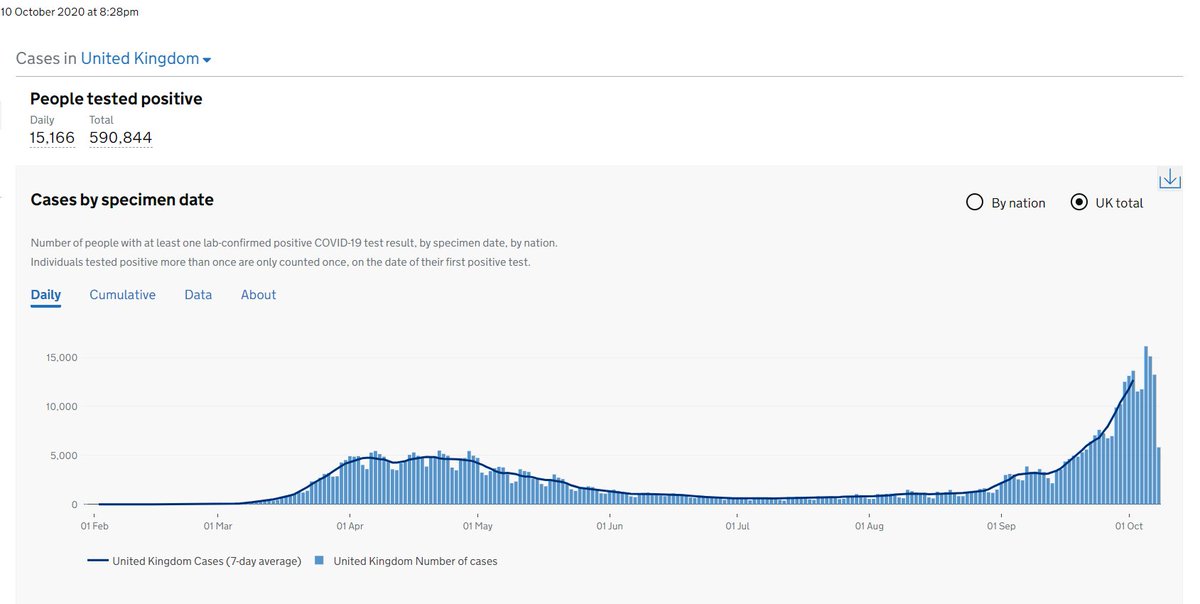
The number of COVID19 cases in UK continues to rise, with a trajectory that is worryingly becoming steeper. Hospitalisations up. ICU admissions up. Community transmission & outbreaks widespread. Clearly control of the epidemic in the UK is deteriorating. Deaths will follow.
1/
1/
Worth revisiting @acmedsci 's report in July for their predictions. acmedsci.ac.uk/file-download/…
Their predicted real worst case scenario is looking more likely.
Give or take a few weeks, we're in for a difficult winter. What's less clear is just how bad is going to get...
2/
Their predicted real worst case scenario is looking more likely.
Give or take a few weeks, we're in for a difficult winter. What's less clear is just how bad is going to get...
2/

The UK gov has thrown £billions at the problem, hired loads of private consultants & consultancy firms, been given lots of good scientific advice, done national lockdown plus local variants of lockdown lite. Yet it's not working.
3/
3/
Loads of opinions out there as to why our efforts aren't working. Frankly dangerous idea out there too about "letting it rip" & going for herd immunity. Pandemic fatigue setting in. If tighter control measures fail, few options left but another damaging national lockdown.
4/
4/
I think there's been a crucial weakness all along in our approach. It's not the lack of scientific advice but the technical expertise & experience of communicable disease control. This is something @doctorshaib has oft repeated & I agree.
5/
5/
Technical expertise is undervalued, a poor relation to science. But technical experts know how to translate science into action, understand realities on the ground & the detail needed to turn ideas into reality. Without them, science & policy intent are just wishful thinking.
6/
6/
That's why we need our jobbing public health folk, senior health managers & civil servants, the apparatus that makes it happen. Crucially, they can tell if an idea is undoable. Outsourcing to private firms isn't the solution as they often lack that technical expertise.
7/
7/
At regional emergency planning level, we have Scientific & Technical Advisory Cells (STACs). But this isn't replicated at higher decision making level. So what seems to be lacking is that operational nous. Diversity of expertise is needed as you don't know what you don't know.
• • •
Missing some Tweet in this thread? You can try to
force a refresh