1. LONG THREAD ON COVID, LOCKDOWN & THE ROADMAP:
TLDR: There’s a lot to like about the roadmap – but it could be & should be made much more effective.
Because this will be tying current situation to the roadmap, I’m concentrating on English data
Read on… (22 tweets - sorry)
TLDR: There’s a lot to like about the roadmap – but it could be & should be made much more effective.
Because this will be tying current situation to the roadmap, I’m concentrating on English data
Read on… (22 tweets - sorry)
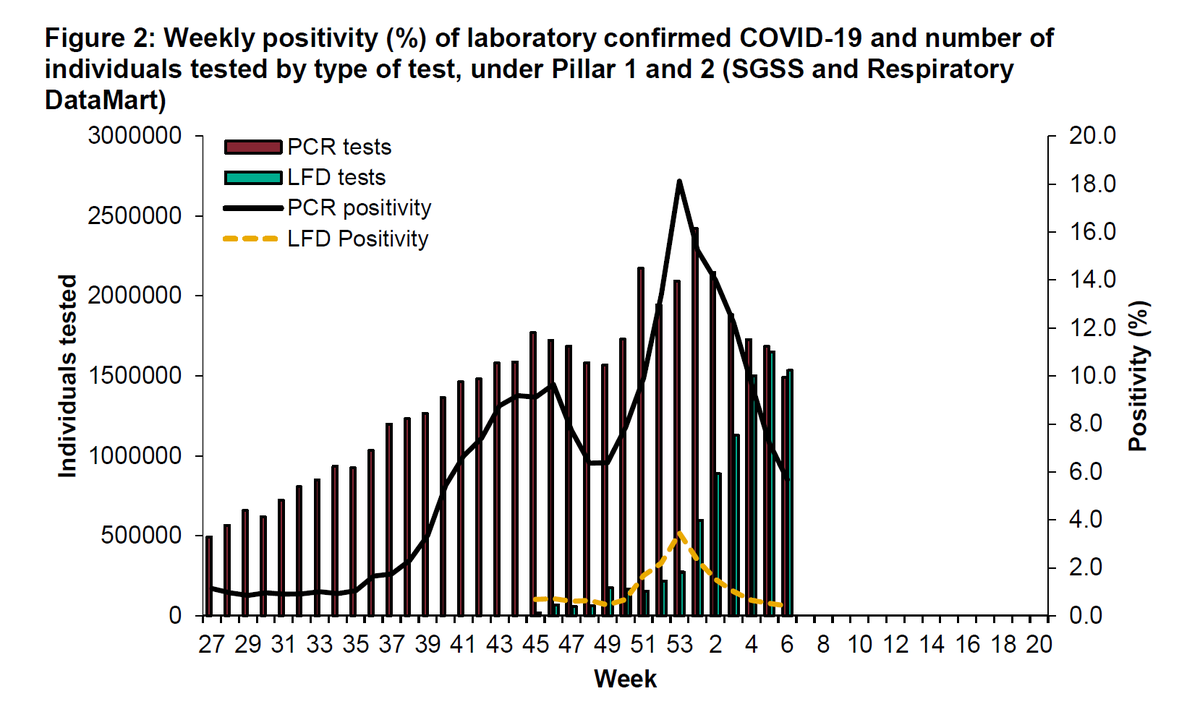
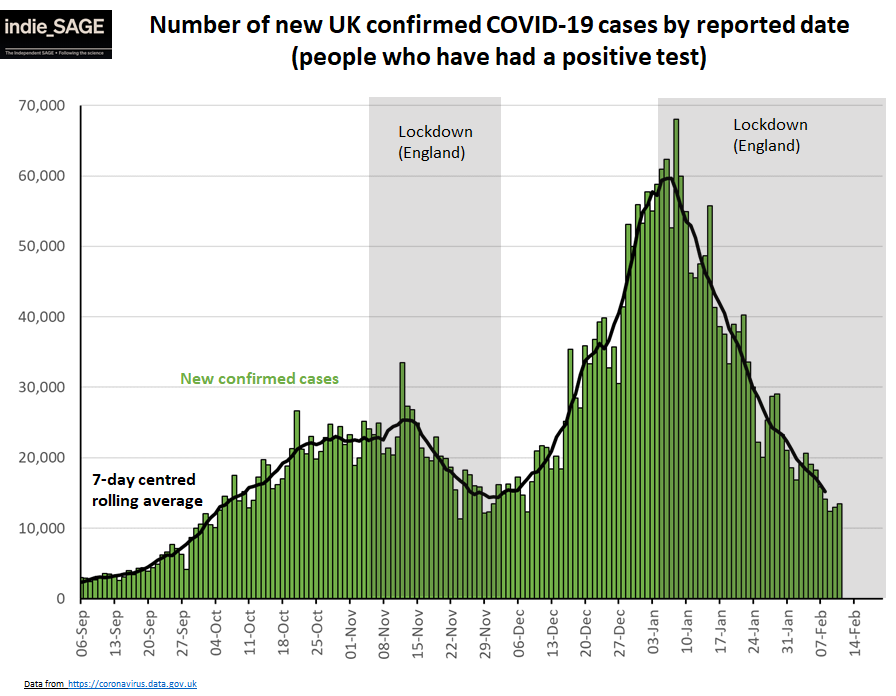
2. Firstly, cases across England are falling. This is good news but the pace of reduction is slowing.
