Normally I enjoy the high standards of journalism in @guardian . Not today as disappointed with misleading headline that suggest infections are spreading fastest in children. It'll worry parents/teachers & I doubt most readers will unpick the headline.
1/
theguardian.com/world/2021/feb…
1/
theguardian.com/world/2021/feb…
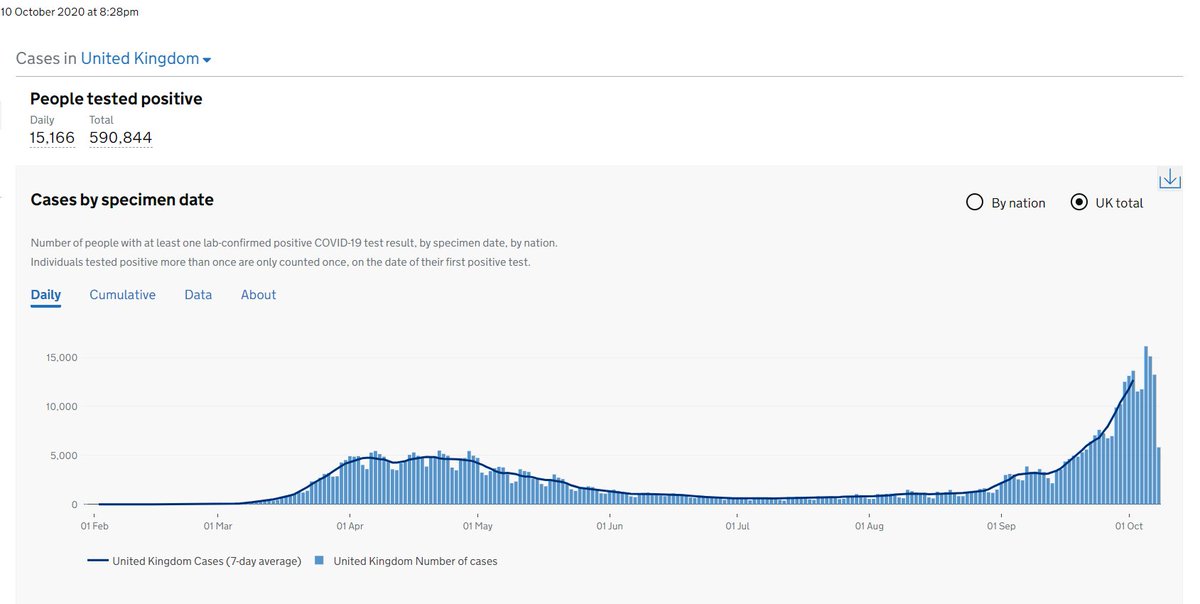
The latest REACT1 report shows prevalence of infection in ALL age groups has fallen, including children aged 5-12 from 1.59% in Round 8 to 0.86% in Round 9a. The authors of REACT1 report also (wisely) didn't try to interpret the prevalence figures.
2/
spiral.imperial.ac.uk/bitstream/1004…
2/
spiral.imperial.ac.uk/bitstream/1004…
If this were a research trial you wouldn't place much weight on the age differences in % prevalence because of the wide confidence intervals, i.e. differences weren't statistically significant.
3/
3/
I've previously tweeted on the challenges (& dangers) of interpreting surveillance data. One would need lots more contextual info to make sense of it & arrive at sound conclusions.
4/
4/
https://twitter.com/andrewleedr/status/1360970602216108033
Undoubtedly some will extrapolate from the prevalence of infection figures in children to other settings i.e. schools based on the headline. I'd advise caution as there is a real risk of over-interpretation through extrapolation of limited data. Association is not causation.
5/
5/
What REACT1 can’t tell us is how infectious children are or how much child infections drive the pandemic. Finding viral RNA on PCR from a child tells you nothing about how much virus they are shedding. Neither can it tell you the direction of transmisison (who infected who).
6/
6/
Those of us in public health are well familiar with Bradford Hill criteria for causation that outlines key factors to consider. It would make sense to apply this approach to this issue.
7/
7/

Is there CONSISTENCY? What’s been reported has been mixed, but @ECDC_EU , @CDCgov , @RCPCHtweets & other expert review groups have concluded the balance of evidence suggests kids aren't key transmitters of infection.
8/
https://twitter.com/CDCDirector/status/1361079524587425793
https://twitter.com/DocJeffD/status/1353149487414439937
8/
Is the SPECIFICITY of the association or are there other confounders? Indeed the REACT1 report clearly show there are multiple other drivers such as deprivation & household size, etc...
9/
9/
What about TEMPORAL SEQUENCE, i.e. does a rise in school outbreaks then follow a rise in community outbreaks? We aren’t seeing that.
10/
https://twitter.com/andrewleedr/status/1358841129119137792
10/
For me what also matters is PLAUSIBILITY & COHERENCE with what is known about the natural history and biology of the disease. Studies have shown that kids, being smaller, produce far fewer aerosols than adults. They also shed less virus than others.
11/
https://twitter.com/andrewleedr/status/1360652991481720842
11/
And also
And we know symptomatic persons shed more virus. So it follows that an adult is more likely to infect a child than the other way.
medrxiv.org/content/10.110…
12/
https://twitter.com/andrewleedr/status/1356909767197941760
https://twitter.com/andrewleedr/status/1356910942257352706
And we know symptomatic persons shed more virus. So it follows that an adult is more likely to infect a child than the other way.
medrxiv.org/content/10.110…
12/
This isn't to say that infections from children to adults don’t happen. Of course they do, but at much lower levels than the other way around. We mustn't lose sight of the fact that adults still account for the bulk of infections.
13/
13/
We know that of all settings, household transmission is the highest risk. If infection is introduced into the household the majority of household members are likely to get infected. Community transmission matters.
14/
https://twitter.com/CT_Bergstrom/status/1360339751933366276
https://twitter.com/andrewleedr/status/1357623142060032003
14/
This in no way refutes need for public health measures in schools to reduce risks of infection. Yes precautionary principle is important but need to balance both benefits & harms. Measures must be proportionate to actual (rather than perceived) risk.
15/
https://twitter.com/apsmunro/status/1362446759545495554
15/
See also @apsmunro's excellent thread that outlines the evidence base.
https://twitter.com/apsmunro/status/1362446759545495554
• • •
Missing some Tweet in this thread? You can try to
force a refresh