THREAD ON LONG COVID & KIDS:
TLDR: I don't think we should ignore it.
ONS Infection survey updated its estimates for Long Covid a couple of weeks ago.
assets.publishing.service.gov.uk/government/upl…
TLDR: I don't think we should ignore it.
ONS Infection survey updated its estimates for Long Covid a couple of weeks ago.
assets.publishing.service.gov.uk/government/upl…
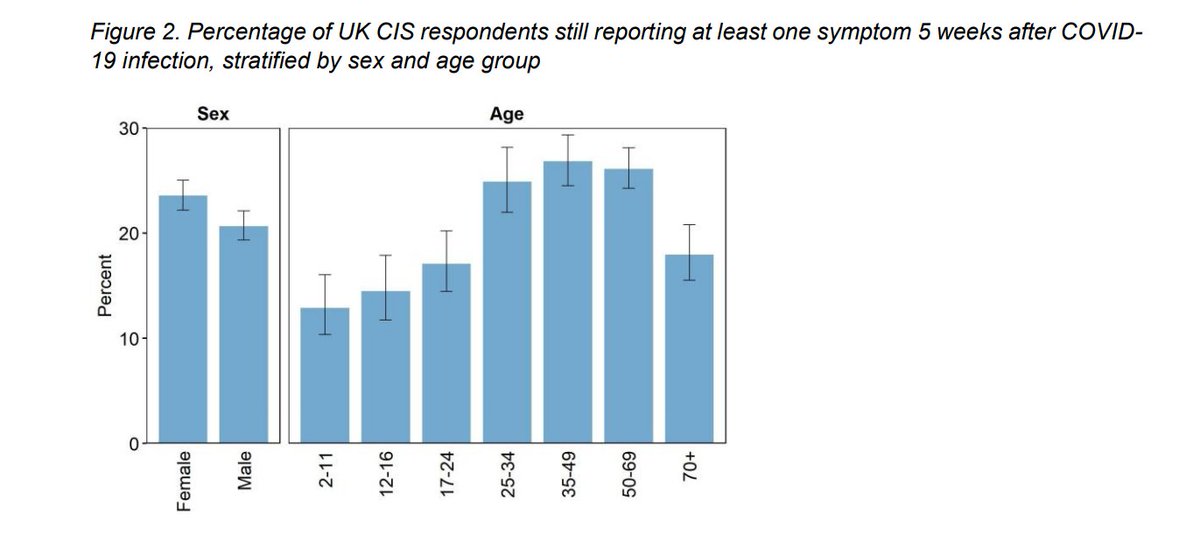
It showed that 13% of under 11's and about 15% of 12-16 yr olds reported at least one symptom 5 weeks after confirmed Covid-19 infection.
ONS samples households randomly - so positive cases do not depend on having had symptoms & being tested.
ONS samples households randomly - so positive cases do not depend on having had symptoms & being tested.
Many have criticised this data because there is no comparator group of kids who had *not* tested positive for Covid and because some of the symptoms are common in childhood. (e.g. fever, cough)
These are perfectly valid criticisms and ideally we would have that.
BUT
These are perfectly valid criticisms and ideally we would have that.
BUT
ONS asks people *every week* for first 4 weeks and then every month after that. They measure duration of symptoms until *first* contact with no reported symptoms after first positive test. This reduces the chance that people are just reporting new colds etc for their kids...
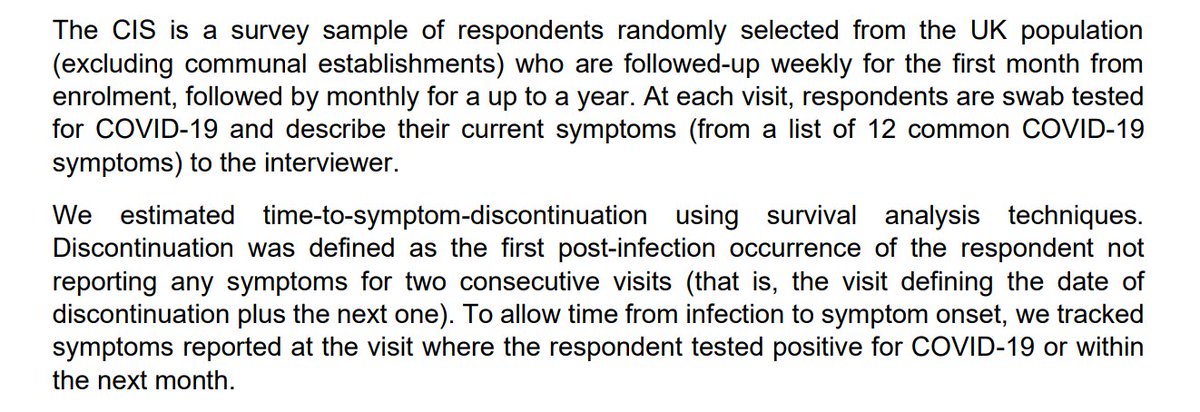
But it is of course still possible. ONS lists the biases in the survey currently and some act to underestimate how common long covid is ("Downwards") and some act to overestimate it ("Upwards").

