
B117 variant is now *dominant* in the US. I’m 99% certain that another surge is on the way in April or May. Why? The more contagious #B117 is surging—now crossed the 50% threshold of all cases, in addition to pockets of others variants. 🧵 #COVID19
washingtonpost.com/opinions/2021/…
washingtonpost.com/opinions/2021/…

2) Just Wednesday, #B117 has hit 50% of all cases in the @my_helix database nationwide. It’s been exponentially surging for weeks.

3) @ashishkjha is right- “No matter where you live, it is too early to relax restrictions that continue to have a critical role in controlling this pandemic. From CA to ME, FL to Seattle, the #COVID19 winter is not yet done—highly infectious variants are threatening new storms.”
4) “But the latest national data, which show case rates have plateaued, indicate that we are not there yet. Over the past week, we have seen about 50,000 new cases reported daily. That’s not far from the **height of the surge last summer**”
5) Unfortunately, the public has been served the "it's-under-control" nonsense, pictured on panel A. But the reality is that it is exponentially even it growing slowly - because that’s how ever exponential function starts. It always sneaks ups.
(Figure by @GosiaGasperoPhD)
(Figure by @GosiaGasperoPhD)

6) Take Alberta 🇨🇦 for example—people dismissed it for weeks. But the data is playing out exactly and predicted...
(Figure by @GosiaGasperoPhD).
(Figure by @GosiaGasperoPhD).

7) We had predicted the graph above long ago... here was over a month ago... does it look familiar? It’s almost exactly the shape of the graph above.
https://twitter.com/DrEricDing/status/1361733271328067595
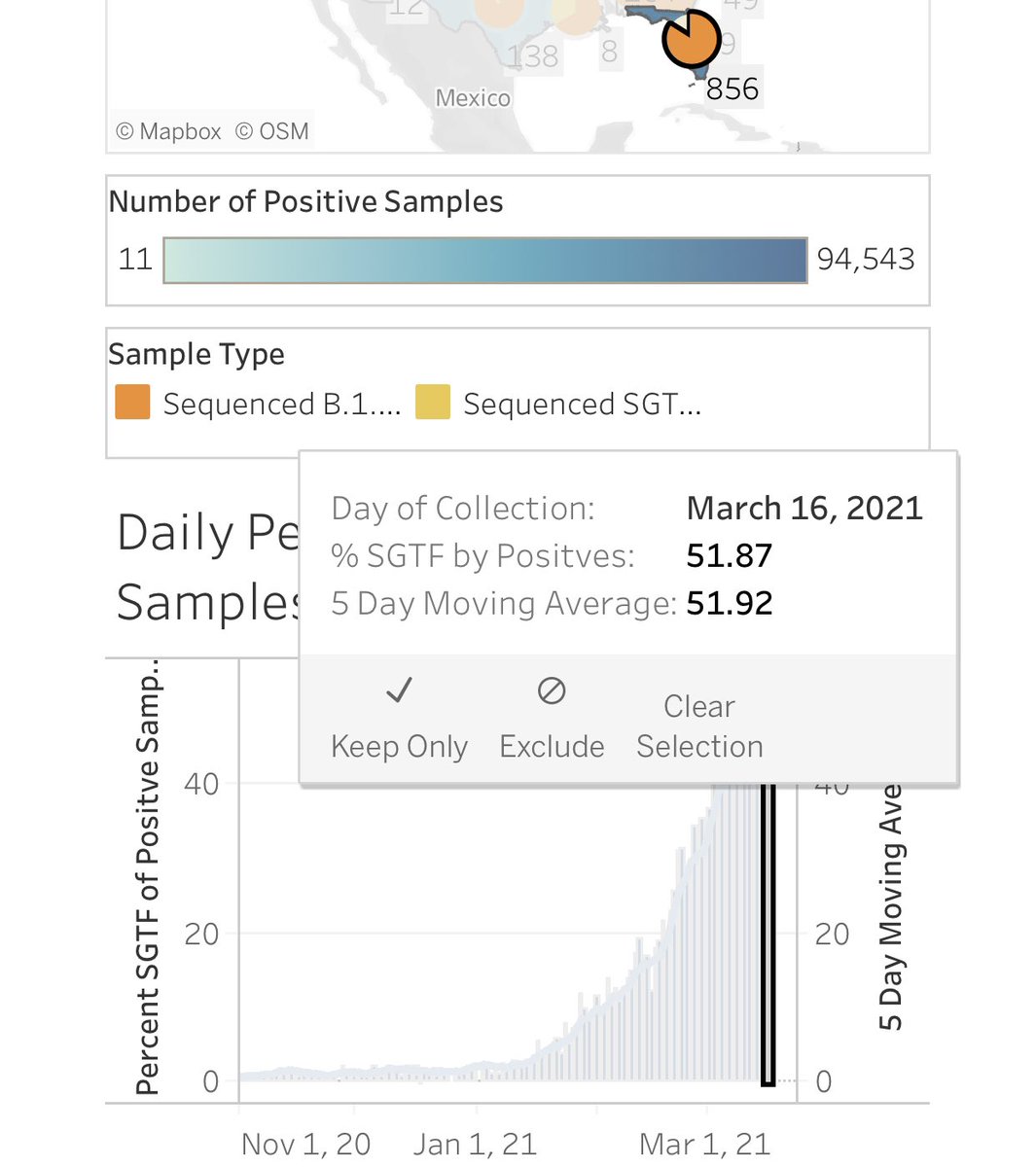
9) But there is a new champion in #B117 lead— 61% #B117 in Georgia, where cases has been rising daily for last 5 days.