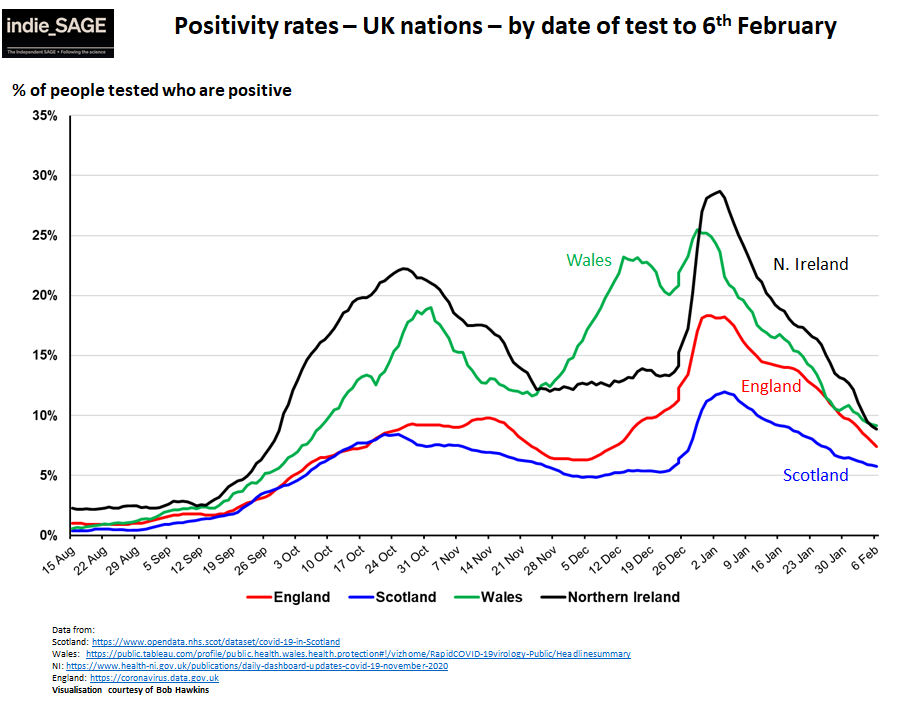
England has the highest case rate in the UK and the nations with lower case rates (on the order of 100 cases/100,000 pop/week) are plateauing even more
England has the highest case rate in the UK and the nations with lower case rates (on the order of 100 cases/100,000 pop/week) are plateauing even more


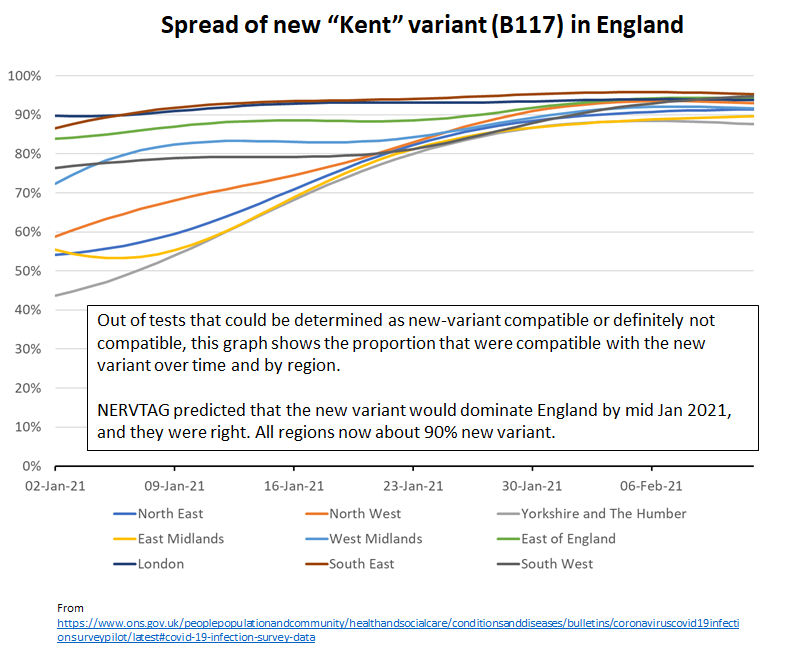
3. The worry is that the more transmissible new strain + many people still out at work, often in non-Covid safe workplaces, means it might be hard to get much below 100/100K/wk , esp in deprived areas, even under current restrictions.
