1/G
I made some threads on how those behind the Great Barrington Declaration (GBD; @gbdeclaration) spread disinformation on COVID-19.
On this thread I'll go over some reasons why the GBD itself is nonsense
I made some threads on how those behind the Great Barrington Declaration (GBD; @gbdeclaration) spread disinformation on COVID-19.
https://twitter.com/AtomsksSanakan/status/1361744135619809280
https://twitter.com/AtomsksSanakan/status/1341563596405354496
https://twitter.com/AtomsksSanakan/status/1359933089527570432
On this thread I'll go over some reasons why the GBD itself is nonsense
2/G
GBD's main point is "focused protection"; i.e. strategies that limit infection risk among older people + others at greater risk of dying from COVID-19, while allowing less vulnerable people to live with less restrictions.
gbdeclaration.org
GBD's main point is "focused protection"; i.e. strategies that limit infection risk among older people + others at greater risk of dying from COVID-19, while allowing less vulnerable people to live with less restrictions.
gbdeclaration.org
3/G
An obvious problem with that is infection can spread from people less at risk of dying from COVID-19, to people at greater risk of dying from COVID-19.
So allowing the non-vulnerable to get infected places the vulnerable at risk.
ncbi.nlm.nih.gov/pmc/articles/P…
An obvious problem with that is infection can spread from people less at risk of dying from COVID-19, to people at greater risk of dying from COVID-19.
So allowing the non-vulnerable to get infected places the vulnerable at risk.
ncbi.nlm.nih.gov/pmc/articles/P…

4/G
Example:
Sweden had a higher infection rate in its general population than did its Nordic neighbors
ssi.dk/aktuelt/nyhede…
covid19.ssi.dk/overvagningsda…
thl.fi/roko/cov-vaest…
nejm.org/doi/10.1056/NE…
fhi.no/studier/preval…
folkhalsomyndigheten.se/folkhalsorappo…
medrxiv.org/content/10.110…
Example:
Sweden had a higher infection rate in its general population than did its Nordic neighbors
ssi.dk/aktuelt/nyhede…
covid19.ssi.dk/overvagningsda…
thl.fi/roko/cov-vaest…
nejm.org/doi/10.1056/NE…
fhi.no/studier/preval…
folkhalsomyndigheten.se/folkhalsorappo…
medrxiv.org/content/10.110…
5/G
That led to a higher infection rate in Sweden's healthcare staff, including in nursing homes.
ncbi.nlm.nih.gov/pmc/articles/P…
ncbi.nlm.nih.gov/pmc/articles/P…
That increases the change of older people in nursing homes getting infected.
ncbi.nlm.nih.gov/pmc/articles/P…
That led to a higher infection rate in Sweden's healthcare staff, including in nursing homes.
ncbi.nlm.nih.gov/pmc/articles/P…
ncbi.nlm.nih.gov/pmc/articles/P…
That increases the change of older people in nursing homes getting infected.
https://twitter.com/AtomsksSanakan/status/1287823818455744515
ncbi.nlm.nih.gov/pmc/articles/P…

