
ACC/CCA COVID Webinar - Serious Illness.
Hope everyone can join!
This will pair very well with @CardioNerds Episode #20 on COVID in the ICU: cardionerds.com/episodes/covid…
Hope everyone can join!
This will pair very well with @CardioNerds Episode #20 on COVID in the ICU: cardionerds.com/episodes/covid…
Starting off with a case presentation.
31 M p/w fever, cough. from Wuhan
H/o DM & HLD
T 38.5C, HR 152, RR 24, BP 134/107
⬇️wbc & plt
⬆️CRP
🤒CT with patchy opacities including ground glass
31 M p/w fever, cough. from Wuhan
H/o DM & HLD
T 38.5C, HR 152, RR 24, BP 134/107
⬇️wbc & plt
⬆️CRP
🤒CT with patchy opacities including ground glass




Bloodwork.
CT.
CT.


Diagnosis

💊Treatments


Takes a turn for the worse
💔Heart Failure by Day 2, LVEF 60%, nondilated
💊Diuretics, Digoxin, Morphine, BiPAP
💔Heart Failure by Day 2, LVEF 60%, nondilated
💊Diuretics, Digoxin, Morphine, BiPAP




Bloodwork trends...
Note: lymphopenia, thrombocytopenia, inflammation
⬆️pro-BNP, TnI, LFT, D-dimer --> WHY?
Note: lymphopenia, thrombocytopenia, inflammation
⬆️pro-BNP, TnI, LFT, D-dimer --> WHY?

😷There is multorgan dysfunction.
🧐Why is there heart failure?
- hypoxic injury? myocarditis?
🧐Why is there heart failure?
- hypoxic injury? myocarditis?
Echo seems ok on face value.
But clincial presentation with heart failure and hypotension seems out of proportion...why?
But clincial presentation with heart failure and hypotension seems out of proportion...why?
Thankfully, with dilignet supportive care, patinet makes a recovery 🙏
But many questions remain..
- why proBNP and TnI elevation?
- why d-dimer elevated?
- best treatment plan?
- role of anti-inflammation Rx?
Ongoing study of Tocilizumab, anti-Il-6 Ab.
But many questions remain..
- why proBNP and TnI elevation?
- why d-dimer elevated?
- best treatment plan?
- role of anti-inflammation Rx?
Ongoing study of Tocilizumab, anti-Il-6 Ab.
Now let's pivot to the use of ECMO with Prof Ning Zhou MD PhD

Wuhan is the epicenter of this epidemic.
BUT, the # of NEW confirmed cases today - March 19 2020 is...
ZERO! 🙏
BUT, the # of NEW confirmed cases today - March 19 2020 is...
ZERO! 🙏

Sadly,
~20 of COVID-19 patients --> SEVERE or CRITICALLY ill🥵
1. Resp failure
2. Shock
3. Multiorgan dysfunction
~20 of COVID-19 patients --> SEVERE or CRITICALLY ill🥵
1. Resp failure
2. Shock
3. Multiorgan dysfunction
What to do if hypoxic respiratory failure is refractory to mechanical ventillation?
Ans: ECMO!
Let's tackle a case (next)
Ans: ECMO!
Let's tackle a case (next)

