
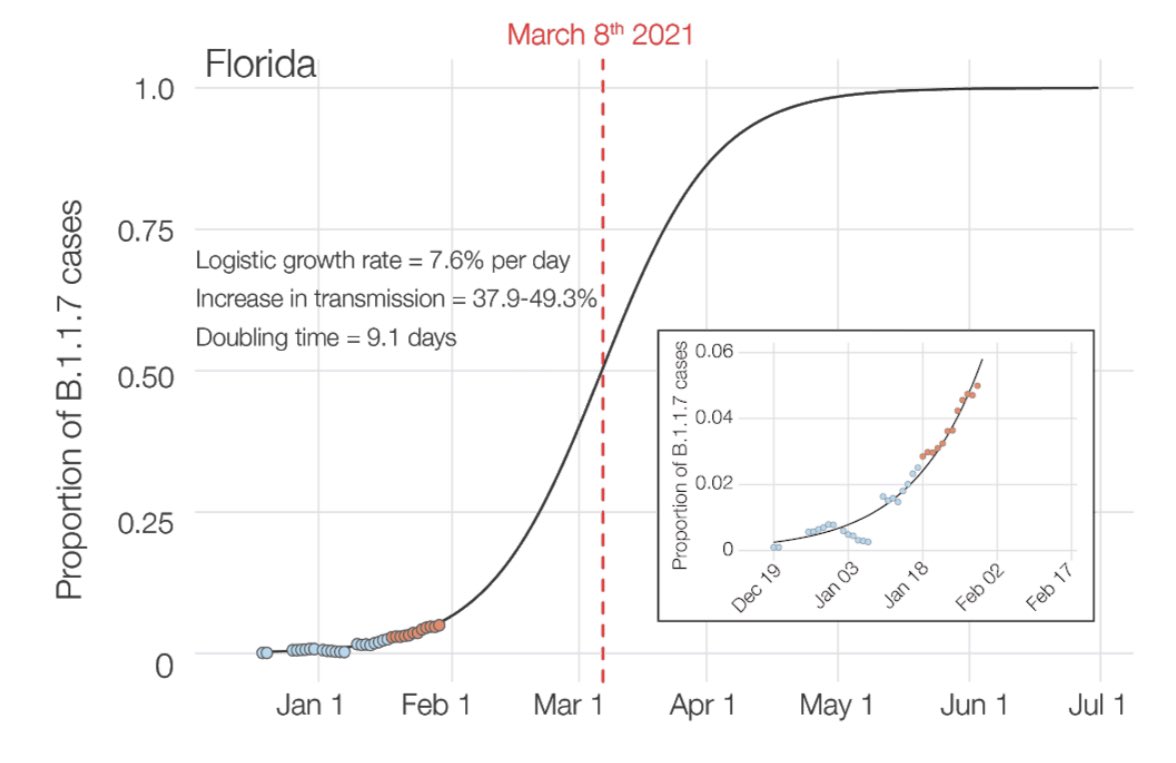
⚠️SURGING #B117 WITHIN US—growing 7% per day, doubling every 9.8 days nationally, & expected to become dominant by March 23rd. It is surging fastest in Florida—doubling every 9.1 days. Scientists are extremely worried: 35-45% more transmissible.🧵#COVID19
washingtonpost.com/health/ukvaria…
washingtonpost.com/health/ukvaria…

2) new preprint, led by @K_G_Andersen, “Our study shows that US is on a similar trajectory as other countries where B.1.1.7 rapidly became the dominant #SARSCoV2 variant, requiring immediate and decisive action to minimize #COVID19 morbidity and mortality” medrxiv.org/content/10.110…
3) Here is the current inferred number of #B117 cases in each state and in Florida and California, to Jan 30th.
