: "ineffective erythropoiesis" and anemia!
To this point we've explained the anemia but haven't yet explained why the resulting RBCs are so large. That's next.
pubmed.ncbi.nlm.nih.gov/9192787/
Without functional DNA, cell division is halted. RBC precursors undergo apoptosis.
Result: "ineffective erythropoiesis" and anemia!
To this point we've explained the anemia but haven't yet explained why the resulting RBCs are so large. That's next.
pubmed.ncbi.nlm.nih.gov/9192787/

11/
Remember that RNA doesn't uses thymine (it uses uracil). And only the thymine containing nucleotide (dTMP) requires B12/folate.
🔑Result: In B12/folate deficiencies, RNA synthesis is relatively unaffected!
pubmed.ncbi.nlm.nih.gov/5640627/
Remember that RNA doesn't uses thymine (it uses uracil). And only the thymine containing nucleotide (dTMP) requires B12/folate.
🔑Result: In B12/folate deficiencies, RNA synthesis is relatively unaffected!
pubmed.ncbi.nlm.nih.gov/5640627/

12/
In the nuclei of B12/folate deficient RBC precursors, DNA synthesis is poor leaving cells stalled and unable to divide.
But, in the cytoplasm, RNA and protein synthesis continues unabated.
Result: "nuclear-cytoplasmic asynchrony"