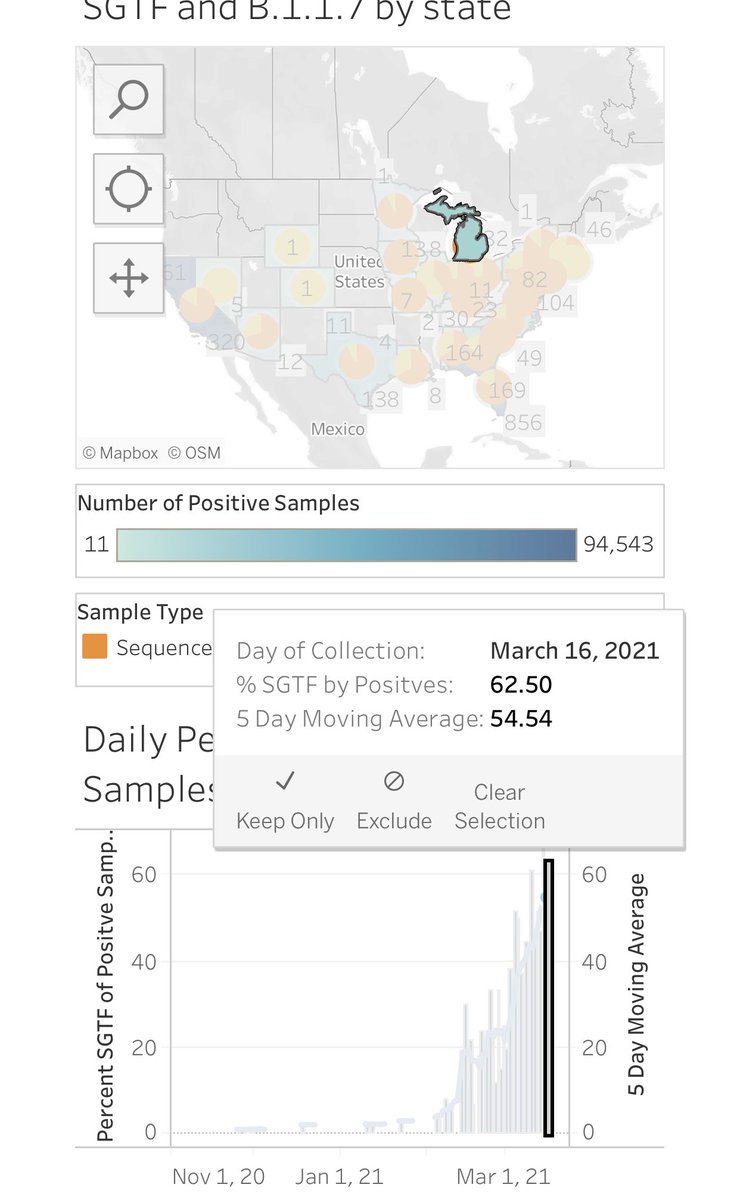
10) And how is Michigan doing in #B117? It tops even Georgia. Michigan #B117 is now 62.5%. How is Michigan cases doing? Also surging in March.