The new strain now dominant everywhere.
The new strain now dominant everywhere.
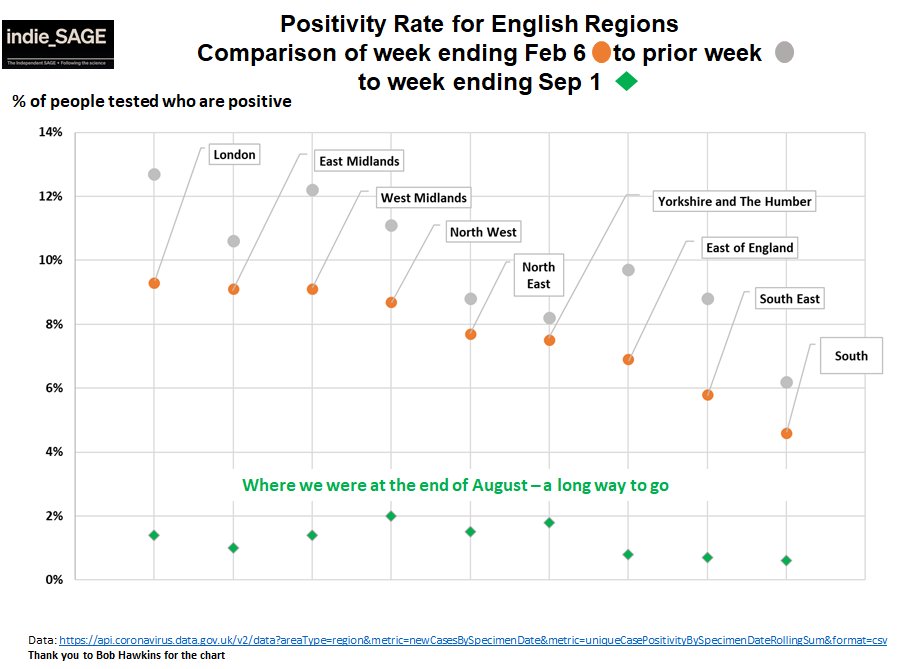
4. Regionally in England, we are starting to see gaps open up, with the North and Midlands having the highest rates again and slower reduction compared to London and SE.
The north of England also now has highest rate of hospital admissions.
The north of England also now has highest rate of hospital admissions.