In the nuclei of B12/folate deficient RBC precursors, DNA synthesis is poor leaving cells stalled and unable to divide.
But, in the cytoplasm, RNA and protein synthesis continues unabated.
Result: "nuclear-cytoplasmic asynchrony"
13/
Precursors with nuclear-cytoplasmic asynchrony are unable to divide into daughter cells. But the cytoplasm continues to expand.
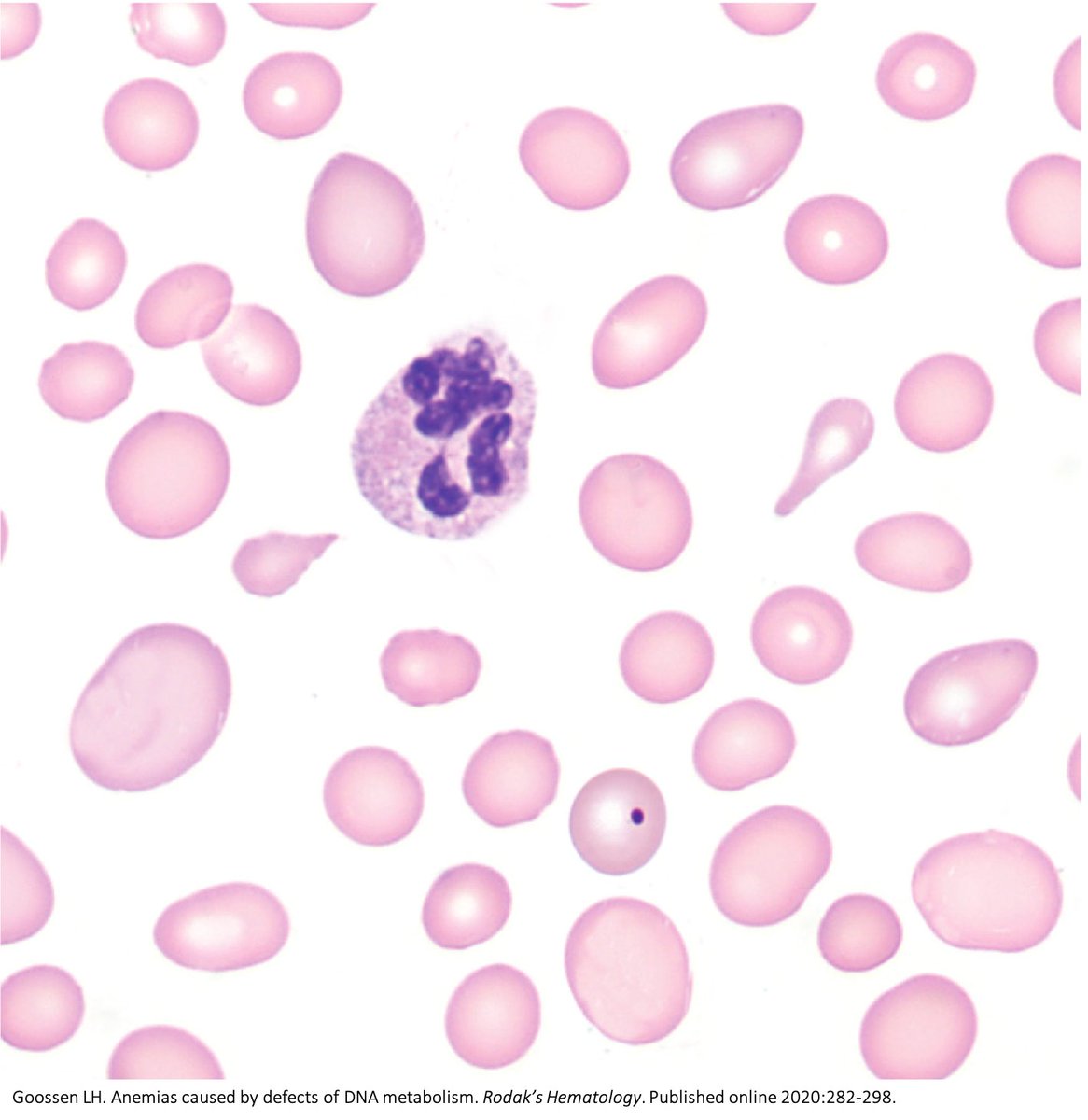
When survivors eventually cast off their nucleus (and its DNA!) and appear in the peripheral blood, they will be huge.
They will be macrocytic!
Precursors with nuclear-cytoplasmic asynchrony are unable to divide into daughter cells. But the cytoplasm continues to expand.
When survivors eventually cast off their nucleus (and its DNA!) and appear in the peripheral blood, they will be huge.
They will be macrocytic!
14/
There are other explanations (see link).
And I admit this doesn't really explain why RBCs are more affected than other cell lines (though all ARE affected).
AND, why are neutrophils hypersegmented?
For these unanswered questions, I seek your help.
pubmed.ncbi.nlm.nih.gov/16103708/
There are other explanations (see link).
And I admit this doesn't really explain why RBCs are more affected than other cell lines (though all ARE affected).
AND, why are neutrophils hypersegmented?
