Neil Ferguson, notorious lead author of Imperial College model, sent a snarky and supercilious response to an earnest but questioning citizen concerned about policy. Full significance of Ferguson's reply wasn't appreciated by recipient but will be understood by old CA readers. 
https://twitter.com/toadmeister/status/1363409373419233280

2/ Ferguson's go-to reference for someone daring to question his statistical work was the following: climatechangecommunication.org/wp-content/upl…. Guess what it was. Without peeking.
3/ COVID modeler Neil Ferguson's go-to reference was Lewandowsky and Cook, 2020. The Conspiracy Theory Handbook.


4/ I encountered Lewandowsky and Cook many years ago: they are the worst of the worst. See
climateaudit.org/tag/lewandowsky. If COVID modeler Neil Ferguson is citing them as scientific authority, then, to borrow a favorite climate phrase, his work is "worse than we thought".
climateaudit.org/tag/lewandowsky. If COVID modeler Neil Ferguson is citing them as scientific authority, then, to borrow a favorite climate phrase, his work is "worse than we thought".
5/ in a 5-second quick look at Lewandowsky and Cook's latest propaganda tract, I noticed that they continue to assert an urban legend propagated years ago by Lewandowsky that arose from gross statistical incompetence by him and his social psychology community.

6/ I looked at the actual data relied upon by Lewandowsky to support his Princess Diana claim. climateaudit.org/2013/11/07/mor…
7/ Lewandowsky's assertion was based on a crappy article (Wood et al 2012) which did rudimentary statistical analysis on Likert-scale questionnaire data, the distributions of which did not satisfy the assumptions of the statistical method. As a result, conclusions were unfounded

8/ although Lewandowsky claimed that this correlation PROVED that respondents held two inconsistent beliefs, if one actually looked at the data - a practice seemingly anathema to today's university academic modelers, ZERO respondents actually held the inconsistent beliefs.


10/ my current notice of Ferguson arose as follows.
As elsewhere, COVID cases in Canada have declined sharply in past 6 weeks, but public health authorities nonetheless urged even more punitive lockdowns due to looming third wave from UK variant:
cbc.ca/news/politics/…
As elsewhere, COVID cases in Canada have declined sharply in past 6 weeks, but public health authorities nonetheless urged even more punitive lockdowns due to looming third wave from UK variant:
cbc.ca/news/politics/…
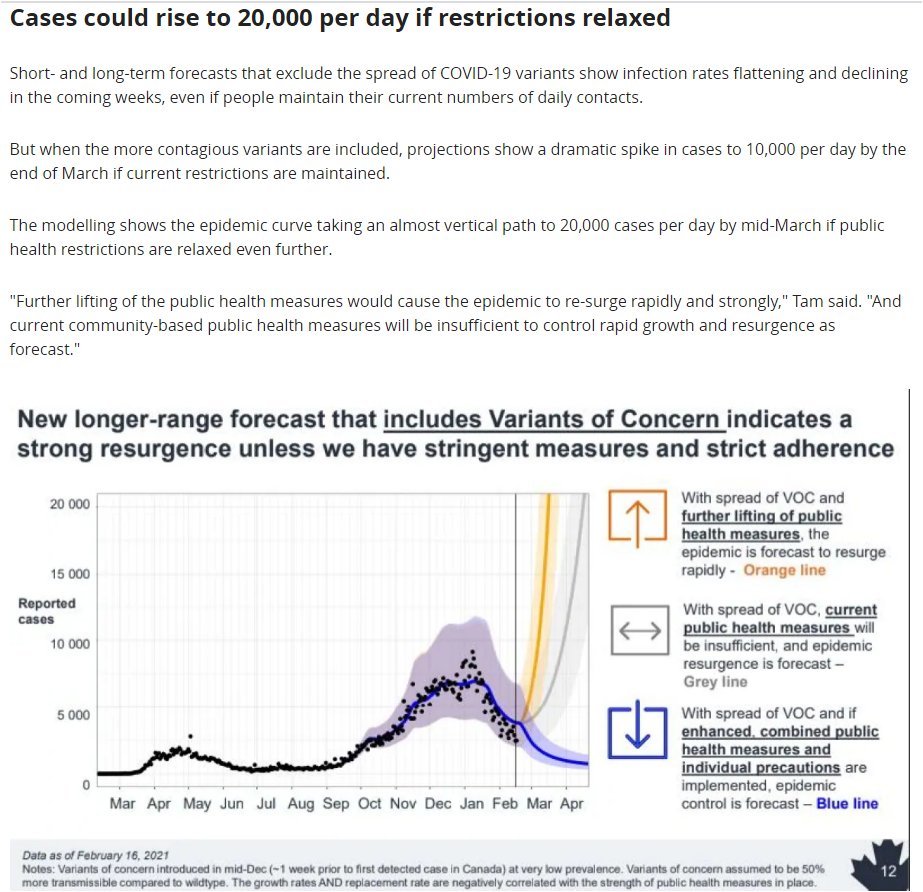
11/ while the Public Health Canada's February projections didn't give a reference for their projections, earlier presentations cited Anderson et al, from which I located graph that almost certainly underpins PH Canada's own graphic. sfu.ca/magpie/blog/hi…