Another (not yet peer reviewed) study from Italy, specifically looking at long covid in kids, was published this week.
medrxiv.org/content/10.110…
medrxiv.org/content/10.110…
It was based on 129 children diagnosed with Covid between March and Nov. 5% of the kids were hospitalised with Covid and 75% had had symptoms.
Parents were asked about *persisting* symptoms using the ISARIC Long Covid survey. The avg time after diagnosis was about 5 months.
Parents were asked about *persisting* symptoms using the ISARIC Long Covid survey. The avg time after diagnosis was about 5 months.

35% of children still had 1 or 2 symptoms and 22.5% still had 3 or more symptoms. Overall 57% still had at least 1 symptom!
This table gives the breakdown by persisting symptom and severity of initial illness.
This table gives the breakdown by persisting symptom and severity of initial illness.

Also, for 35% of children, parents reported that the ongoing symptoms distress the child a little or quite a lot (11% said quite a lot).
Now this is a study based on kids diagnosed in a clinical setting (I think) and is only a small sample (unlike ONS) - so it's not clear how it would translate to the general population. It also doesn't have a control group which the authors acknowledge as a key limitation.
So what does this all mean? Well none of it conclusive. But it's becoming increasingly clear that long covid in adults is a real and serious problem. thelancet.com/journals/ebiom…
ONS in tweet 2 suggests (unsurprisingly) that is less common in kids than in adults. BUT NOT uncommon.
ONS in tweet 2 suggests (unsurprisingly) that is less common in kids than in adults. BUT NOT uncommon.
*Even if* ONS survey overestimates persistent covid symptoms in kids by a factor of 2 or 3, that is still thousands of kids since we know prevalence of infection has been higher among school age kids than general pop when covid common & schools open.

While our vaccination programme is rapidly vaccinating millions of adults, there is no licenced vaccine for kids & won't be until probably end 2021 /early 2022.
Yes the evidence of long covid in kids is uncertain, there is so much we don't know, not least actual impact.
BUT
Yes the evidence of long covid in kids is uncertain, there is so much we don't know, not least actual impact.
BUT
As Rutter & @trishgreenhalgh said in this great BMJ piece bmj.com/content/370/bm… "Consider carefully whether to wait for definitive evidence or act on the evidence you have."
Consequences of being wrong about long covid in kids are huge *if* we let covid spread through kids.
Consequences of being wrong about long covid in kids are huge *if* we let covid spread through kids.
So are the consequences of keeping schools shut long term.
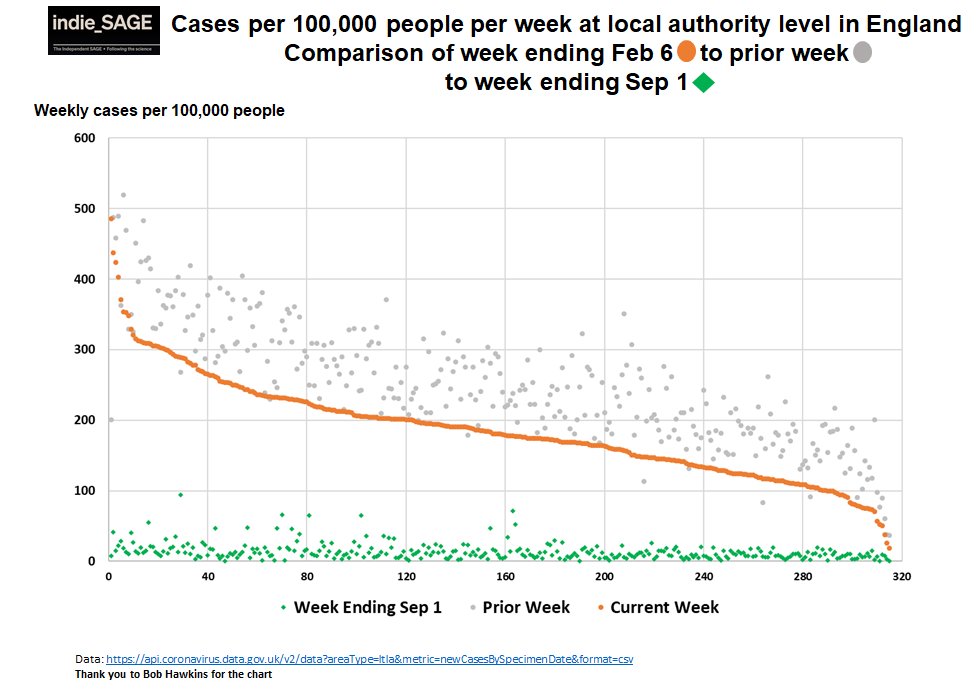
But we *can* do all we can do make schools as safe as possible AND drive transmission very low in communities (lower than 10 cases / 100K people / week) and so minimise the number of cases in kids (and everyone!)
But we *can* do all we can do make schools as safe as possible AND drive transmission very low in communities (lower than 10 cases / 100K people / week) and so minimise the number of cases in kids (and everyone!)
I believe this is the precautionary approach.
We *can* do it - all UK nations got to lower than that last summer. Vaccination of adults will make it easier.
It *will* mean keeping in many restrictions for longer to get cases below that threshold to protect schools & kids. END
We *can* do it - all UK nations got to lower than that last summer. Vaccination of adults will make it easier.
It *will* mean keeping in many restrictions for longer to get cases below that threshold to protect schools & kids. END
• • •
Missing some Tweet in this thread? You can try to
force a refresh