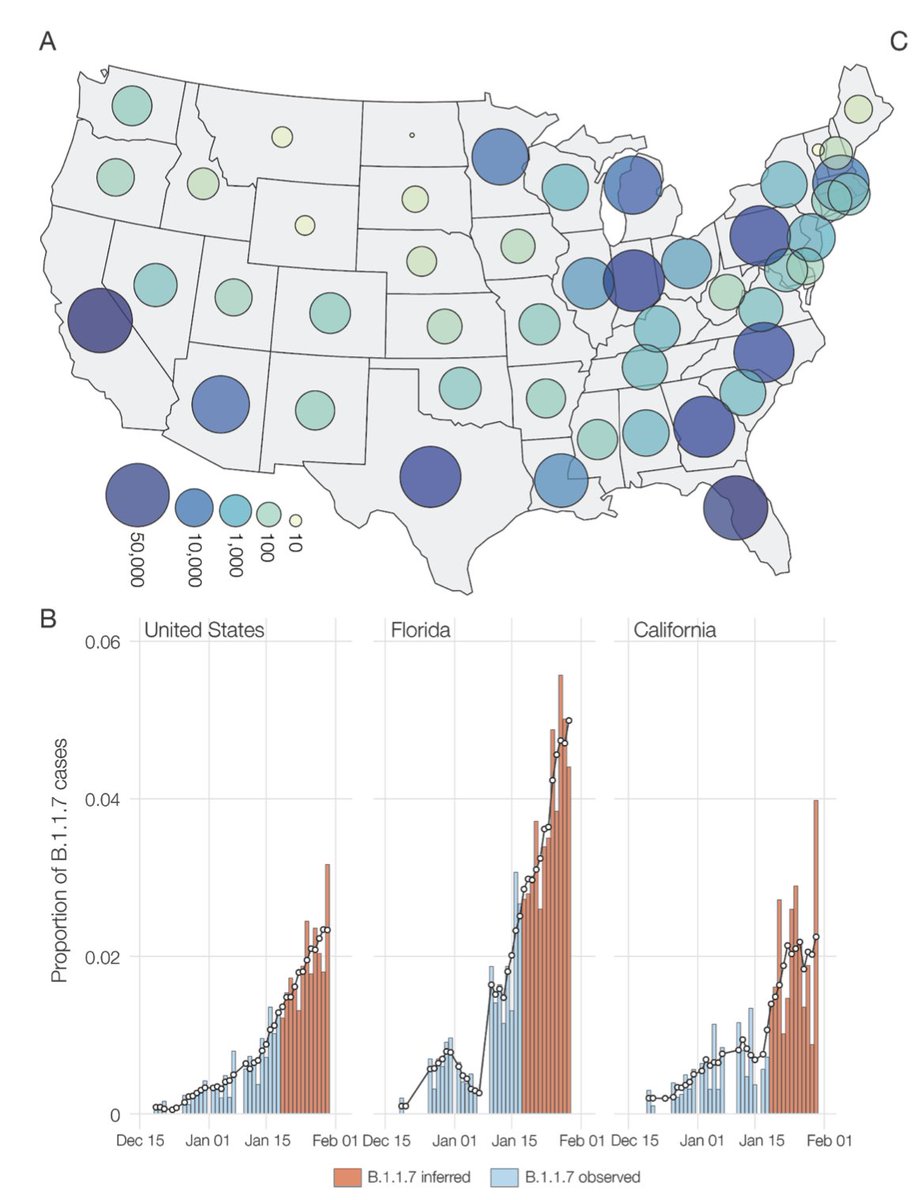
4) Florida seems to be experiencing the faster rate of growth. (Maybe because @RonDeSantisFL @GovRonDeSantis hasn’t put in much mitigation). #B117 will become dominant in Florida sooner... likely by March 8th.
5) Why is #B117 worse than other #SARSCoV2? It carries a package of mutations, including many which change the structure of the spike protein that enhance its ability to bind to human ACE2 receptor, yielding higher viral loads, and may shed more virus when coughing or sneezing.
6) “It is here, it’s got its hooks deep into this country, and it’s on its way to very quickly becoming the dominant lineage,” said Michael Worobey, an evolutionary biologist at the University of Arizona and a co-author of the new paper.
7) other wild cards in play, in the form of additional variants, such as #B1351 from South Africa and worrisome because it contains a mutation (E484K, nicknamed “Eeek”) that lowers but does not entirely undermined the efficacy of vaccines.
