Our paper “Estimated transmissibility and impact of SARS-CoV-2 lineage B.1.1.7 in England” has now been published in Science (early release: science.sciencemag.org/content/early/…). I’ve tweeted about this a few times before, so I’m going to focus here on some key messages. (1/8)
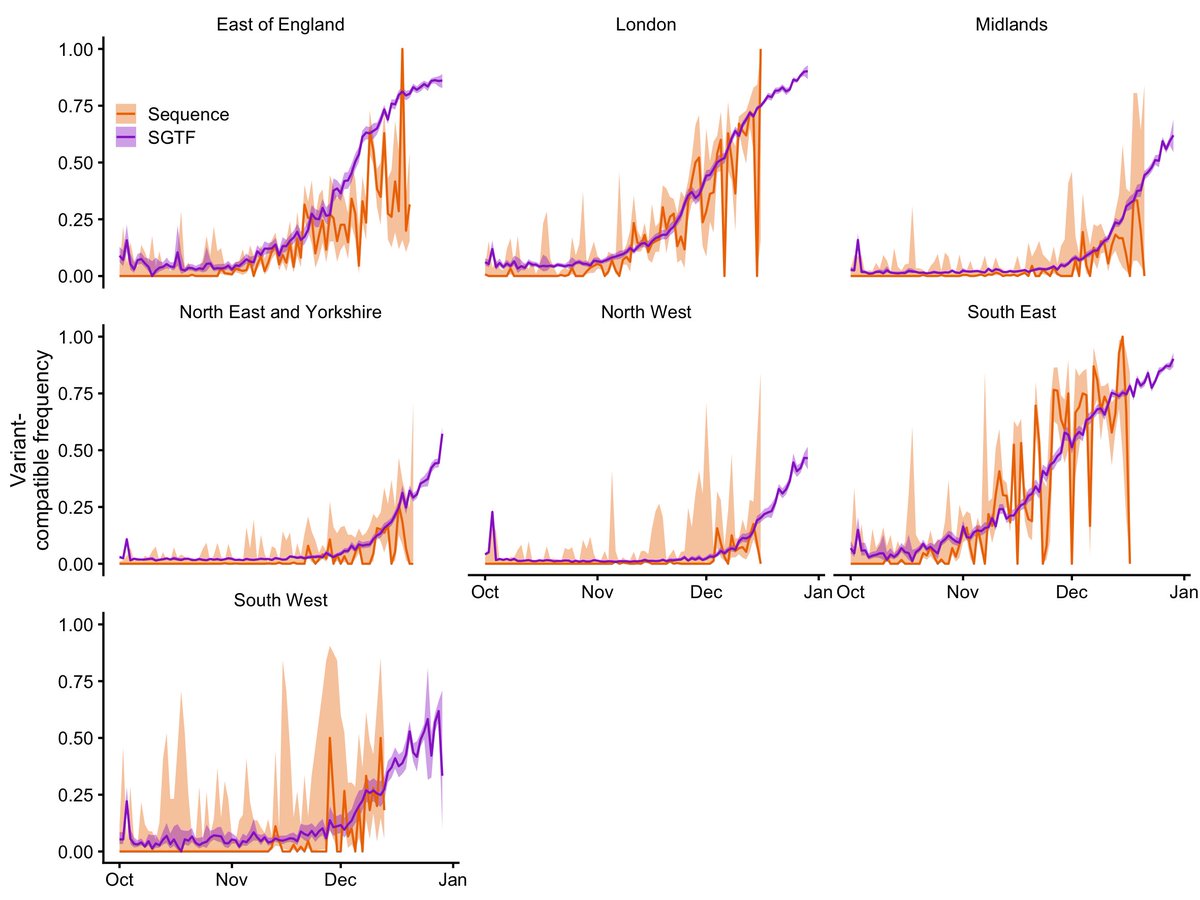
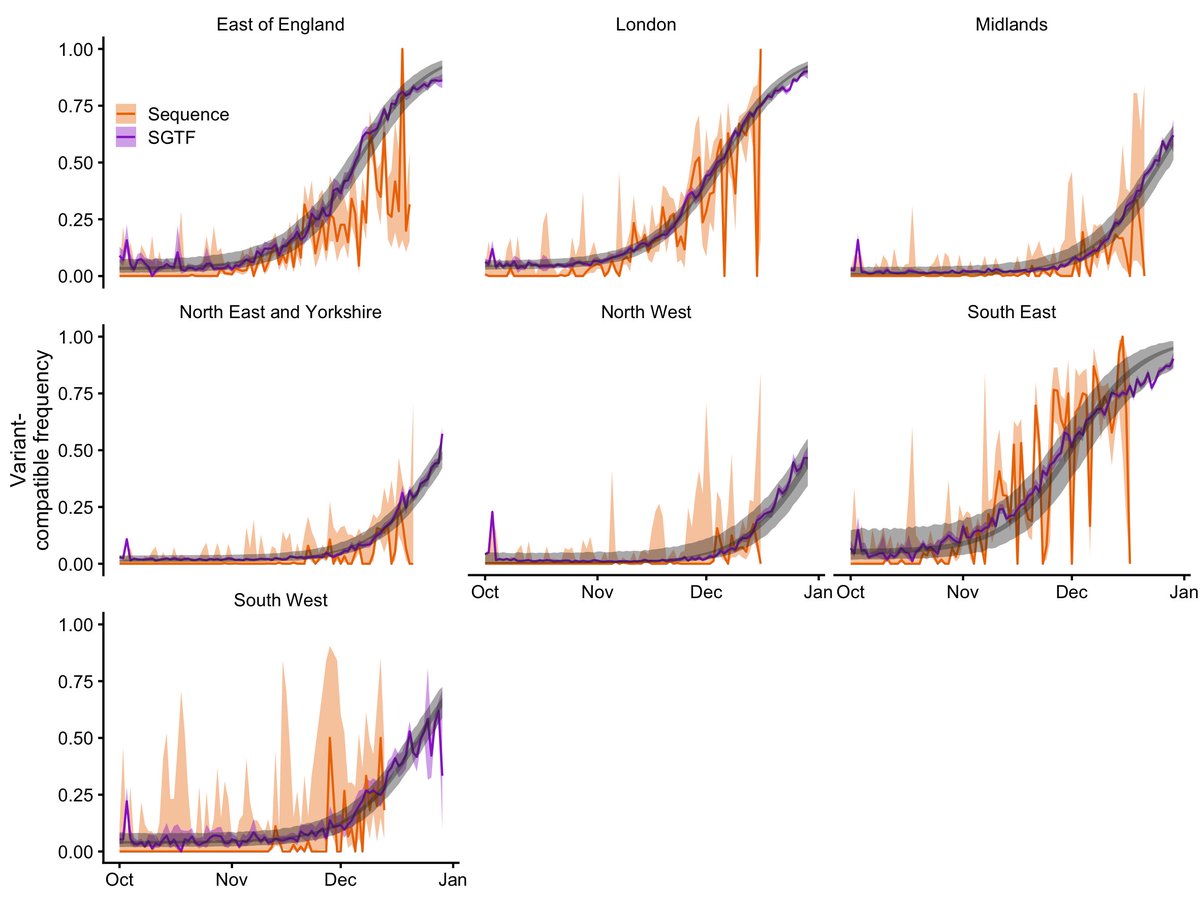
B.1.1.7 has a 43–90% higher reproduction number than previous SARS-CoV-2 strains. This holds for several different methods we used to analyse its spread, and we found similar rates of increase in the UK, Denmark, Switzerland, and the United States. (2/8) 

