How often do you check for Primary Aldosteronism (PA)?
Chances are, NOT nearly often enough!
VA study reveals widespread undertesting...can we do better?
acpjournals.org/doi/10.7326/M2…
If you've seen 10 pt's with HTN ➡️ you've probably seen PA!
Let's review in this #medtweetorial
Chances are, NOT nearly often enough!
VA study reveals widespread undertesting...can we do better?
acpjournals.org/doi/10.7326/M2…
If you've seen 10 pt's with HTN ➡️ you've probably seen PA!
Let's review in this #medtweetorial
I feel comfortable diagnosing Primary Aldosteronism
3/ First, why even check for PA?
🚫🦓It's NOT a zebra‼️
It IS one of the most common causes of 2* HTN:
📛5-10% of those w/ HTN
📛20% w/ resistant HTN
Have you seen 10 patients with HTN?
If yes, you've likely seen PA!
🚫🦓It's NOT a zebra‼️
It IS one of the most common causes of 2* HTN:
📛5-10% of those w/ HTN
📛20% w/ resistant HTN
Have you seen 10 patients with HTN?
If yes, you've likely seen PA!
4/ Why check for PA?
It's common & it's BAD.
PA causes HTN &:
💔3.7x ⬆️CHF
🧠4.2x ⬆️CVA
🫀 6.5x ⬆️MI
💗12.1x⬆️AF
😬 & LVH, Diastolic🔻, tissue fibrosis, kidney damage
Ooof...that's a LOT of badness.
Wouldn't it be great if we could treat this...wait we can⁉️
Do tell...
It's common & it's BAD.
PA causes HTN &:
💔3.7x ⬆️CHF
🧠4.2x ⬆️CVA
🫀 6.5x ⬆️MI
💗12.1x⬆️AF
😬 & LVH, Diastolic🔻, tissue fibrosis, kidney damage
Ooof...that's a LOT of badness.
Wouldn't it be great if we could treat this...wait we can⁉️
Do tell...

5/ Why check for PA?
It's common, & it's bad, BUT it's treatable & potentially even curable❗️
Diagnosis➡️
🔪Surgical cure if unilat
💊Effective med rx if b/l
Many deleterious PA effects are reversible.
BUT you have to diagnose it first!!!
Let's bust some myths.
It's common, & it's bad, BUT it's treatable & potentially even curable❗️
Diagnosis➡️
🔪Surgical cure if unilat
💊Effective med rx if b/l
Many deleterious PA effects are reversible.
BUT you have to diagnose it first!!!
Let's bust some myths.
6/ Fact vs Fiction
Primary Aldosteronism is a rare zebra!
Primary Aldosteronism is a rare zebra!
7/ Good, you were paying attention!
PA is present in:
🧮~11% of HTN patients in specialized centers
🧮& ~6% in PCP clinics.
pubmed.ncbi.nlm.nih.gov/17161262/
pubmed.ncbi.nlm.nih.gov/28385310/
------------------------
NEXT:
Only screen those with HTN & ⬇️K because Aldo ⬆️K loss.
PA is present in:
🧮~11% of HTN patients in specialized centers
🧮& ~6% in PCP clinics.
pubmed.ncbi.nlm.nih.gov/17161262/
pubmed.ncbi.nlm.nih.gov/28385310/
------------------------
NEXT:
Only screen those with HTN & ⬇️K because Aldo ⬆️K loss.
8/ Correct! That was FICTION…one I falsely lived by for years!
YES: Aldo --> ⬆️K loss
BUT the MAJORITY of those w/ PA have NORMAL K
SO: look beyond the K when screening
------------------------
NEXT:
Aldo must be HIGH if the pt has primary aldosteronISM.
YES: Aldo --> ⬆️K loss
BUT the MAJORITY of those w/ PA have NORMAL K
SO: look beyond the K when screening
------------------------
NEXT:
Aldo must be HIGH if the pt has primary aldosteronISM.
9/ Indeed, patients with PA need NOT have high aldo level because:
- Low-renin normo-aldo cases exist
- Aldo secretion is pulsatile
- If very aldo-sensitive, can have PA with mild elevation
Don't just look at absolute plasma aldo conc (PAC) but also the aldo/renin ratio (ARR).
- Low-renin normo-aldo cases exist
- Aldo secretion is pulsatile
- If very aldo-sensitive, can have PA with mild elevation
Don't just look at absolute plasma aldo conc (PAC) but also the aldo/renin ratio (ARR).
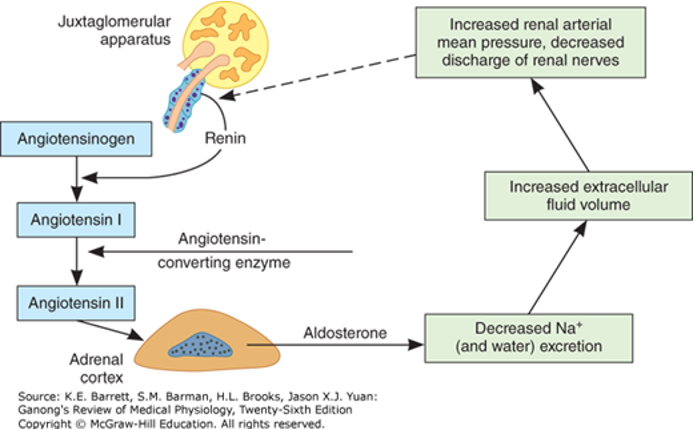
10/ To understand testing, first let's quickly review aldo physiology.
Here's the normal endocrine axis.
Normally, aldo secretion is renin-dependent (via Ang II) & causes:
⬆️BP, Na, HCO3
⬇️low K
In addition, Aldo is:
📉Inhibited by Na & fluid
📈Stimulated by K, Ang II, ACTH
Here's the normal endocrine axis.
Normally, aldo secretion is renin-dependent (via Ang II) & causes:
⬆️BP, Na, HCO3
⬇️low K
In addition, Aldo is:
📉Inhibited by Na & fluid
📈Stimulated by K, Ang II, ACTH
11/ Two concepts about PA:
#1⃣ Aldo secretion becomes autonomous.
✖️Independent of renin. ⬆️Aldo=⬆️BP,Na,Fluid=⬇️Renin
✖️Insensitive to normal breaks.
So ⬆️BP,Na,Fluid FAIL to supress Aldo secretion.
Results:
⏫Aldo-to-Renin Ratio (ARR)
🚫Salt challenge doesn't⬇️Aldo
#1⃣ Aldo secretion becomes autonomous.
✖️Independent of renin. ⬆️Aldo=⬆️BP,Na,Fluid=⬇️Renin
✖️Insensitive to normal breaks.
So ⬆️BP,Na,Fluid FAIL to supress Aldo secretion.
Results:
⏫Aldo-to-Renin Ratio (ARR)
🚫Salt challenge doesn't⬇️Aldo