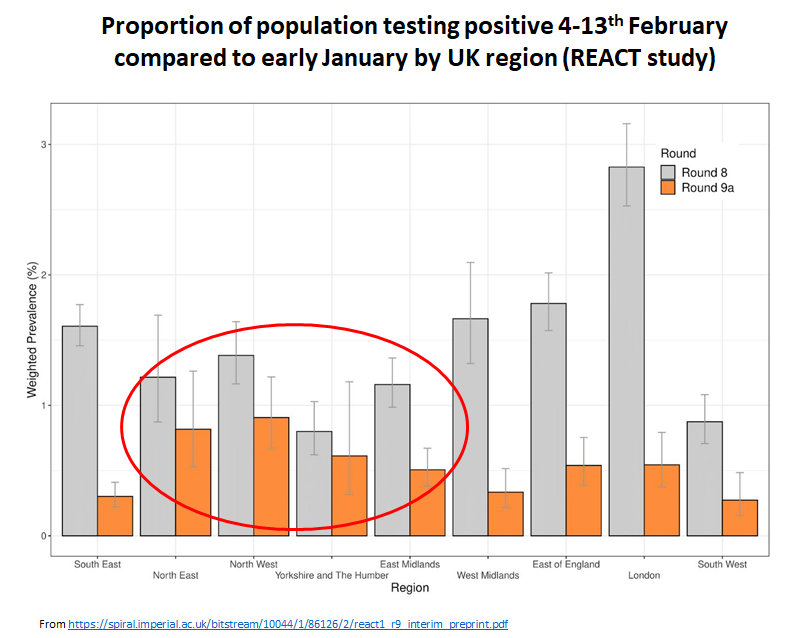

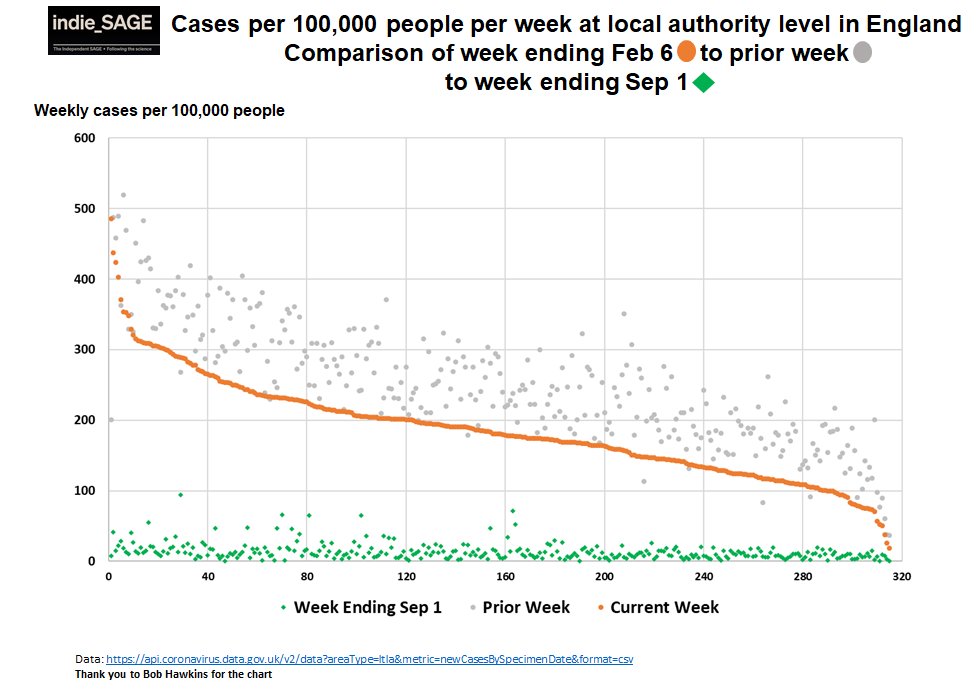
5. We had a similar situation last summer and autumn where it proved really hard to get cases down in many deprived communities.
SAGE said that poorer communities were hit with a perfect storm in Covid. REACT showed differences by deprivation had worsened since early Jan.
SAGE said that poorer communities were hit with a perfect storm in Covid. REACT showed differences by deprivation had worsened since early Jan.

6. We see the same pattern in confirmed cases. Using local level deprivation scores kindly provided by @thomasforth, Bob Hawkins charted cases by deprivation.
The gap by deprivation level widens under lockdown. People are out at work, in poor housing, cannot afford to isolate.
The gap by deprivation level widens under lockdown. People are out at work, in poor housing, cannot afford to isolate.


7. We also know that more deprived areas are lagging in receiving the vaccine. So for instance while overall more than 93% of over 80’s have been vaccinated, it’s only 73% in East London.
See also
See also
https://twitter.com/lewis_goodall/status/1362920623924731904?s=20

8. Basically, lockdowns work best for people who can actually lock down.
To drive cases down *everywhere*, you need to address pockets of high cases in more deprived areas. Failure to do so last year resulted in more spread once we opened & local (finally national) lockdowns.
