1/ Why are hypodermic needles and IV catheters referenced by gauge numbers?
And why does the needle diameter get smaller as the gauge number increases?
Let's explore the obscure history of IV sizing in the following #histmed #tweetorial.
And why does the needle diameter get smaller as the gauge number increases?
Let's explore the obscure history of IV sizing in the following #histmed #tweetorial.

2/ The gauge numbers on modern hypodermic needles are adapted from the Birmingham Wire Gauge (BWG), a system developed during the Industrial Revolution in the early 1800s to standardize the British cottage industry of iron and steel wire manufacturing.

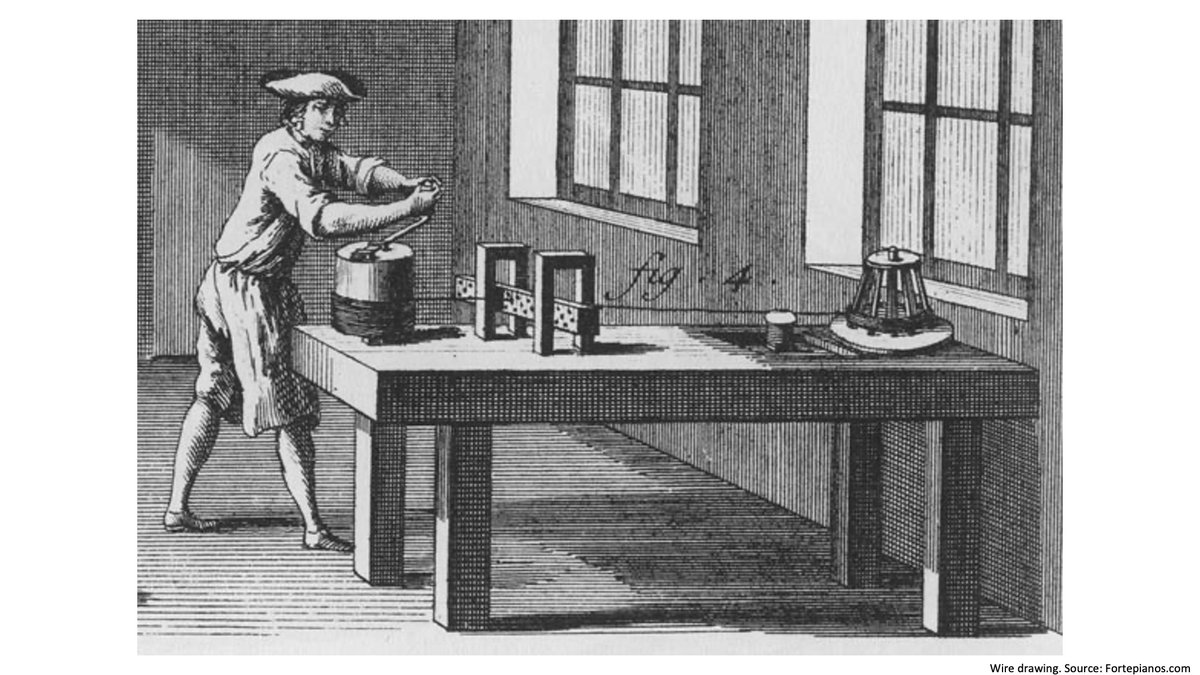
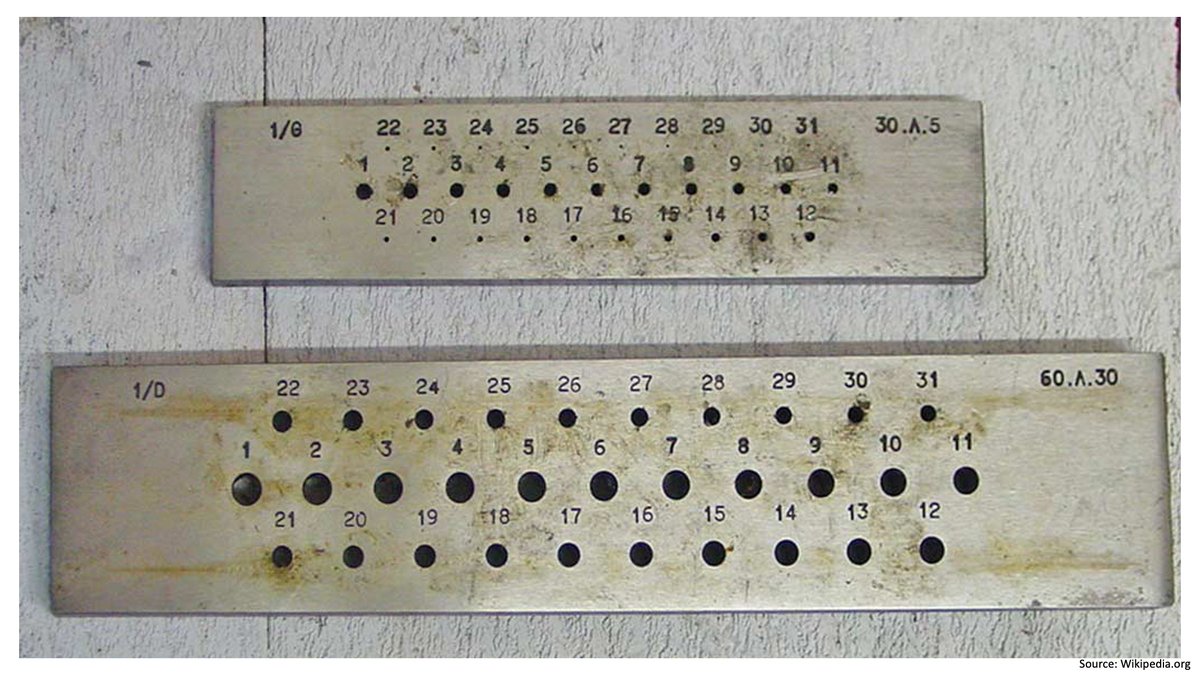
3/ As early as the 1200s wire was made through the process of wire-drawing, which involved pulling iron rods through a conical hole in a draw-plate or gauge.