11) it was previously predicted that #B117 would pass 50% previously (@K_G_Andersen’s group) on March 23rd nationwide in the US.
We just passed it early... 6 days early. Damn.
We just passed it early... 6 days early. Damn.
https://twitter.com/drericding/status/1358468446548357123
12) Almost every epidemiologist agrees a 4th surge is coming. It is almost inevitable. The only question is how bad will it be. Maybe not that bad if we vaccinate faster. washingtonpost.com/opinions/2021/…
13) What makes me sad is that, aside from Australia, New Zealand, Vietnam, and Taiwan (all ~zero Covid countries) we never act fast enough until it is much too late. Leadership failures.
Correction- this figure is by @vb_jens.
Correction- this figure is by @vb_jens.

14) But there are other variants to worry about too. In he UK and France, the South Africa #B1351 is also rising steadily. Here is a good thread 🧵 on their rise in the UK. The SA variant is the most problematic in vaccine lab studies so far.
https://twitter.com/dr_d_robertson/status/1372619667668398083?s=21

15) Notably, in the large study of Pfizer and NIH-Moderna vaccinated people, the 🇿🇦 #B1351 variant is the most troublesome. (This thread 🧵 below has been vetted and concurred by 2 immunology colleagues).
Good news is #B117 responds well to the vaccines! so take it!
Good news is #B117 responds well to the vaccines! so take it!
https://twitter.com/DrEricDing/status/1371209487491735553
16) I also want everyone to look carefully just how gosh darn PERFECTLY ACCURATE the Feb 1st model by @GosiaGasperoPhD was to the reality currently. Her forecasts were always exactly as predicted.
Hence let’s please not relax too soon. Surge is coming.
Hence let’s please not relax too soon. Surge is coming.
https://twitter.com/gosiagasperophd/status/1373053575526445057?s=21

17) This is why even with vaccinations, we have to be vigilant — relaxing everything else in terms of mitigation is a recipe for disaster until we have vaccinated up to vaccine herd immunity thresholds — likely 85% range for #B117 given its higher contagiousness.
https://twitter.com/drericding/status/1372853841037770752
18) And please continue to mask even if vaccinated due to residual chance of carrying virus. And definitely do NOT rely on prior #COVID19 infection for sufficient protection. It’s only 47% in the elderly!
https://twitter.com/DrEricDing/status/1372647243560464385
19) Notice the sharp dropoff in the protection from reinfection by age. It’s only ~80% under 65, but only 47% in those 65 or older!
Also semi good news is that protection seems to be as good over 7 months. But not that high.
thelancet.com/action/showPdf…
Also semi good news is that protection seems to be as good over 7 months. But not that high.
thelancet.com/action/showPdf…