8) Will return to Eeek mutation later, but #B117 also led to a super outbreak that infected 10% of an entire Italy 🇮🇹 village in just a few weeks. 140 of 1400 residents. 60% children.
https://twitter.com/drericding/status/1357599530296958982
9) As explained 2 days ago, don’t be deceived that total cases are dropping, there is actually a surging underbelly of #B117 cases that is much much more transmissible and will cause another surge soon in March and April. Please read this 🧵 below.
https://twitter.com/drericding/status/1357566949404905472
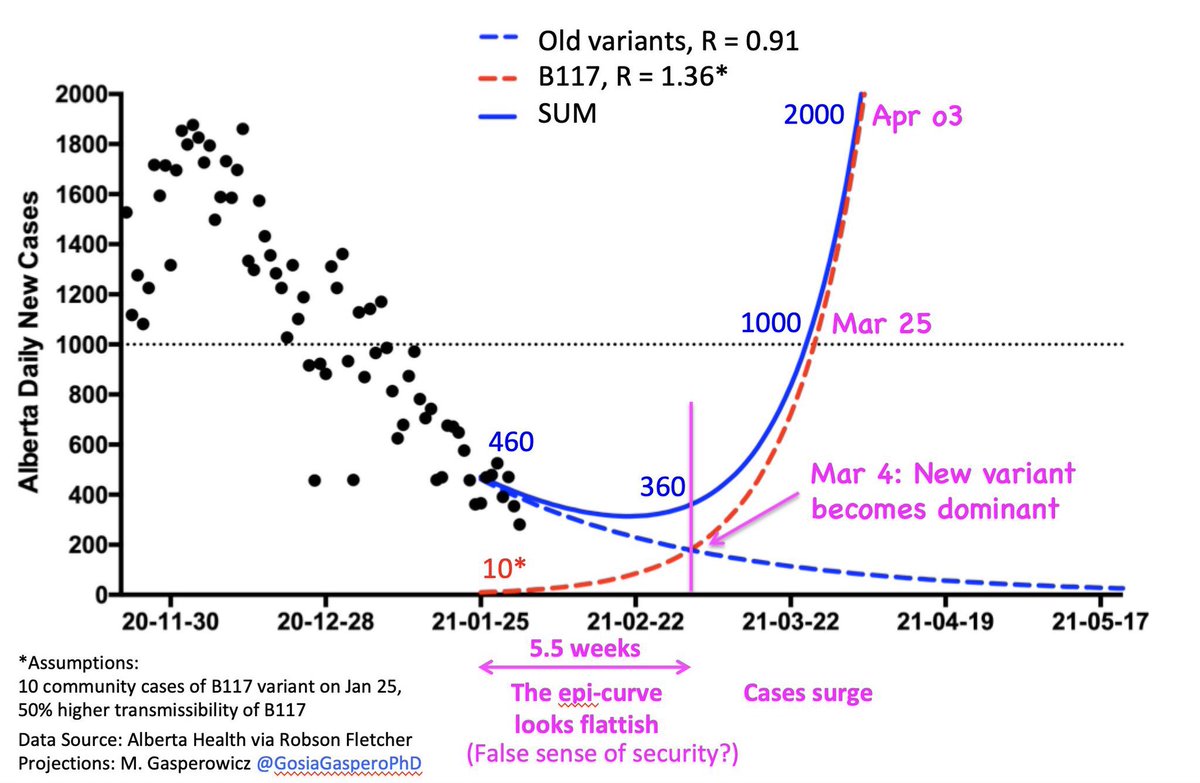
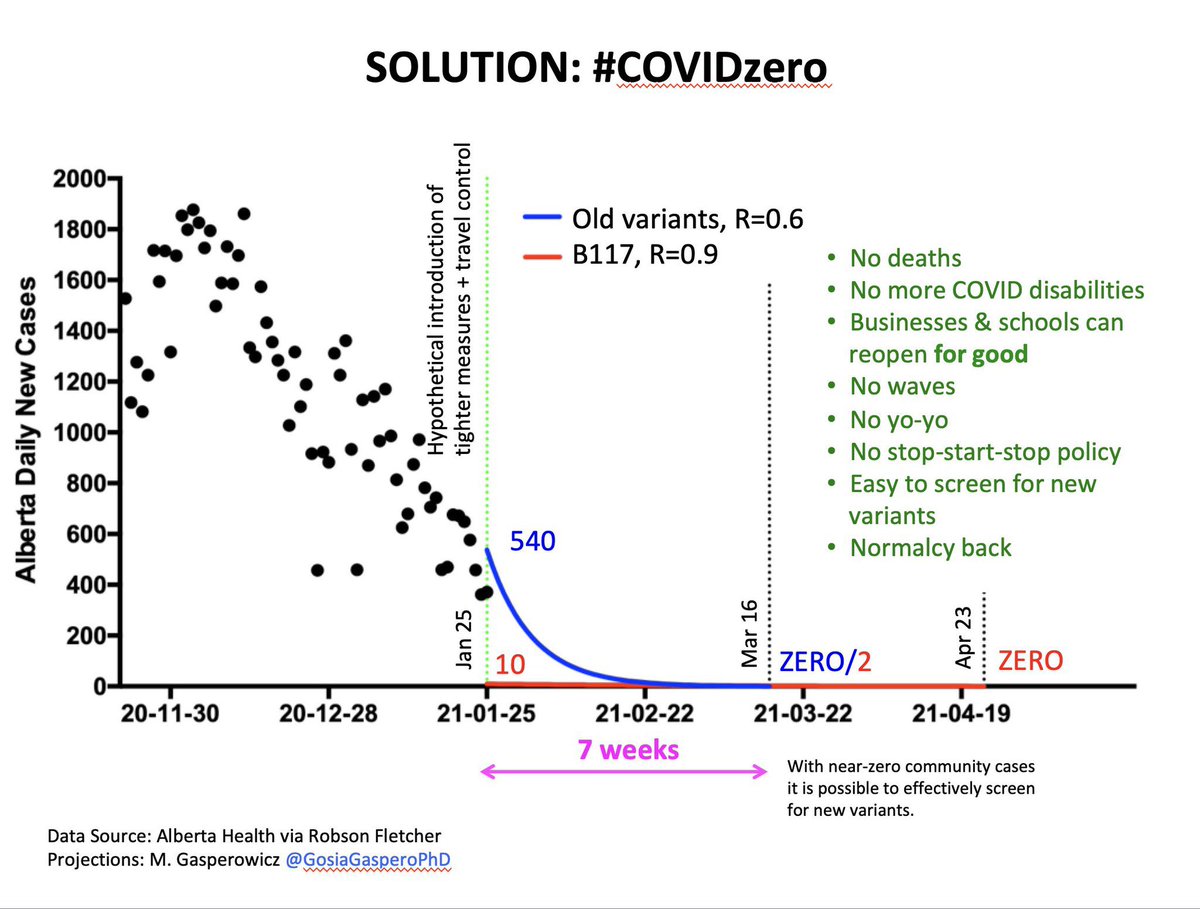
10) Here is what is going to happen... currently R is ~0.9 in many places, but with the more infectious #B117, the R will jump 50% approximately. And it is inevitable (all CDC and Danish models say this) that B117 will take over as the reigning dominant variant soon—Alberta 🇨🇦
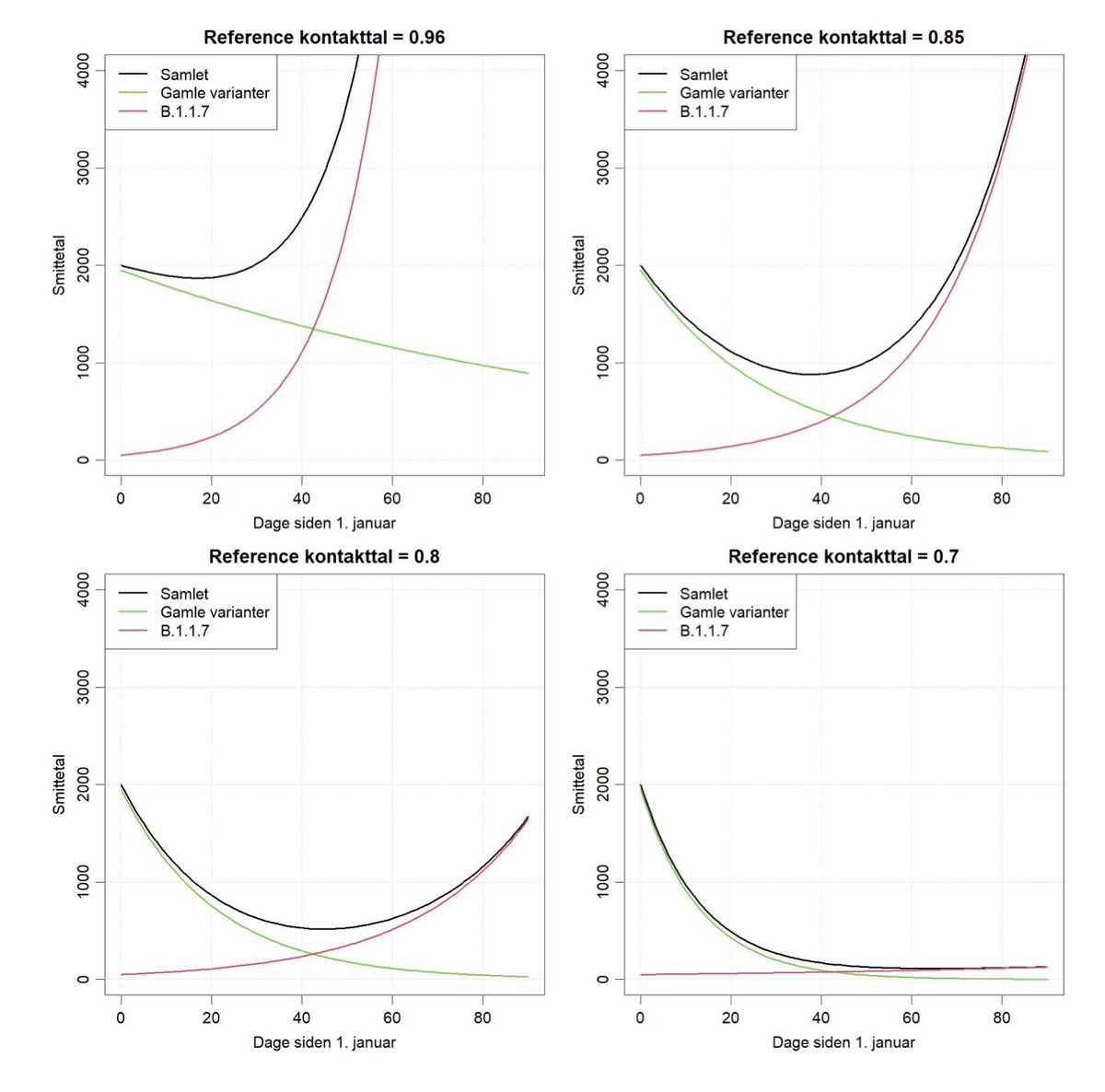
11) Danish models show the same thing. Unless we slam the R current to <0.7, but optimally <0.6 right now, we will be in a world of trouble soon.
