
Our paper on identifying and mitigating biases in epidemiologic studies of #COVID-19 is now out and is #OA . doi.org/10.1007/s10654…. Skillfully led by
@AccorsiEmma
this project involved much of our group and many discussions arising from papers we were reading.
@AccorsiEmma
this project involved much of our group and many discussions arising from papers we were reading.
including @XuetingQ @EvaRumpler @LeeKShaffer @rebeccajk13 Ed Goldstein @NeneRiehus from @CCDD_HSPH with special guests @mats_julius and @mugecevik .
We consider the challenges of several kinds of studies: 1. Seroprevalence studies to estimate cumulative incidence
where a key challenge is representativeness of participants
where a key challenge is representativeness of participants

and another (easier to adjust for) is imperfect test characteristics

2. Seroprotection studies (like this that just came out jamanetwork.com/journals/jamai… ) that seek to study the protection that prior infection or antibodies generated by it gives vs. future infection
Here key challenges are confounding (because the exposure and the outcome are both SARS-CoV-2 infection (or its consequence) just at different times -- so they share many common causes, as well as the issue of distinguishing direct from indirect effects

3. Risk factors for becoming infected. Here key challenges are selection biases of various sorts whereby those who are tested are at differential risk for infection from the source population

And differential misclassification because different kinds of tests are combined in one analysis, with different test characteristics, and different kinds of people tend to get different kinds of test. A risk factor for which test you get can look like a risk factor for infxn
For example different kinds of people get PCR vs serologic vs. antigen tests and the outcome is "any positive." Something similar is what makes interpretation of "any infection" in vaccine effectiveness studies tricky.
https://twitter.com/mlipsitch/status/1364744541903986698?s=20(from a reply to another thread)
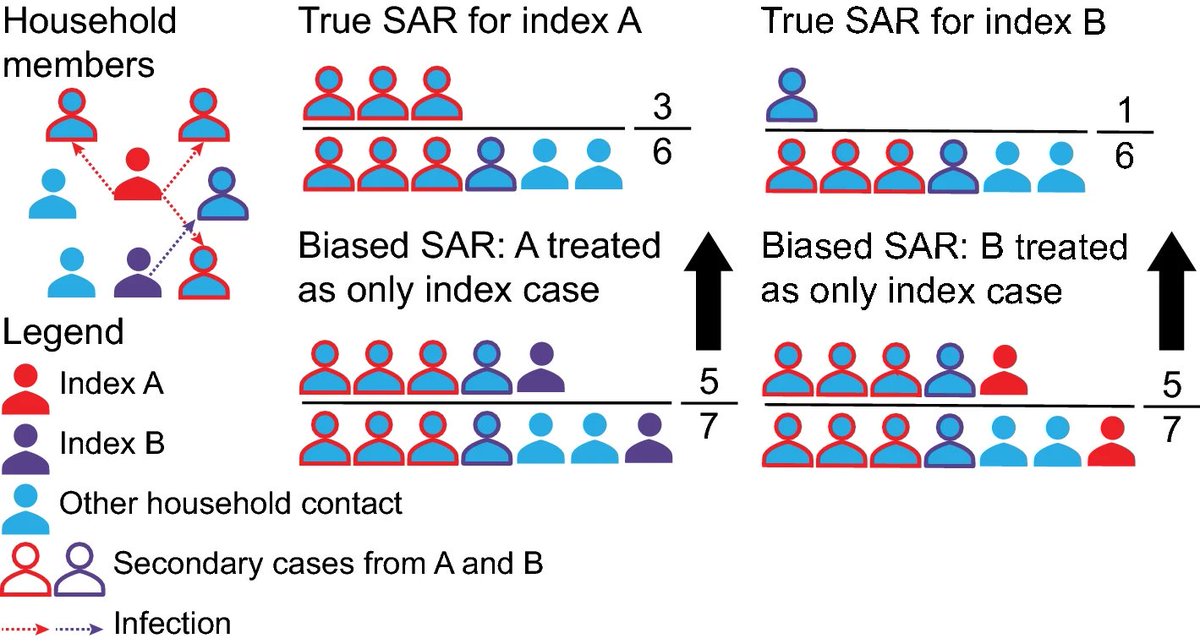
4. Secondary attack rate estimation eg in households. Lots of issues here. a) misclassifying index case (for example if the true index case is not the first to get sick in the hh)

b) misclassifying index when there are more than one but only one identified
c) misclassifying the contact type and infection status

d) misclassification of close contacts

We did our best to explain these sometimes subtle issues clearly (a large group of mixed backgrounds helped us, we think, ferret out unclarities) and offer practical solutions. We hope it will be useful to those (including ourselves) working on design and analysis of epi studies
Oh no! I was multitasking when I started this thread and left off coauthors @KeyaJoshi3 and @LeeKShaffer -- purely due to distraction - sorry! It was a great team effort.
@threadreaderapp unroll
Thread continues here.
https://twitter.com/mlipsitch/status/1365063947339055104?s=20
• • •
Missing some Tweet in this thread? You can try to
force a refresh


