In the past 15+ yrs I've worked as a GP in some of the poorest parts of Sheffield with all the social ills of poverty: debts, joblessness/job insecurity, crime, abuse, domestic violence, mental ill health, disrupted lives, chronic diseases, alcoholism, early deaths, etc... 1/
For many of my patients, poverty isn't an abstract concept you read about. It's their lived experience. It's real. It's pervasive. It wears you down. It kills your hopes & dreams. And they're trapped in a repeating cycle across generations. 2/
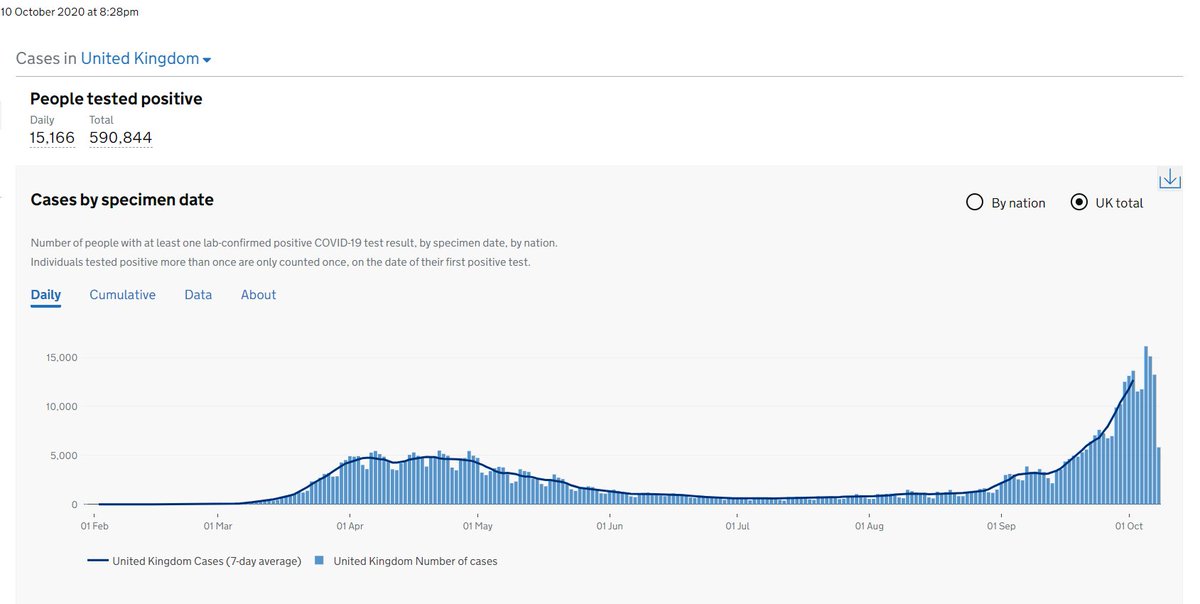
COVID has been really bad for them. Difficult to lockdown in rubbish housing, little greenspace, nowhere to go, nothing to do. Having debts & insecure work forces you to work. I feel most for the kids, many who went to school with my kids, but lack the opportunities mine have. 3/
Education is a key to better life opportunities for them & better lives. But even that's now denied. How do you home school/learn at home if you have no wifi/laptop, squashed with others in a 2 room terrace, with minimal teacher input? 4/
Many have missed so much school this year & probably only been in 2-3 months out of 12. The loss of learning will scar this generation, & these disadvantaged families, & their future families, for generations to come. This is real, not imagined. 5/
I'm disappointed by those who clamour for school closures on flimsy evidence. Yes the evidence isn't perfect, but it is good enough to know nurseries & primary schools can be run fairly safely. No zero risk solution. Let's not lose sight of the kids in all of this.
• • •
Missing some Tweet in this thread? You can try to
force a refresh