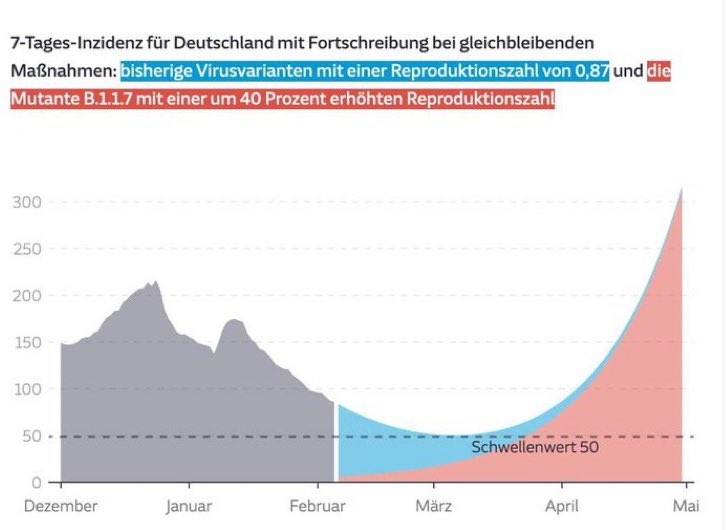
12) And Germany 🇩🇪 also shows the same phenomenon—that #B117 will become the dominant reigning variant (new strain??) and cause a late March / April new surge. Especially if vaccine rollout is slow. sueddeutsche.de/wissen/coronav…
13) The solution to defeating the #B117 is to chase a #ZeroCovid approach and slam the R even lower to below 0.7.... but optimally 0.6 or less. So that even when the #B117 arises, it will keep R under 1 (0.6*1.5=0.9). And by keeping R at 0.6 now—we will have buffer room for B117.