To drive cases down *everywhere*, you need to address pockets of high cases in more deprived areas. Failure to do so last year resulted in more spread once we opened & local (finally national) lockdowns.
9. Supporting people to isolate financially & practically is crucial. Supporting business to create safer workspaces is crucial. Supporting communities to increase vaccine uptake is crucial. The roadmap goes some way, but not far enough, to doing these.
bmj.com/content/372/bm…
bmj.com/content/372/bm…
10. If we want to not just open schools, but *keep* them open, we need to keep reducing cases & get rates in the community much lower.
If we want to open up our lives more generally, we need to drive cases lower still - back to at least where we were last July.
If we want to open up our lives more generally, we need to drive cases lower still - back to at least where we were last July.
11. Why do cases matter so much? It's not just about the unfairness of putting the burden of covid on disadvantaged communities (jackiecassell.com/self-isolation…) but it's also about protecting everyone.
There are 2 main protections low cases give us.
There are 2 main protections low cases give us.
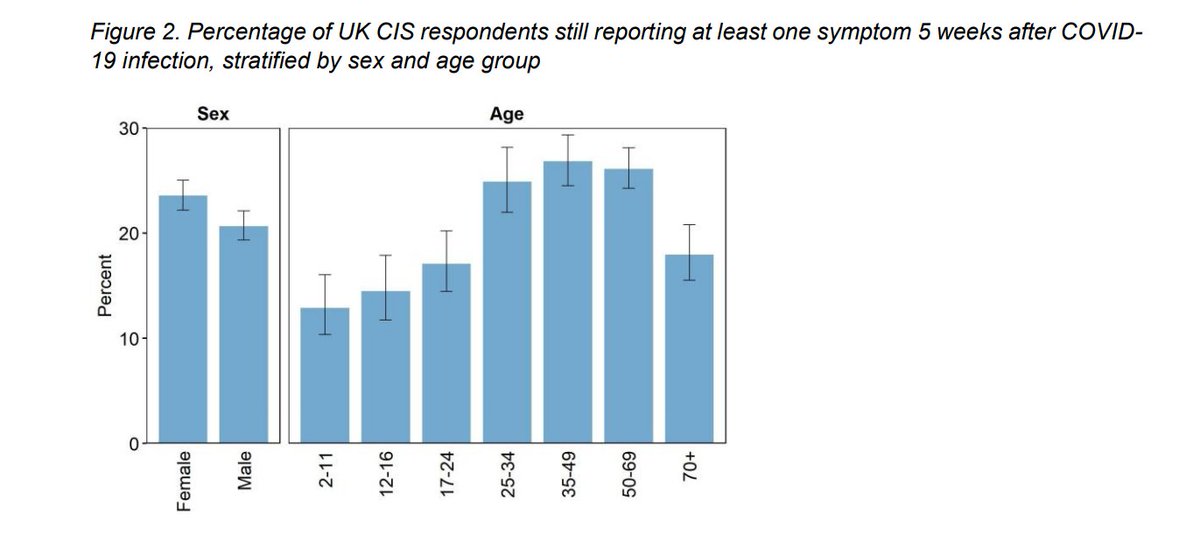
12. Firstly, preventing long covid, particularly in younger adults who will be vaccinated last.
A recent US case-control study showed over 35% of people with mild to severe covid still had symptoms 6 months later. 30% reported worse quality of life.
jamanetwork.com/journals/jaman…
A recent US case-control study showed over 35% of people with mild to severe covid still had symptoms 6 months later. 30% reported worse quality of life.
jamanetwork.com/journals/jaman…

13. A SAGE study in England of people who had been discharged after a Covid hospital stay, showed that 12% died within 5 months & 30% were readmitted to hospital.
The risks were *higher* in younger people after taking into account normally better health.
gov.uk/government/pub…
The risks were *higher* in younger people after taking into account normally better health.
gov.uk/government/pub…

14. Long covid is also increasingly recognised in kids (& vaccines not yet licenced for kids).
I discussed this in a recent thread
Basically - long covid seems pretty common and pretty unpleasant. We should be trying to avoid it by avoiding cases.
I discussed this in a recent thread
https://twitter.com/chrischirp/status/1363473889951637504?s=20
Basically - long covid seems pretty common and pretty unpleasant. We should be trying to avoid it by avoiding cases.