12/ according to its covering note. the variant hockey stick graph was constructed as a purely mathematical exercise of inserting a variant (B.1.1.7) with 40-80% higher transmissibility. Estimate of higher transmissibility relied on Volz et al (Jan 4, 2021).

13/ So who are Volz et al? Here is link to original article: medrxiv.org/content/10.110….
Senior author is .... Neil Ferguson.
Senior author is .... Neil Ferguson.

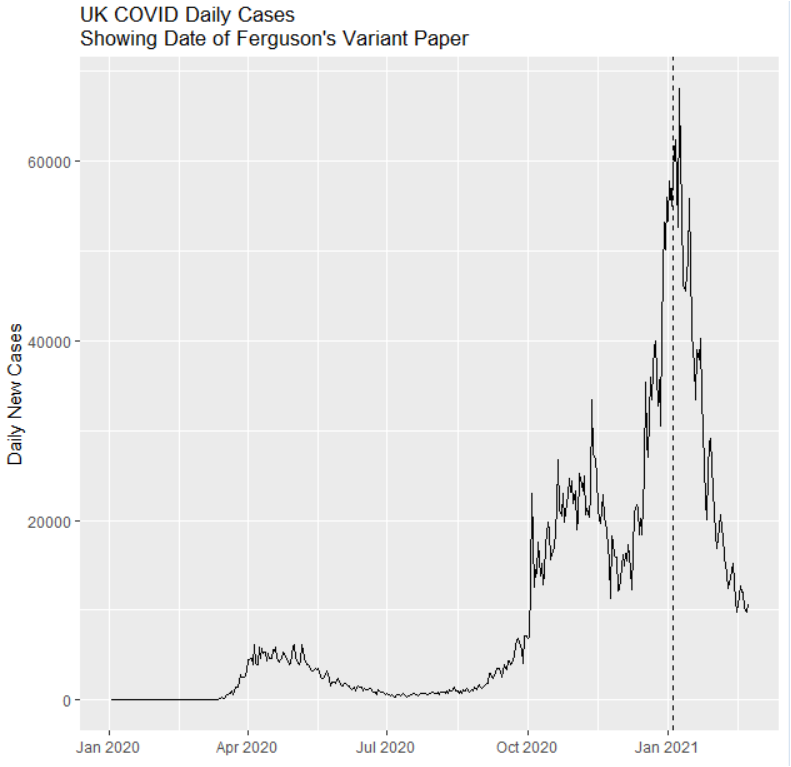
14/ if one plots the date of Ferguson's variant paper against UK data on new cases, it was published at the absolute "top of the market". ALL of his calculations on relative transmissibility of B.1.1.7 are based on rising "market". Do his calculations work out of sample?
15/ I've spent the day trying to figure out Ferguson's code and data. They've put Supplementary Information online github.com/mrc-ide/sarsco… It's not very clearly presented but at least it's there. I wonder if anyone other than me has tried to run it, as it needs bodges to run.
16/ one bit of good fortune in trying to parse this study: they use the lmer function from the lme4 package for at least some of their key calculations.

17/ veteran readers may recall that I frequently used lme4 for analysis. Early on, I advocated it as a rational statistical basis for tree ring chronologies and had even planned to present it at a dendro conference in Finland, to which I'd been invited
climateaudit.org/tag/mixed-effe…
climateaudit.org/tag/mixed-effe…
• • •
Missing some Tweet in this thread? You can try to
force a refresh