6/G
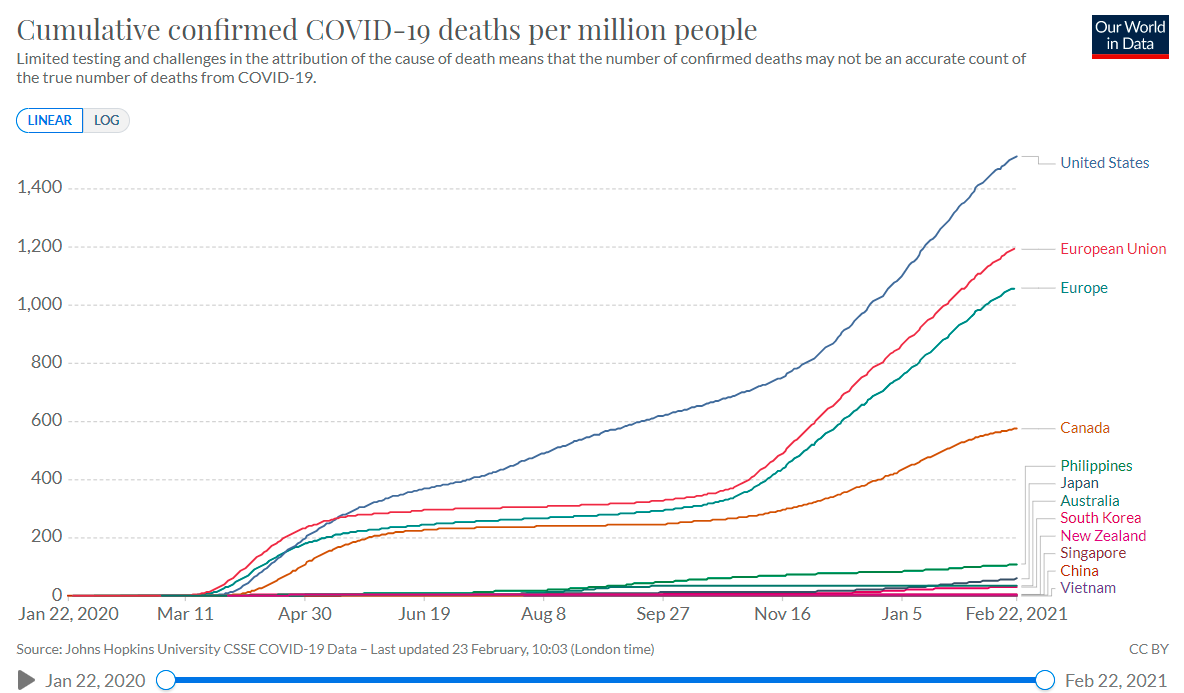
That higher infection rate led to poor outcomes in Sweden.
And even with that, Sweden was nowhere near achieving the "herd immunity" the GBD aims for. That would require way more infections, with more deaths.
ourworldindata.org/coronavirus-da…
That higher infection rate led to poor outcomes in Sweden.
And even with that, Sweden was nowhere near achieving the "herd immunity" the GBD aims for. That would require way more infections, with more deaths.
https://twitter.com/AtomsksSanakan/status/1354830205454610433
ourworldindata.org/coronavirus-da…

7/G
Sweden's government setup a coronavirus commission to figure out where they went wrong.
The commission noted that Sweden's single biggest mistake was letting a large number of people get infected in the general population
coronakommissionen.com/wp-content/upl…
thelocal.se/20201215/what-…
Sweden's government setup a coronavirus commission to figure out where they went wrong.
The commission noted that Sweden's single biggest mistake was letting a large number of people get infected in the general population
coronakommissionen.com/wp-content/upl…
thelocal.se/20201215/what-…

8/G
Sweden's government learned from that. So they tried to limit community-wide infection during their 2nd wave, instead of just in the "vulnerable".
That contradicts what GBD recommended.
thelocal.se/20201203/swede…
swedishchamber.nl/news/sweden-ba…
Sweden's government learned from that. So they tried to limit community-wide infection during their 2nd wave, instead of just in the "vulnerable".
That contradicts what GBD recommended.
https://twitter.com/DrKatrin_Rabiei/status/1339988276229206017
thelocal.se/20201203/swede…
swedishchamber.nl/news/sweden-ba…

9/G
So one protects the "vulnerable" by shifting how the "non-vulnerable" behave. The same principle applies in vaccination, including for pathogens besides SARS-CoV-2. We often vaccinate those at ↓ risk, because it indirectly protects those at ↑ risk.
publichealthontario.ca/-/media/docume…
So one protects the "vulnerable" by shifting how the "non-vulnerable" behave. The same principle applies in vaccination, including for pathogens besides SARS-CoV-2. We often vaccinate those at ↓ risk, because it indirectly protects those at ↑ risk.
publichealthontario.ca/-/media/docume…