12/ Two concepts about PA:
#2⃣ Aldo can become autonomous via several mechanisms.
🔪Surgically curable, often aldo-producing adenoma --> adrenalectomy
💊Surgically incurable, often b/l adrenal hyperplasia --> MRA
Adrenal vein sampling (AVS) is 🔑 to diagnosing uni vs bilat dx!
#2⃣ Aldo can become autonomous via several mechanisms.
🔪Surgically curable, often aldo-producing adenoma --> adrenalectomy
💊Surgically incurable, often b/l adrenal hyperplasia --> MRA
Adrenal vein sampling (AVS) is 🔑 to diagnosing uni vs bilat dx!

13/ Now you're ready to diagnose PA!
First whom to screen?
2017 ACC/AHA HTN Guidelines
✅Resistant HTN
✅HTN & ⬇️K
✅Adrenal mass
✅FHx early HTN
✅Stroke at <40yrs
BUT recall PA is common even in routine normo-K HTN? May consider more liberal testing.
ahajournals.org/doi/10.1161/HY…
First whom to screen?
2017 ACC/AHA HTN Guidelines
✅Resistant HTN
✅HTN & ⬇️K
✅Adrenal mass
✅FHx early HTN
✅Stroke at <40yrs
BUT recall PA is common even in routine normo-K HTN? May consider more liberal testing.
ahajournals.org/doi/10.1161/HY…


14/ Ok, the Dx isn't straightforward, but some pearls:
1⃣Consider BOTH ARR & PAC
2⃣If ARR is super high, proceed; if moderate, retest
3⃣Salt/saline/ACE challenge may help exclude PA
4⃣Imaging is important but not enough
5⃣AVS is key to finding curable dx if surgery is an option
1⃣Consider BOTH ARR & PAC
2⃣If ARR is super high, proceed; if moderate, retest
3⃣Salt/saline/ACE challenge may help exclude PA
4⃣Imaging is important but not enough
5⃣AVS is key to finding curable dx if surgery is an option

15/ RAAS axis is complex & interactions confound diagnosis; know these!
For ex:
⬇️K suppresses Aldo = false negative. So correct K before testing for PA.
Don't need to withdraw BP meds, but understand how they affect ARR. BBs lower Aldo so if PAC is high on BB, PA is likely.
For ex:
⬇️K suppresses Aldo = false negative. So correct K before testing for PA.
Don't need to withdraw BP meds, but understand how they affect ARR. BBs lower Aldo so if PAC is high on BB, PA is likely.

16/ Nuances of PA dx go beyond this #tweetorial, but are important, so here are some resources:
jacc.org/doi/full/10.10…
nephjc.com/news/aldostero… @nsmcinternship
nephjc.com/freelyfiltered… @NephJC_Podcast
Get help from your local HTN specialist!
jacc.org/doi/full/10.10…
nephjc.com/news/aldostero… @nsmcinternship
nephjc.com/freelyfiltered… @NephJC_Podcast
Get help from your local HTN specialist!
17/ Let’s review:
✅PA is common & undertested
✅PA has bad CV effects, BUT is treatable
✅Screen: resistent HTN, low K, Fhx early HTN, stroke at <40 yrs, adrenal mass...but probably many others
✅ARR is key but know the caveats
✅Imaging is important, but AVS is critical
✅PA is common & undertested
✅PA has bad CV effects, BUT is treatable
✅Screen: resistent HTN, low K, Fhx early HTN, stroke at <40 yrs, adrenal mass...but probably many others
✅ARR is key but know the caveats
✅Imaging is important, but AVS is critical
I feel comfortable diagnosing Primary Aldosteronism
#MedTwitter #CardioTwitter, thanks for reading!
Would love your feedback and pearls about PA!
How often do you screen for primary aldosteronsim?
What are your thoughts about adrenal vein sampling?
What are other sources to learn more?
Would love your feedback and pearls about PA!
How often do you screen for primary aldosteronsim?
What are your thoughts about adrenal vein sampling?
What are other sources to learn more?

I learned something in this Tweetorial that might change my practice.
• • •
Missing some Tweet in this thread? You can try to
force a refresh