50 yo M p/w fever and sob. From Wuhan with known COVID-19 contacts.
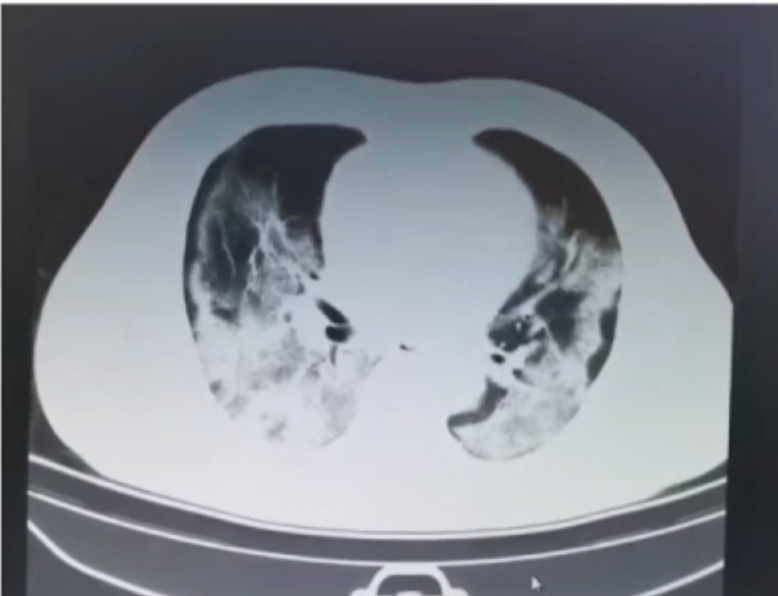
Hypoxic with infiltrates & groung glass on CT
Labs:
- ⬆️hsCRP, LFT, NT-proBNP, TnI, PO2
- ⬇️Lymphocyte
TTE: EF 45%
Hypoxic with infiltrates & groung glass on CT
Labs:
- ⬆️hsCRP, LFT, NT-proBNP, TnI, PO2
- ⬇️Lymphocyte
TTE: EF 45%



Rx:
- anti-bacterial
- anti-viral
- asthma Rx and respiratory clearance
- nutrition
- chinese traditional Rx
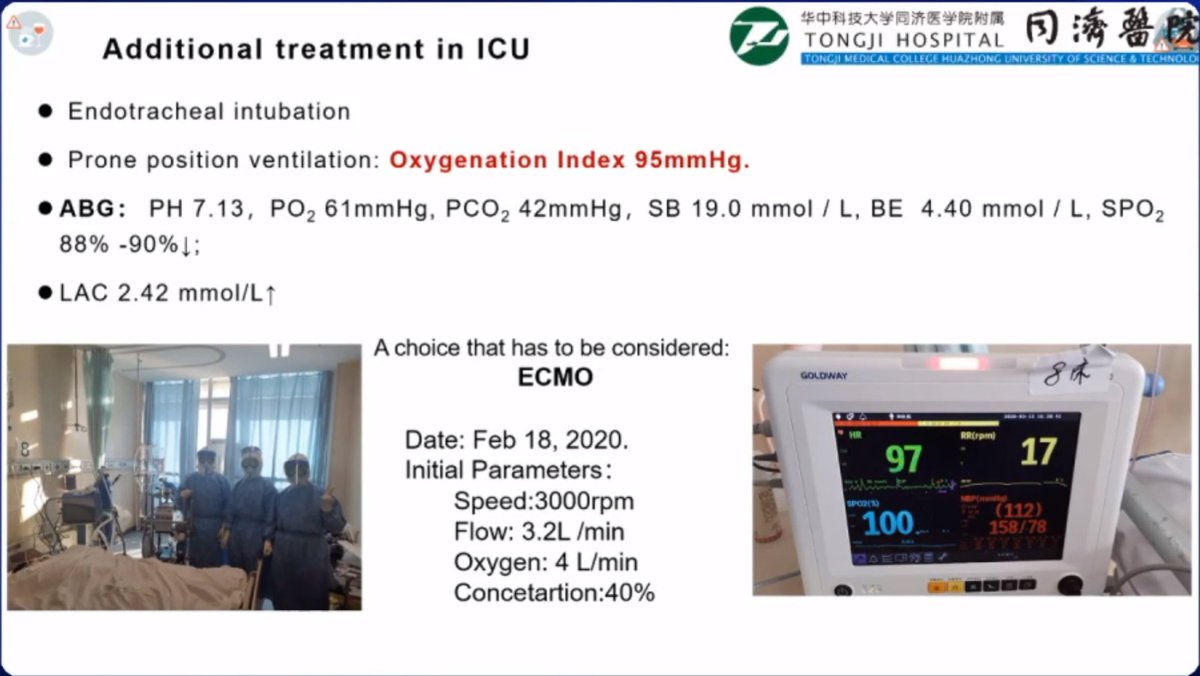
BUT: rapid worsening of respiratory failure --> ARDS
- Prone position ventillation --> hypoxia
- Lactate rising
NEXT?
--> VV-ECMO
- anti-bacterial
- anti-viral
- asthma Rx and respiratory clearance
- nutrition
- chinese traditional Rx
BUT: rapid worsening of respiratory failure --> ARDS
- Prone position ventillation --> hypoxia
- Lactate rising
NEXT?
--> VV-ECMO

