- Denominators, Part Two -
Or more of how Ohio's 'special math' works.
I had a question about what the significance of the number of days counted in the cases/100,000 metric is - whether it's 7 days (as the CDC counts it) or 14 days (the way Ohio counts it).
Or more of how Ohio's 'special math' works.
I had a question about what the significance of the number of days counted in the cases/100,000 metric is - whether it's 7 days (as the CDC counts it) or 14 days (the way Ohio counts it).
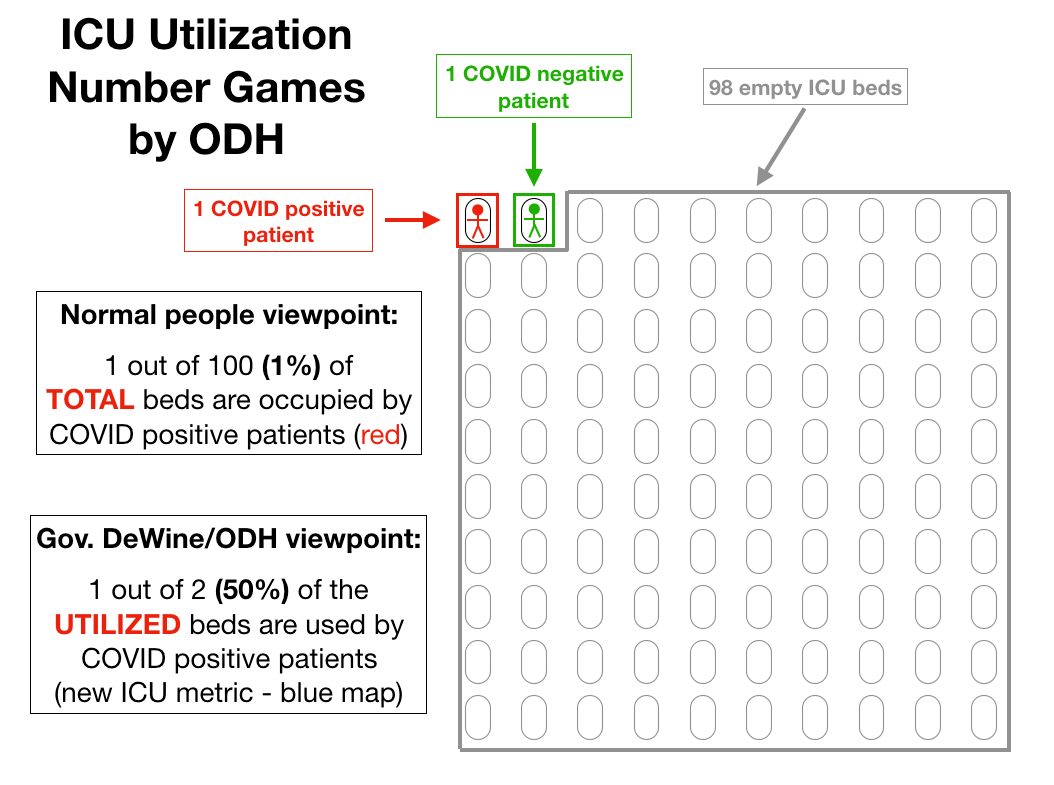
So I figure this is a good time for another set of hypotheticals to illustrate how this all works and how important the details really are. In the first attached graphic, I want you to imagine a county with exactly 100,000 residents that has exactly 7 new cases every single day.
If we count only one week's worth of cases (green box) we come up with 49 cases/100,000 - Freedom!
But if we count over 2 weeks (red box), we are suddenly at 98 cases/100,000!! PANIC!
But if we count over 2 weeks (red box), we are suddenly at 98 cases/100,000!! PANIC!

Just by changing the number of days we count, we can vastly change our rate, despite there being exactly the same number of cases per day.
But there's more to it.
But there's more to it.
We are not in a situation right now where there are exactly the same number of cases per day - cases are dropping over time in reality.
So how does that affect our calculations?
So how does that affect our calculations?
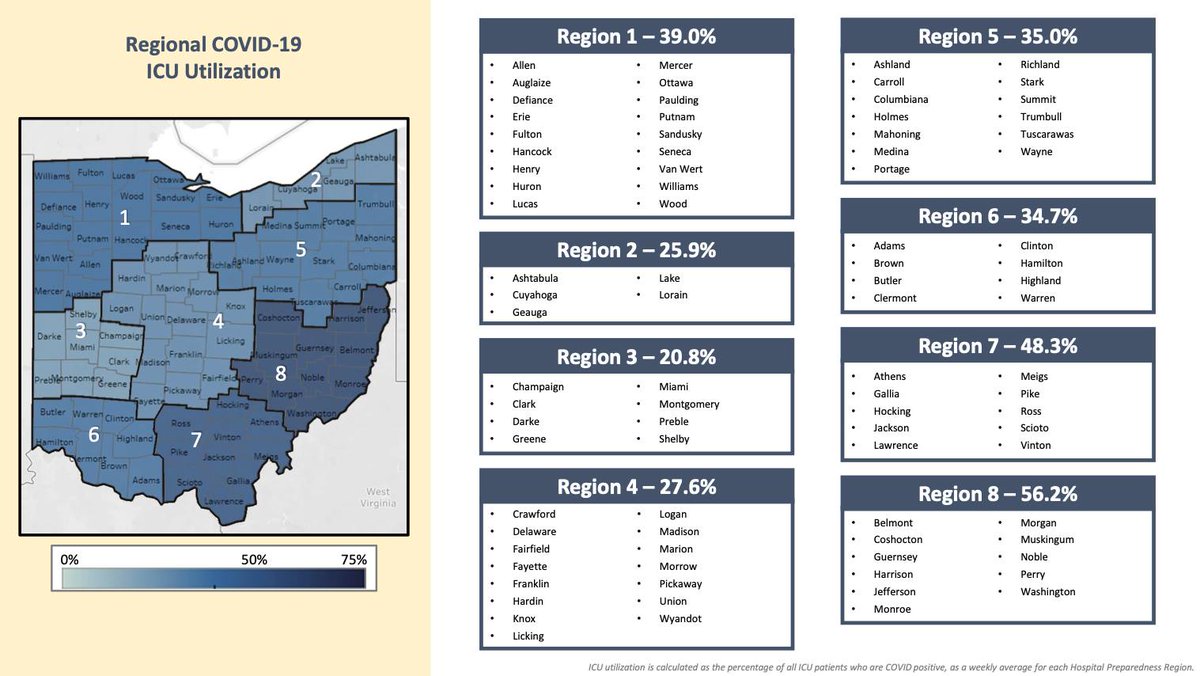
Please see the second attached image for the same hypothetical county with exactly 100,000 people, but this time with a case count that decreases by one from 13 cases to 0 cases over the course of two weeks.

When we add up one week's cases (green box) we end up with just 21 cases/100,000! While over 14 days (red box) we are at 91 cases/100,000!
Again -
⭐️When you control the rules, you control the game. ⭐️
Again -
⭐️When you control the rules, you control the game. ⭐️
• • •
Missing some Tweet in this thread? You can try to
force a refresh