
1/ Man ca 30, exertional dyspnea, CPET with normal VO2max, but pulmonologist concerned about possible drop in CO at peak exercise. Normal resting echo, no LVOT obstruction or gradient, no MR. Dobutamine stress: Chordal SAM, no regional ischemia
2/ Intraventricular gradient 

3/ shown by CMM to be mid ventricular, moving towards apex in systole. No concomitant MR.
What next?
What next?
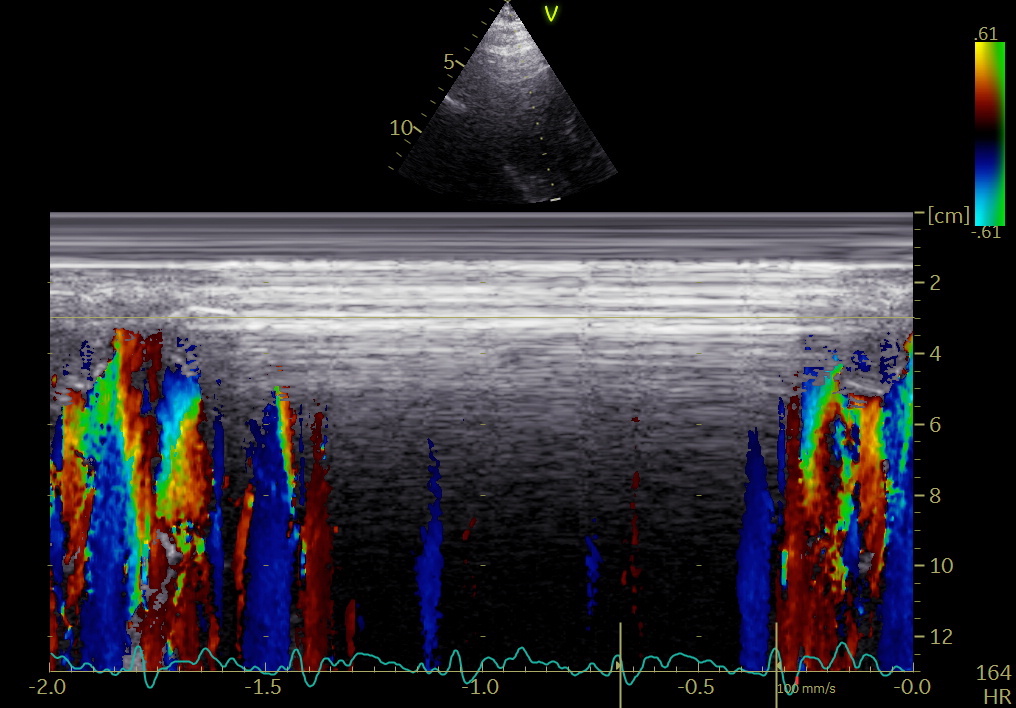
4/ Repeat with exercise stress. Semi supine bicycle exercise, same HR (165, not 180 as the count says): NO SAM, no ischemia.
5/ - and no gradient at all.

6/ The point of this case is that an intraventricular gradient during dobutamine stress is completely unspecific, and related to the artificial hemodynamics created by dobutamine. Low dose increases SV somewhat, and thus reduces EDV. Higher doses increase mainly HR.
7/ Increased HR without further increased CO (no increase in venous return), reduces SV, and EDV, which can give an intrventricular gradient. Exercise increases HR parallel with venous return, increases SV and maintains EDV. Dobu gradient should always be verified by exercise.
• • •
Missing some Tweet in this thread? You can try to
force a refresh