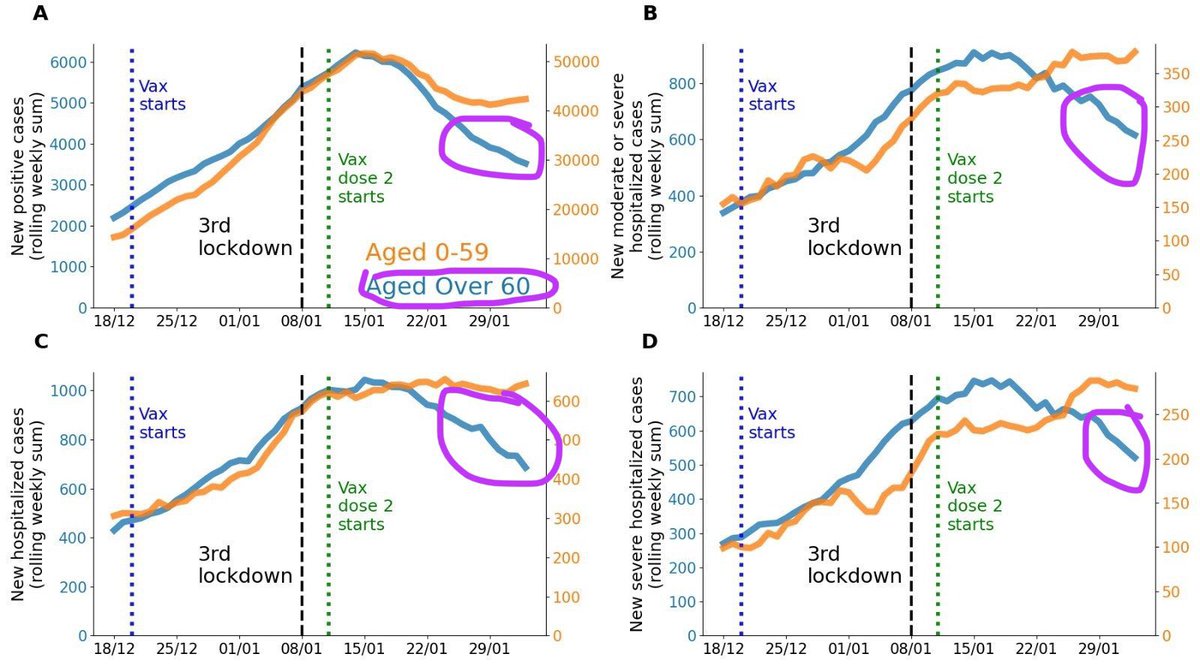
14) other way to win is with fast mass vaccination like in Israel 🇮🇱 that has already vaccinated 60 shot per 100 people in the elderly. Hence now look how fast the cases, hospitalizations are diverging for those age 60+ vs 59 or under. That is the effect of **mass** vaccinations.