The resultant wires could then be drawn through successively smaller diameter gauges to produce thinner wire.
The resultant wires could then be drawn through successively smaller diameter gauges to produce thinner wire.
4/ As iron work was a cottage industry, each manufacturer had their own draw-plates and dies which resulted in proprietary wire thicknesses.
These gauges did not represent actual measurements of the wire diameter but rather the number of draw-plates the wire would pass through.
These gauges did not represent actual measurements of the wire diameter but rather the number of draw-plates the wire would pass through.
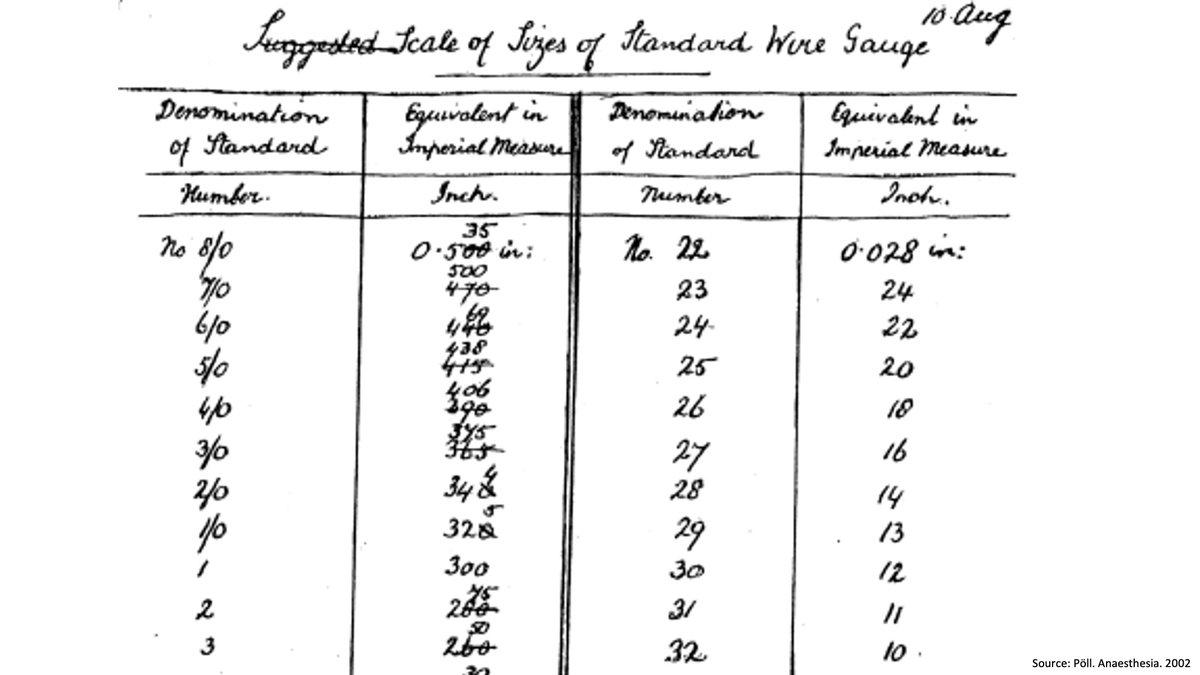
5/ Eventually sophisticated measurement allowed for quantification of existing gauges in 1/1000s of an inch.