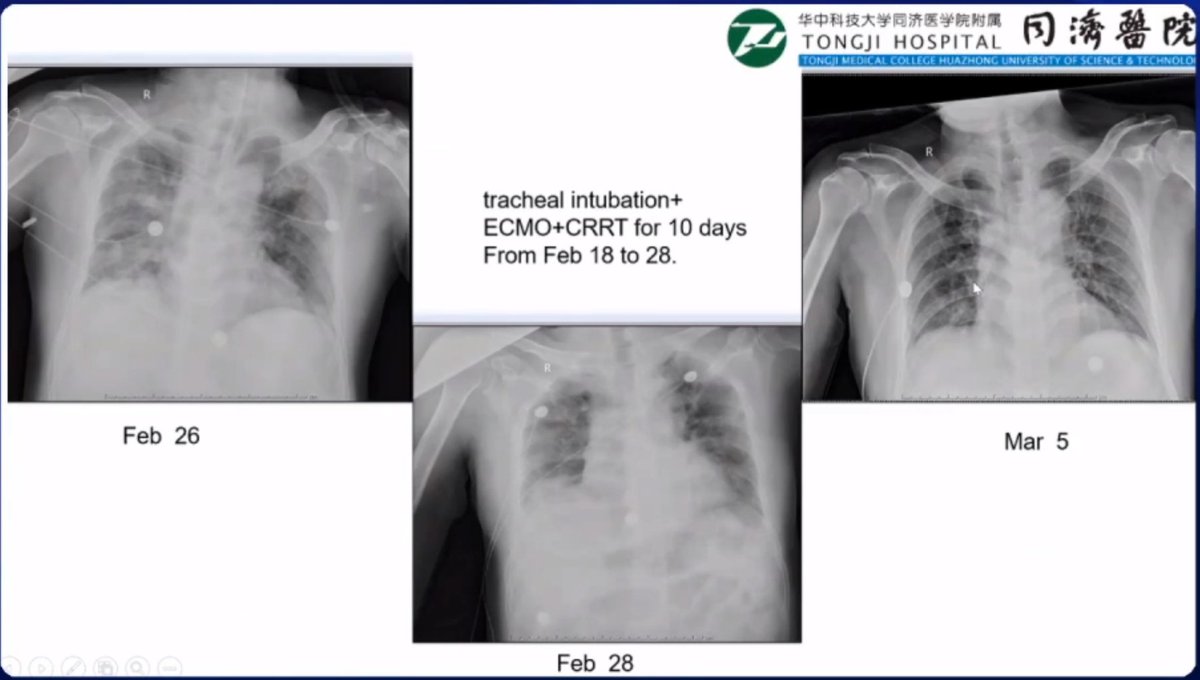
Thankfully,
Imroving with max support on VV-ECMO x10 days
Result: another patient saved
Great work team!
Imroving with max support on VV-ECMO x10 days
Result: another patient saved
Great work team!