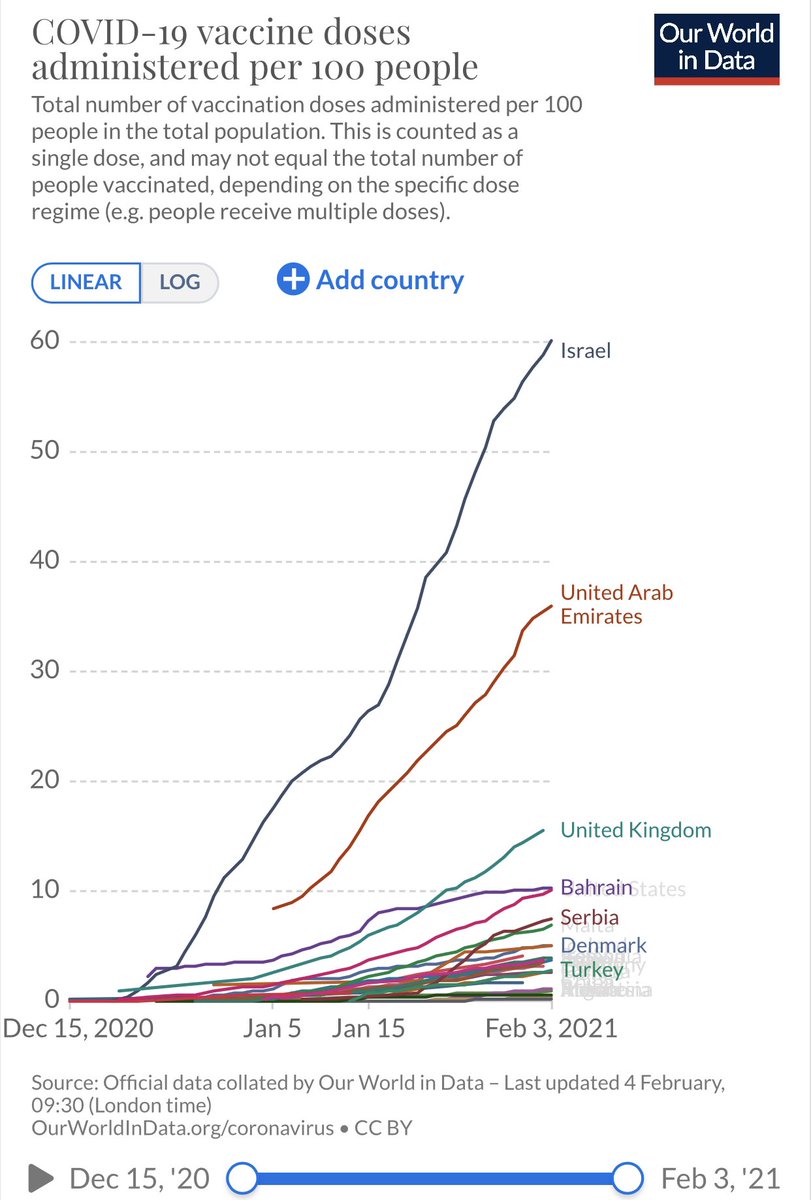
15) Israel with 60 shots per 100 people (note 200 per 100 needed for full coverage, which we can only do when kids vaccine approved) is currently 4x 🇬🇧 and 6x ahead of the US. We need to all get to Israel level vaccinations by March...
16) And vaccines do work well for the general #B117 variant. Just a bit attenuated for South African #B1351 variant that has the E484K “Eeek” mutation. See thread 🧵
https://twitter.com/DrEricDing/status/1353706396282474499
17) ...But we also discovered the #B117 has a sublineage with also the E484K “Eeek” mutation. UK researchers found it in 11 people across England and Wales. And there is some concern about this.
https://twitter.com/drericding/status/1356365178330378251
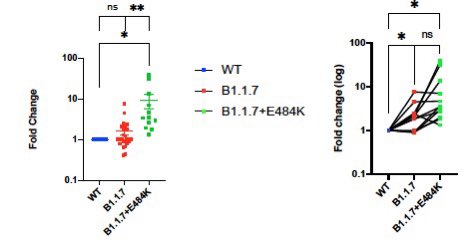
18) So what do we know about the #B117+E484K combo sublineage? Not much except this preprint study showing it is might be more resistant to antibody neutralization (more antibodies needed in lab study to neutralize the pseudovirus) than the common strain and the regular B117.