Since development of the gauges predated the ability measure in standard units of length, there is no logical or linear progression of measurement between gauge sizes.
Since development of the gauges predated the ability measure in standard units of length, there is no logical or linear progression of measurement between gauge sizes.
6/ Interestingly, while there is no linear progression, there is an exponential decay seen within the Birmingham Wire Gauge as each successive gauge wire is ~11% thinner than the prior gauge number, likely due to the cohesive strength of the iron wire itself.
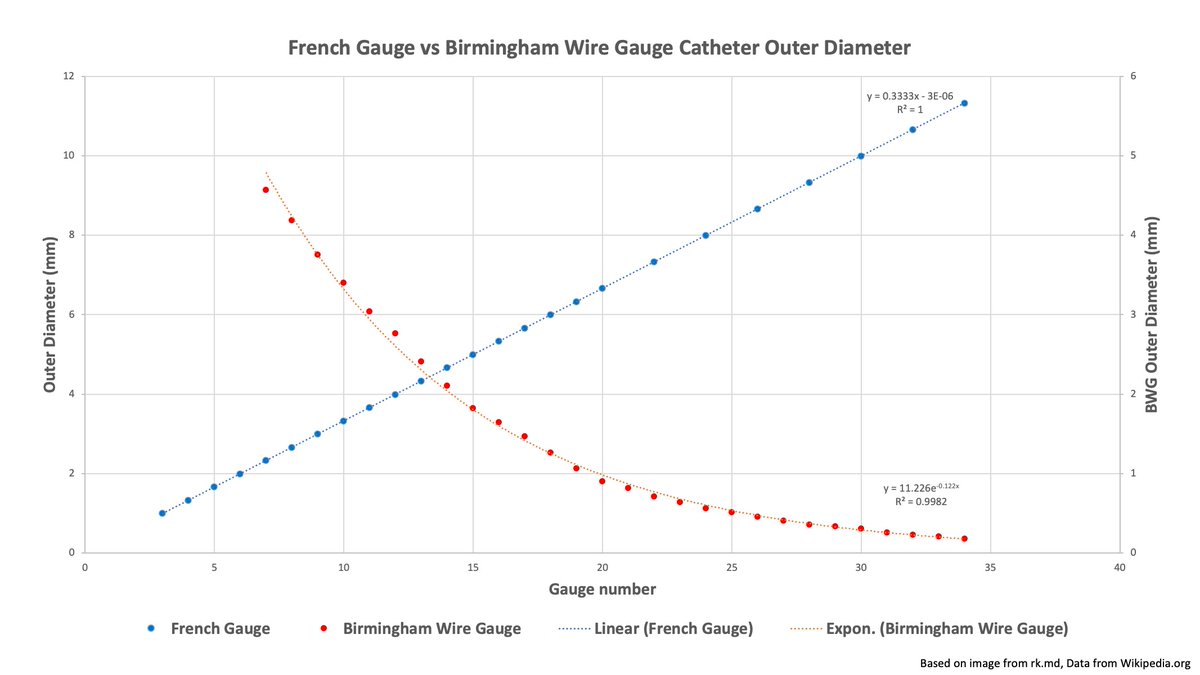
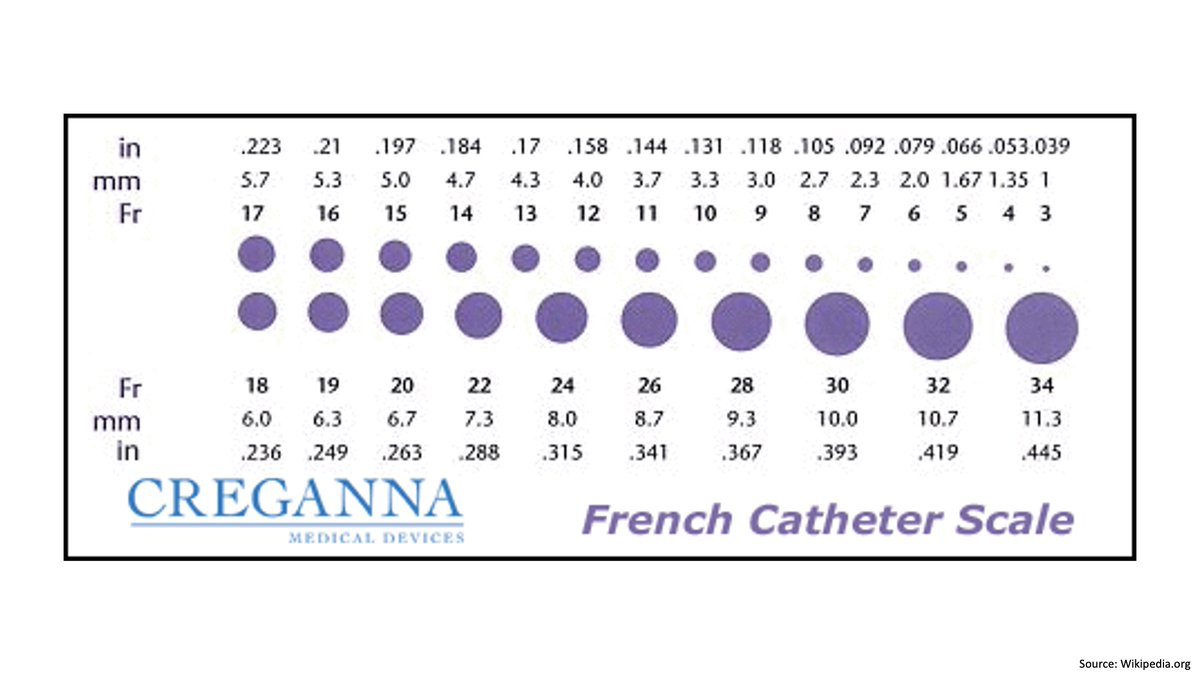
7/ As industrialization increased globally, so did demand for a standard. The British engineering industry would debate several options including switching to a millimeter-based system, like the French gauge (1Fr = 1/3mm), and inventing a new gauge based on the inch.
8/ Ultimately, Queen Victoria would keep the existing BWG as its own standard since it was Imperial, familiar, and easier to say “18 gauge” than “50 thousandths of an inch”.
The BWG was also largely adopted by the USA which soon surpassed the UK in steel manufacturing.