10/G
I have not seen GBD proponents give a means of "focused shielding" that hasn't already failed under conditions with high infection rates.
That's because allowing for more community-wide infection undermines shielding, contrary to what GBD assumes.
I have not seen GBD proponents give a means of "focused shielding" that hasn't already failed under conditions with high infection rates.
That's because allowing for more community-wide infection undermines shielding, contrary to what GBD assumes.
https://twitter.com/AtomsksSanakan/status/1349173276262719488
11/G
So that's the core set of problems with the Great Barrington Declaration. Following it kills people.
To run through some other problems:
Way too many people would need to be infected to get to herd immunity before a vaccine
So that's the core set of problems with the Great Barrington Declaration. Following it kills people.
To run through some other problems:
Way too many people would need to be infected to get to herd immunity before a vaccine
https://twitter.com/AtomsksSanakan/status/1353863914501640192
https://twitter.com/AtomsksSanakan/status/1341851013096083461
12/G
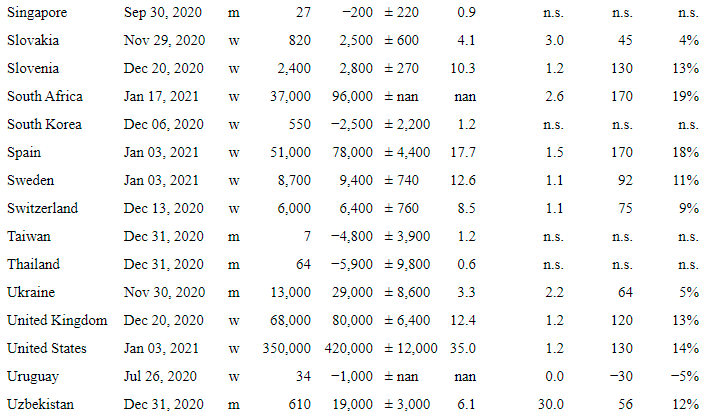
Those behind the GBD illegitimately downplay how many people would die from their policy, by repeatedly under-estimating the proportion of infected people who die of COVID-19.
Those behind the GBD illegitimately downplay how many people would die from their policy, by repeatedly under-estimating the proportion of infected people who die of COVID-19.
https://twitter.com/AtomsksSanakan/status/1359933089527570432
https://twitter.com/AtomsksSanakan/status/1358018699903565825
13/G
Many middle-aged, non-elderly people die of COVID-19:
link.springer.com/article/10.100…
sciencedirect.com/science/articl…
And COVID-19 can harm younger people, even if it doesn't kill them. So GBD proponents under-estimate the proportion of people needing shielding.
publichealthontario.ca/-/media/docume…
Many middle-aged, non-elderly people die of COVID-19:
link.springer.com/article/10.100…
sciencedirect.com/science/articl…
And COVID-19 can harm younger people, even if it doesn't kill them. So GBD proponents under-estimate the proportion of people needing shielding.
publichealthontario.ca/-/media/docume…

14/G
The GBD is an ideologically-motivated document from people who illegitimately downplayed COVID-19 for months to suit their opposition to particular policies.
It's denialist nonsense on par with tobacco industry propaganda.
bmj.com/bmj/section-pd…
The GBD is an ideologically-motivated document from people who illegitimately downplayed COVID-19 for months to suit their opposition to particular policies.
It's denialist nonsense on par with tobacco industry propaganda.
https://twitter.com/AtomsksSanakan/status/1349261381867073537
bmj.com/bmj/section-pd…

15/G
For more context on the Great Barrington Declaration, see the solid thread below:
For more context on the Great Barrington Declaration, see the solid thread below:
https://twitter.com/GidMK/status/1338336184414572544
https://twitter.com/GidMK/status/1338331883487150080

16/G
Some further context on the risks of high infection rates:
"Indeed, even if an outbreak is mainly concentrated among younger people, it may be very difficult to prevent the virus from spreading among older adults [141]."
link.springer.com/article/10.100…
bmj.com/content/371/bm…
Some further context on the risks of high infection rates:
"Indeed, even if an outbreak is mainly concentrated among younger people, it may be very difficult to prevent the virus from spreading among older adults [141]."
link.springer.com/article/10.100…
bmj.com/content/371/bm…

17/G
And again:
"These findings support the need for comprehensive preventive measures to help reduce the spread of the virus, even in young or middle-aged adults"
sciencedirect.com/science/articl…
[johnsnowmemo.com]
thelancet.com/journals/lance…
And again:
"These findings support the need for comprehensive preventive measures to help reduce the spread of the virus, even in young or middle-aged adults"
sciencedirect.com/science/articl…
[johnsnowmemo.com]
thelancet.com/journals/lance…

18/G
Allowing for high infection rates also aids in the evolution of more dangerous variants of SARS-CoV-2. That's another downside of the GBD's strategy.
Allowing for high infection rates also aids in the evolution of more dangerous variants of SARS-CoV-2. That's another downside of the GBD's strategy.
https://twitter.com/AdamJKucharski/status/1358762039569694725
https://twitter.com/ashishkjha/status/1354995266143875072

19/G
South Korea limited community-wide infections, which helped prevent dangerous virus variants from arising there, as per part 18/G.
Thread below on how southeast Asian countries succeeded by limiting community-wide infection, contrary to the GBD:
South Korea limited community-wide infections, which helped prevent dangerous virus variants from arising there, as per part 18/G.
Thread below on how southeast Asian countries succeeded by limiting community-wide infection, contrary to the GBD:
https://www.twitter.com/AtomsksSanakan/status/1364486601234120704
• • •
Missing some Tweet in this thread? You can try to
force a refresh