For these unanswered questions, I seek your help.
pubmed.ncbi.nlm.nih.gov/16103708/
15/
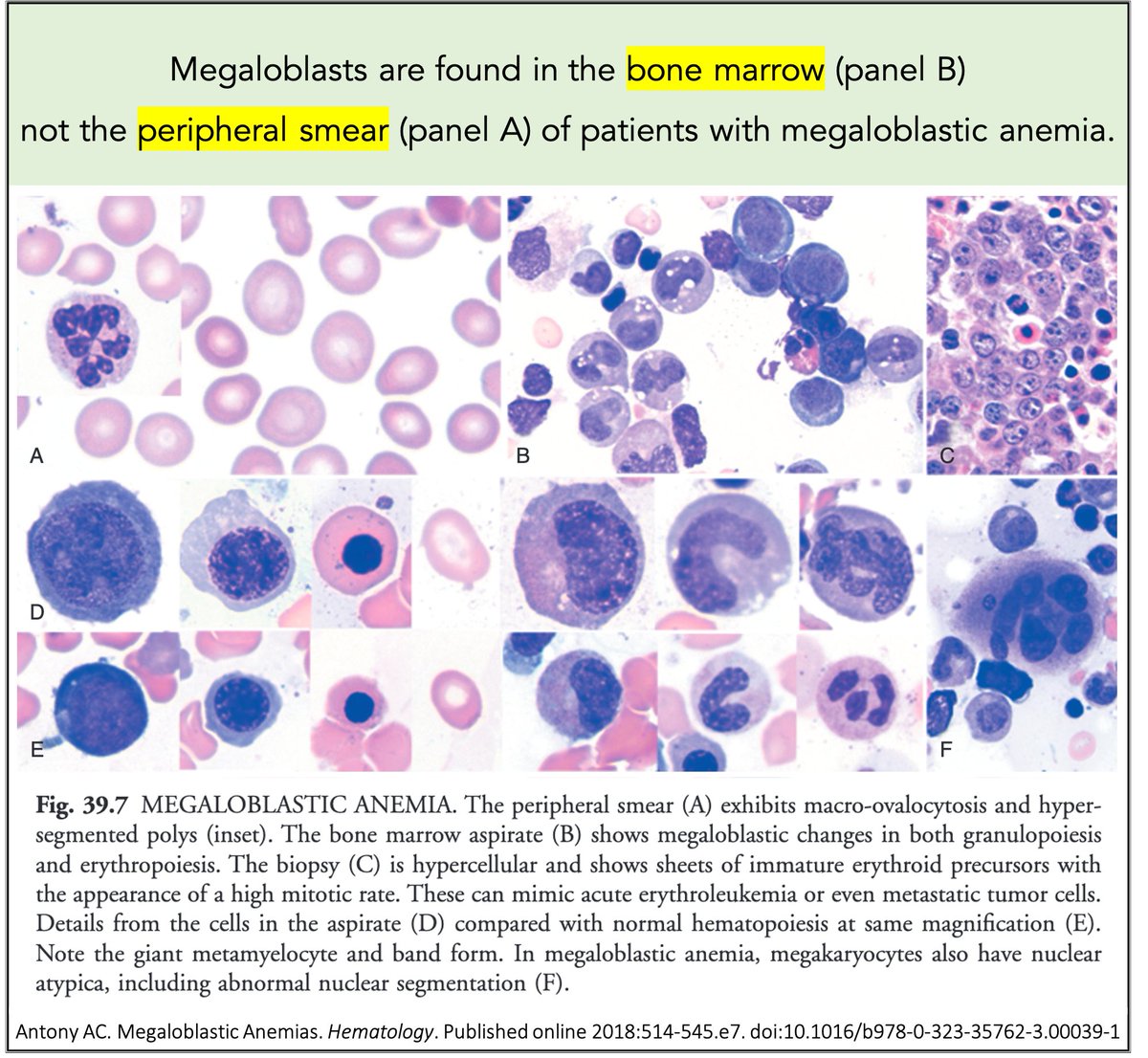
Before closing, full disclosure: I had NO IDEA what "megaloblastic" referred to.
Was it the big RBCs? Was it the hypersegmented neutrophils?
Nope.
Megaloblasts are in the bone marrow. We still use this term despite the fact that nowadays most patients don't under biopsy.
Before closing, full disclosure: I had NO IDEA what "megaloblastic" referred to.
Was it the big RBCs? Was it the hypersegmented neutrophils?
Nope.
Megaloblasts are in the bone marrow. We still use this term despite the fact that nowadays most patients don't under biopsy.
16/16
➤In megaloblastic anemia, DNA synthesis is hindered by decreased dTTP and increased incorporation of dUTP
➤RNA synthesis remain relatively unaffected
➤This leads to:
💥Ineffective erythropoiesis ➛ anemia
💥Nuclear-cytoplasmic asynchrony ➛ macrocytosis
➤In megaloblastic anemia, DNA synthesis is hindered by decreased dTTP and increased incorporation of dUTP
➤RNA synthesis remain relatively unaffected
➤This leads to:
💥Ineffective erythropoiesis ➛ anemia
💥Nuclear-cytoplasmic asynchrony ➛ macrocytosis
• • •
Missing some Tweet in this thread? You can try to
force a refresh