20) meantime—I’m more worried about #P1–here is the ominous study on #P1 variant that is now everywhere in 🇧🇷... it is 2.52x faster transmission that old wild common type of #SARSCoV2. That is 152% increase! #B117 is only 40-60% faster.
medrxiv.org/content/10.110…
medrxiv.org/content/10.110…
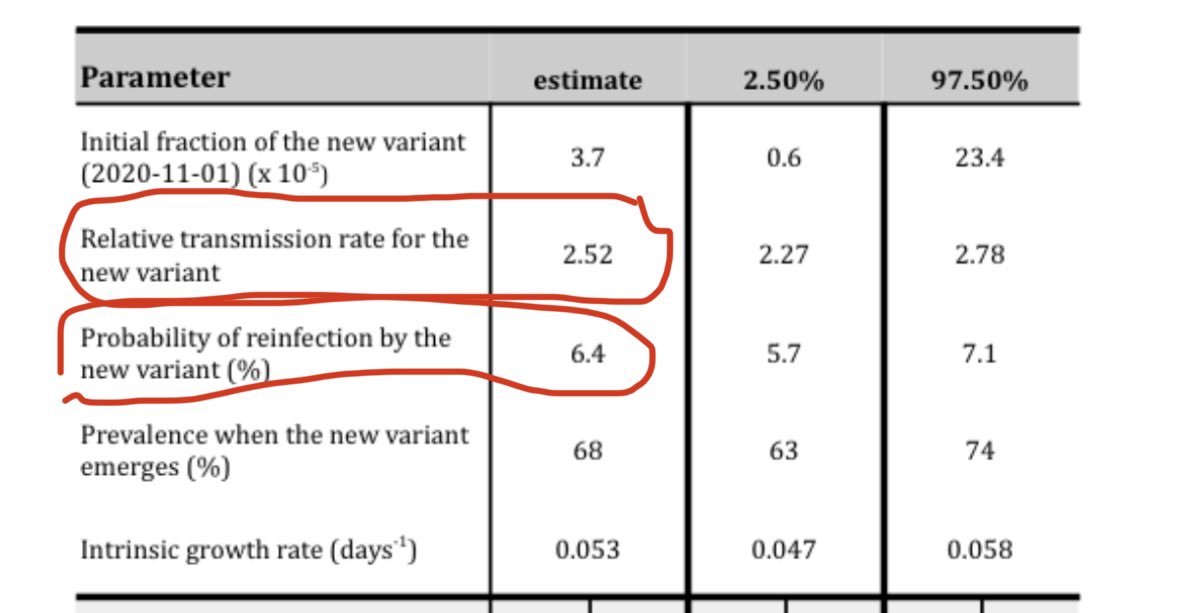
21) Another Brazil 🇧🇷 #COVID19 research group puts #P1 transmission at 2x faster than old strain (instead of 2.5x above), but they estimate a way worse whopping 25-60% reinfection rate! Ugh.
I’m honestly not sure which is worse. Both models really bad. bbc.com/news/amp/healt…
I’m honestly not sure which is worse. Both models really bad. bbc.com/news/amp/healt…
22) to be clear—the Pfizer and Moderna vaccines works against #B117–lots of studies. But for the #P1 and #B1351 variants, neutralization of the pseudovirus in lab by vaccine sera shows slight issues with #P1 and bigger issues with #B1351. We need to urgently chase #ZeroCovid.
https://twitter.com/drericding/status/1371215625562030082


23) I’m a big fan of the J&J single dose vaccine — it not only grows stronger over time, but it also has good efficacy in both South Africa and Brazil! (Albeit before #P1 became heavily dominant in Brazil).
https://twitter.com/drericding/status/1366619383997607941
24) But I’m worried about #P1 and #B117 most of all. #P1 especially because it poses both potential reinfection risk and possibly faster transmission than even the already faster #B117 (see above). We need to keep #P1 contained in Brazil and squash out all 🌎 scattered #P1 cases.
https://twitter.com/DrEricDing/status/1372305355460517891
25) Because we can’t let what’s happening in Brazil keep happening... or let it happen to other countries.
The world needs to unite together during a pandemic with the 3 Musketeers’ “ALL FOR ONE, ONE FOR ALL” motto. Or else we will sink as one planet.
The world needs to unite together during a pandemic with the 3 Musketeers’ “ALL FOR ONE, ONE FOR ALL” motto. Or else we will sink as one planet.

26) Now the US needs to share its vaccine stockpile and vaccine excess orders with the world. And send aid to Brazil 🇧🇷. Or else we will all drown under the variants.
Let’s unite to fight this pandemic... all for one, one for all!
God help us.
Let’s unite to fight this pandemic... all for one, one for all!
God help us.
https://twitter.com/drericding/status/1372005826383204353
27) I’m so tired... been trying to warn about this exact #B117 for over 6 weeks. So so tired.
https://twitter.com/drericding/status/1357566949404905472
28) things in South Florida are going as well as can be expected... #B117 variant surging there.
Why do we ignore this warning sign? I didn’t suffer through a doctorate in epidemiology by age 23, just so that DeSantis can pretend to govern in a pandemic.
sun-sentinel.com/coronavirus/fl…
Why do we ignore this warning sign? I didn’t suffer through a doctorate in epidemiology by age 23, just so that DeSantis can pretend to govern in a pandemic.
sun-sentinel.com/coronavirus/fl…
29) #B117 update—Germany entering a new stricter lockdown after #B117 is growing and fueling another increase across EU.
https://twitter.com/drericding/status/1374203293036056580
• • •
Missing some Tweet in this thread? You can try to
force a refresh




