The BWG was also largely adopted by the USA which soon surpassed the UK in steel manufacturing.
9/ Use of the Birmingham Wire Gauge continued into the 20th century and during World War I, the Randall-Faichney Company would become one of the largest producers of hypodermic needles, making the BWG a needle measurement standard we use today.

10/ To summarize:
💉 IV gauges are based on British wire diameters from the 1800s.
💉 ⬆️ gauge number = ⬇️ diameter needles because wire was drawn through progressively smaller dies.
💉 Unlike French gauge which ⬆️ linearly, there is no linear progression of BWG IV gauge sizes.
💉 IV gauges are based on British wire diameters from the 1800s.
💉 ⬆️ gauge number = ⬇️ diameter needles because wire was drawn through progressively smaller dies.
💉 Unlike French gauge which ⬆️ linearly, there is no linear progression of BWG IV gauge sizes.
11/ For further reading, be sure to check out the following articles used as sources for this tweetorial.
🆓 pubmed.ncbi.nlm.nih.gov/10403873/
🔒 pubmed.ncbi.nlm.nih.gov/3295010/
🆓 pubmed.ncbi.nlm.nih.gov/10403873/
🔒 pubmed.ncbi.nlm.nih.gov/3295010/
• • •
Missing some Tweet in this thread? You can try to
force a refresh