15. The second super important reason to keep cases low is to reduce the chance of a vaccine resistant variant arising here. Every case is an extra chance for covid to mutate.
See this article on variants & vaccines! lrb.co.uk/the-paper/v43/…
See this article on variants & vaccines! lrb.co.uk/the-paper/v43/…
16. If a vaccine resistant variant *did* take hold here it could re-expose more vulnerable vaccinated populations to serious infection - & death. We would likely require *new severe restrictions* until booster vaccines were available (perhaps many months). It could be a disaster.
17. To reduce this chance, we *also* need to tighten our border controls this year – minimal international travel and managed quarantine for everyone (inc returning UK citizens) at the border to prevent importing new cases and new variants.
theguardian.com/world/2021/feb…
theguardian.com/world/2021/feb…
18. So how does the roadmap do in the light of all the above?
Its caution is good. The long wait between phases does allow for proper assessment. Starting with schools and the outdoors is the right approach. It discusses tackling inequalities in exposure & vaccine uptake.
BUT
Its caution is good. The long wait between phases does allow for proper assessment. Starting with schools and the outdoors is the right approach. It discusses tackling inequalities in exposure & vaccine uptake.
BUT
19. The focus on determining speed of opening by hospitalisations instead of cases is *wrong*.
It's cases (in anyone) we need to keep down for the reasons above – low hospitalisations will naturally follow.
It's cases (in anyone) we need to keep down for the reasons above – low hospitalisations will naturally follow.