So far they've had 5 patients on ECMO
4 recovered, 1 ongoing
4 VV-ECMO, 1 VA-ECMO
Duration ~9.2 days, range 6-13 days
4 recovered, 1 ongoing
4 VV-ECMO, 1 VA-ECMO
Duration ~9.2 days, range 6-13 days
Lessons learned:
✅Indications:
- not standard, don't wait for last resort
- need to lower threshold
- don't wait for severe hypoxia which leads to multiorgan failure
- don't do ECMO when patient is dying
✅Indications:
- not standard, don't wait for last resort
- need to lower threshold
- don't wait for severe hypoxia which leads to multiorgan failure
- don't do ECMO when patient is dying
🚫Contraindications:
- bleeding (need anticoagulation)
- irreversible severe brain injury
- poor outlook: deathly ill, advanced age
Don't have ECMO for everyone...we have to choose patients who are more likely to recover
- bleeding (need anticoagulation)
- irreversible severe brain injury
- poor outlook: deathly ill, advanced age
Don't have ECMO for everyone...we have to choose patients who are more likely to recover
⏳When to start ECMO:
- earlier is probably better, if progression is ominous
- if wait too long, may loose the chance to recover them
- ECMO is not just to prolong life for couple days...want to use for SURVIVAL 👏
- earlier is probably better, if progression is ominous
- if wait too long, may loose the chance to recover them
- ECMO is not just to prolong life for couple days...want to use for SURVIVAL 👏
⚖️Which ECMO?
1st is VV-ECMO - for severe respiratory failure not responding to mechanical ventillation
BUT if cardiac dysfunction 💔 --> don't forget they may need a VA-ECMO
1st is VV-ECMO - for severe respiratory failure not responding to mechanical ventillation
BUT if cardiac dysfunction 💔 --> don't forget they may need a VA-ECMO
Intubation and mechanical ventillation:
- risk of transmission
- resource limitation
- interrupts airway clearance
Is there a place for VV-ECMO without intubation⁉️
Hmmm...🤨
Something maybe worth considering.
- risk of transmission
- resource limitation
- interrupts airway clearance
Is there a place for VV-ECMO without intubation⁉️
Hmmm...🤨
Something maybe worth considering.
"I would like to say thank you to my patients...
...they are the heros of my city" (Wuhan, China)
...they are the heros of my city" (Wuhan, China)
I personally am in awe of these incredible doctores, on the frontlines, not just battling COVID-19 in the wards, but taking the time to describe their experience and teach us globally.
Q: What is indicatin for VA ECMO in COVID-19⁉️
-Not all 🏥have ECMO...limited availability
-Most often using VV-ECMO <-- hypoxemia is #1⃣
-VA-ECMO: ⏫Afterload > bad for ♥️
-BUT: if heart failure 💔 & Hypoxia
--> VA-ECMO + Impella
-Not all 🏥have ECMO...limited availability
-Most often using VV-ECMO <-- hypoxemia is #1⃣
-VA-ECMO: ⏫Afterload > bad for ♥️
-BUT: if heart failure 💔 & Hypoxia
--> VA-ECMO + Impella
Emphasize: activate VV-ECMO EARLY if patient will likely need it, to prevent worsening. Once they develop multiorgan failure from severe hypoxemia --> may be too late.
ok ok ...so if we need to activate early, but still be judicious...is there a risk score? How do we balance this?
Is there a way to identify the sickest?
Ans:
- no risk score; clinical judgement
- oxygen, lactate, liver & kidney function
Is there a way to identify the sickest?
Ans:
- no risk score; clinical judgement
- oxygen, lactate, liver & kidney function
Q: How did you monitor inflammatory markers? Daily?
A: CRP (+/-cytokines) & cardiac biomarker
- severe, non-critical: once per week
- ICU patient: every 2-3 days
- severe critical: daily
A: CRP (+/-cytokines) & cardiac biomarker
- severe, non-critical: once per week
- ICU patient: every 2-3 days
- severe critical: daily
Q: How did you use Steroid Rx?
A:
- Steroids: active debate in our group
- Possible benefit: may help reduce inflammatory storm
- Possible harm: prolong viral shedding, etc
- Not using commonly
A:
- Steroids: active debate in our group
- Possible benefit: may help reduce inflammatory storm
- Possible harm: prolong viral shedding, etc
- Not using commonly