Back in December, we predicted that B.1.1.7 would cause a huge surge in cases and that without stringent measures and faster vaccine deployment, more people in England would likely die from COVID-19 in the first half of 2021 than in all of 2020. (3/8)

Given all the big improvements in COVID-19 treatment over 2020, I found this result hard to get my head around. Stringent restrictions were imposed, and the vaccine schedule was accelerated in the UK. These definitely helped save lives. (4/8)

Even with these measures, 42,000 people in England have died from COVID-19 in the first two months of 2021, equal to the number who died in March–Oct 2020 (8 months). I’m certain that much of this loss of life would have been avoided without B.1.1.7. (5/8)

B.1.1.7 has now spread globally (cov-lineages.org/global_report_…). Other high-income countries have gotten vaccine campaigns well underway before B.1.1.7 hit them, and I hope this will help to mitigate its effect. Lower-income countries may not, and need more support. (6/8)

I can finally say NOW PEER REVIEWED! Thanks to all my coauthors: @seabbs @BarnardResearch @Jarvis_Stats @AdamJKucharski @JDMunday @cap1024 @timwrussell @DamienTully @Alex_Washburne @TWenseleers @amyg225 @ve3hw @kerrylmwong @KevinvZandvoort @inschool4life @cmmid_lshtm ... (7/8)
Thanks to coauthors, continued... thank you @CovidGenomicsUK @karlado @RuthHKeogh @rozeggo @sbfnk @markjit @katiito and John Edmunds! (8/8)
• • •
Missing some Tweet in this thread? You can try to
force a refresh