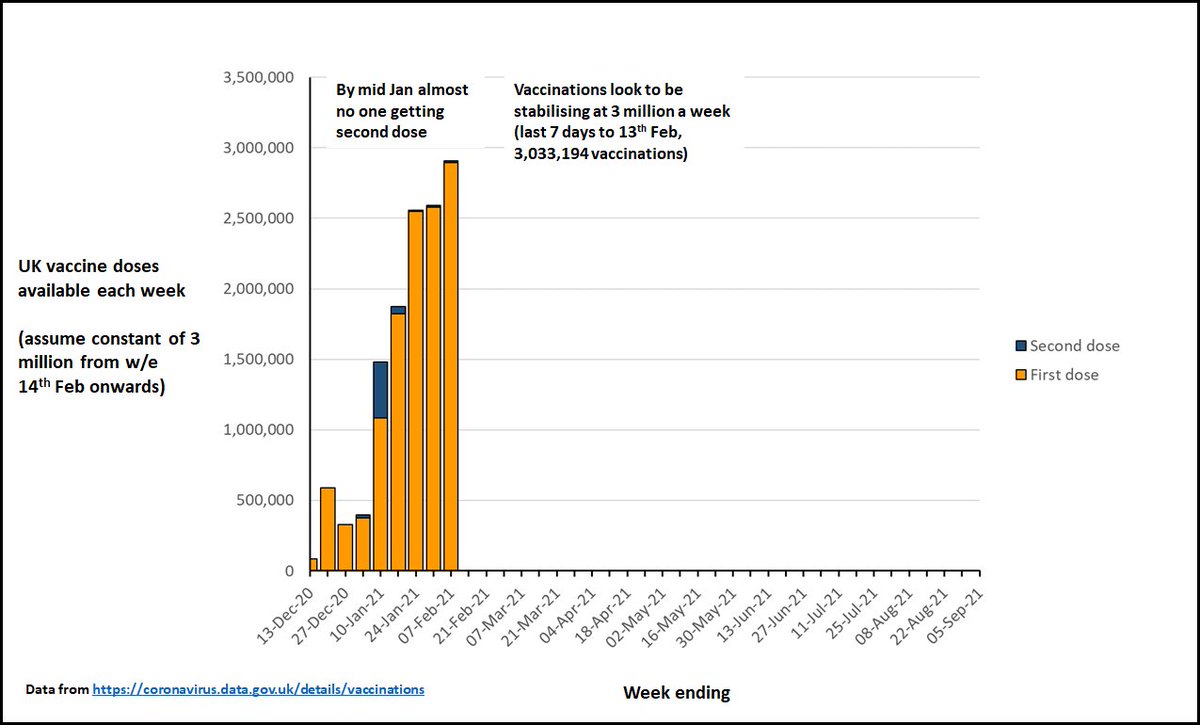
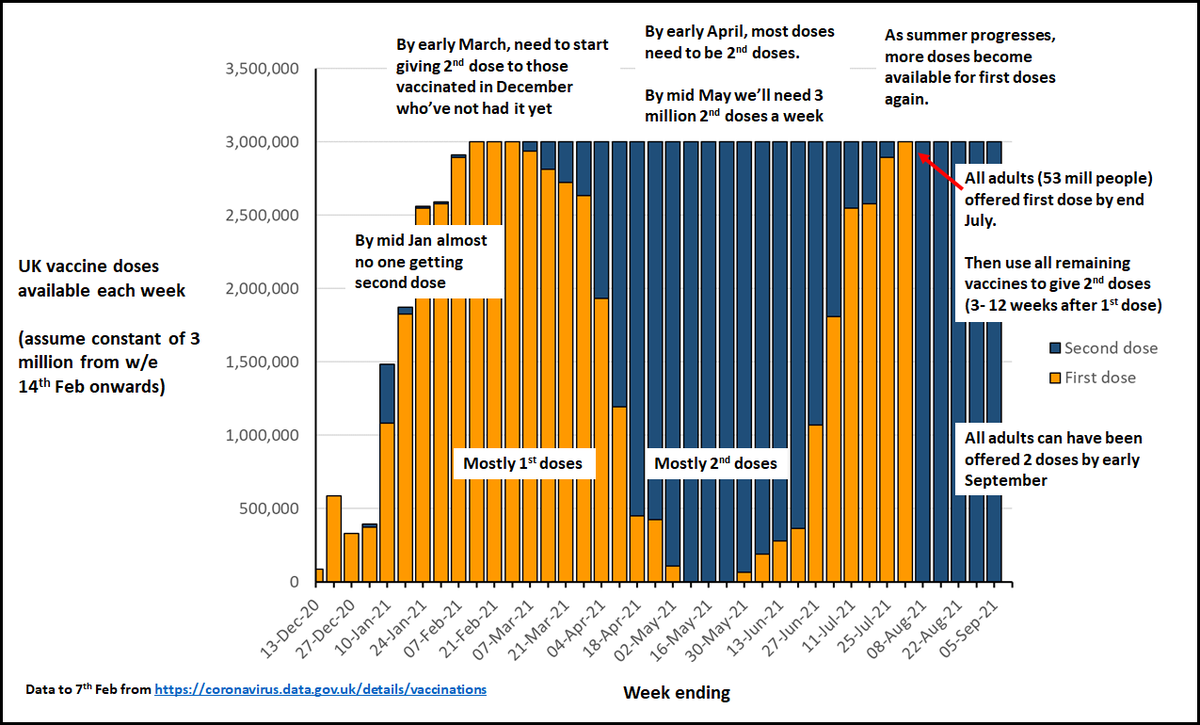
20. The roadmap relies overmuch on the vaccines. The vaccines are amazing but can't solve everything.
We can HELP vaccines control cases AND address the inequalities in exposure & protection, by supporting isolation, making workplaces & schools safer and supporting communities.
We can HELP vaccines control cases AND address the inequalities in exposure & protection, by supporting isolation, making workplaces & schools safer and supporting communities.
21. SAGE modelling released this week paints a pessimistic picture of being able to avoid a second third wave (assets.publishing.service.gov.uk/government/upl…) and a pessimistic picture of the impact of opening schools (cmmid.github.io/topics/covid19…).

22. Going all in on support & infrastructure to reduce cases to a really low level while rolling out vaccine is the best bet for avoiding thousands of deaths and further lockdowns.
It also maximises the impact of the vaccines.
Let’s do it.
independentsage.org/a-sustainable-…
It also maximises the impact of the vaccines.
Let’s do it.
independentsage.org/a-sustainable-…
PS! we should of course also be making schools as safe as possible.
And the reasons for getting cases low mean we shouldn't be ok with R above 1 with schools open as PM seemed ok with today. Implementing additional supports should keep R below 1 (& cases reducing)
And the reasons for getting cases low mean we shouldn't be ok with R above 1 with schools open as PM seemed ok with today. Implementing additional supports should keep R below 1 (& cases reducing)
• • •
Missing some Tweet in this thread? You can try to
force a refresh