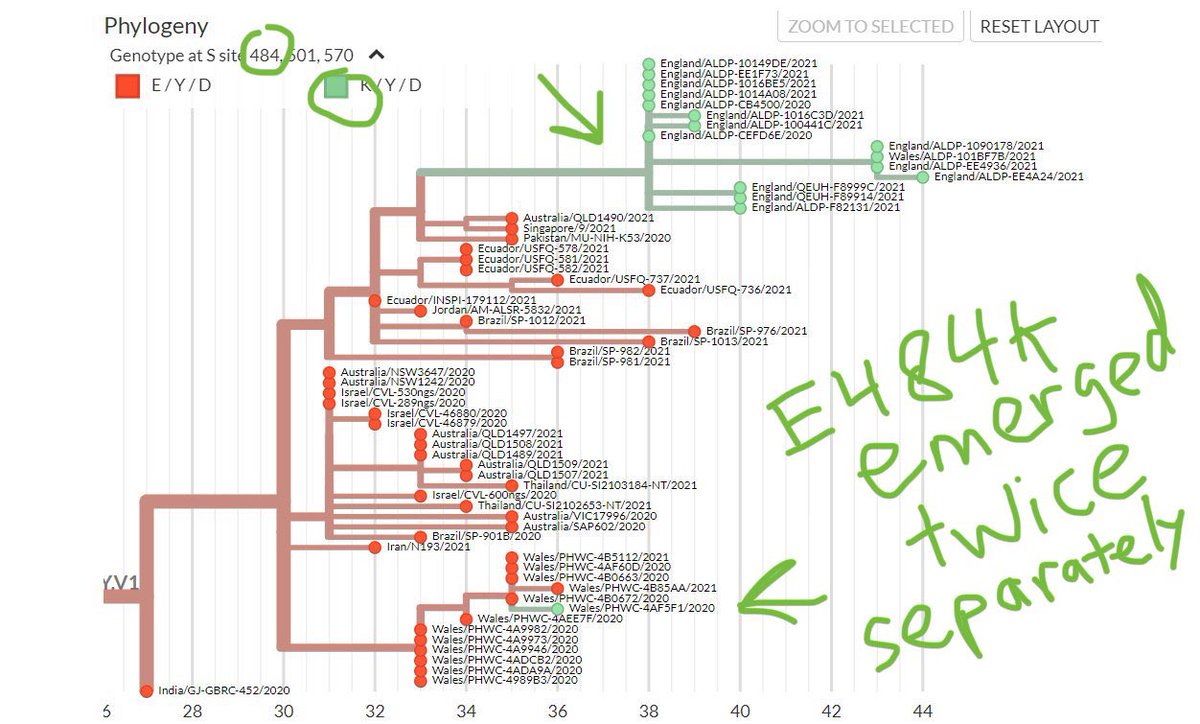
19) We don’t know about vaccine resistance yet, but could #B117+E484K be bad? it emerged in UK twice—independently arising in Wales, and in England, plus in 🇧🇷 & 🇿🇦—so 4 times means convergent evolution is real. And convergent evolution is usually always greater survival fitness.
20) #B117 is becoming a beast. Israel is seeing a sharp rise in the number of children and teens getting infected with #COVID19. “This is something we did not witness in previous waves,” Health Minister Yuli Edelstein said. Some think it’s due to B117. jpost.com/health-science…
21) More than 50,000 🇮🇱 children and teens have gotten #COVID19 since the start of Jan, many more than in any month during 1st/2nd waves.
“We got a letter from the Israeli Association of Pediatrics that says they are very worried about the rate of disease in younger students”
“We got a letter from the Israeli Association of Pediatrics that says they are very worried about the rate of disease in younger students”
22) “one hypothesis is that it is tied to 🇬🇧#B117 mutation, which has spread rapidly across Israel.”
“The British variant is more contagious, so it increases the chances of infection in children,” Cyrille Cohen, head of Bar-Ilan University’s immunotherapy laboratory, told JPost.
“The British variant is more contagious, so it increases the chances of infection in children,” Cyrille Cohen, head of Bar-Ilan University’s immunotherapy laboratory, told JPost.
23) We might end up back at square one if we don’t stop these mutants. It was just discovered this week that the #B1351 variant with the Eeek mutation is so evasive —people with prior #COVID19 has no extra protection against this variant —not even for severe reinfection!! See 🧵
https://twitter.com/drericding/status/1358065355785134083
24) BOTTOMLINE: “We have to be concerned about the mutants”.
Fauci is right about the concern of #B117, #B1351, #P1.
We gotta end pandemic fast with vaccines and #ZeroCovid approach, or else we will be back to square one again. Another wave is brewing.
Fauci is right about the concern of #B117, #B1351, #P1.
We gotta end pandemic fast with vaccines and #ZeroCovid approach, or else we will be back to square one again. Another wave is brewing.
25) Summary of the vaccines and their efficacy and also for the mutations.
https://twitter.com/drericding/status/1358757953772355585
• • •
Missing some Tweet in this thread? You can try to
force a refresh




















