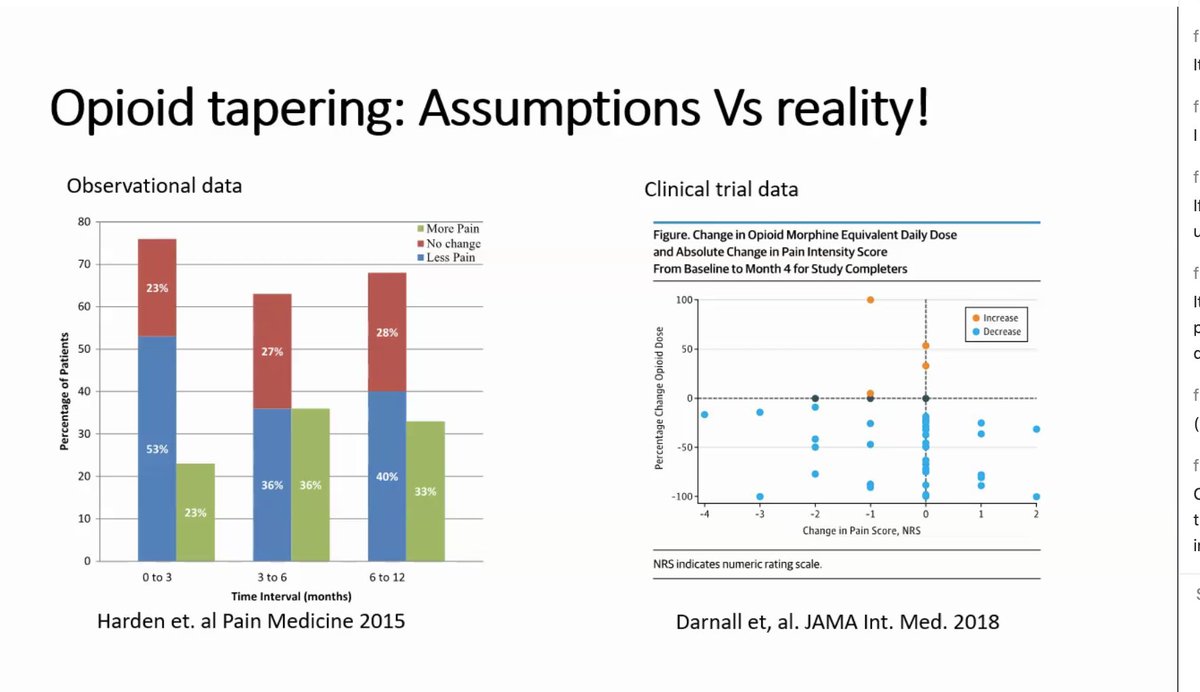
1/Large studies show that in long-term recipients, opioid taper may offer benefit but is *often* harmful (an unclear balance).
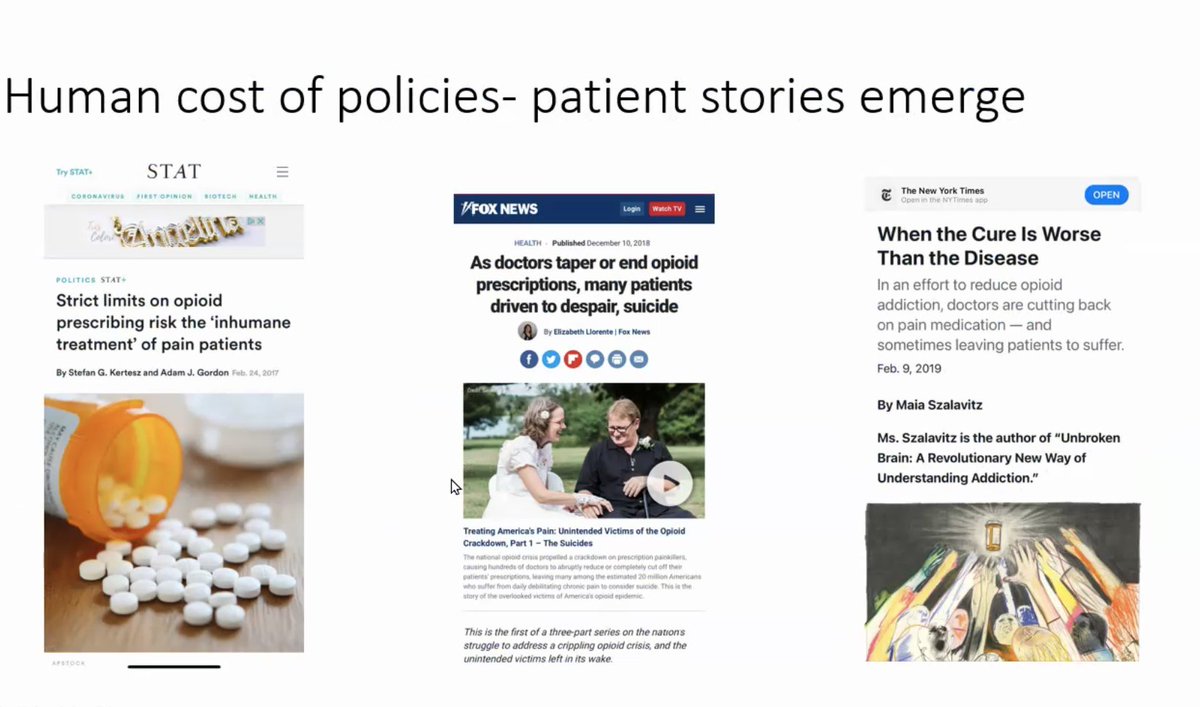
The patient experience deserved attention. This new paper delivers:
"I felt like I had a scarlet letter" @DrugAlcoholDep sciencedirect.com/science/articl…
The patient experience deserved attention. This new paper delivers:
"I felt like I had a scarlet letter" @DrugAlcoholDep sciencedirect.com/science/articl…

2/Interviews with 41 persons tapered (⬇️>50% ) were open. The framework for assessing stigma allowed that it may include “societal-level conditions, cultural norms, & institutional policies that constrain the opportunities, resources, and wellbeing of the stigmatized”
3/Major finding: "Participants identified themselves as overlooked and negatively impacted by measures implemented during the pharmacovigilance period, including various tapering initiatives"
Yep, I've witnessed that.
Yep, I've witnessed that.
4/Major finding: "During the course of pain treatment, dominant cultural norms reinforced the socially devalued status of people living with chronic pain and invalidated their experiences"
Yep, I've witnessed that both institutionally and interpersonally
Yep, I've witnessed that both institutionally and interpersonally
5/Racial mistreatment was bound up with the major finding on invalidation. Black women in particular felt singled out under the tapering regime. Disbelieved and "drug seeking"
Yep: other studies show tapers target persons of color
Yep: other studies show tapers target persons of color

6/Major finding: "During and after opioid tapers, institutional policies and programs further marginalized and yielded unintended consequences for people living with chronic pain"
Yep: we've been decrying the unintended consequences since 2016. Some have heard us.
Yep: we've been decrying the unintended consequences since 2016. Some have heard us.
7/ persons going through this feel their survival is being discounted in care that changes their lives, nonconsensually, discounting them on whole
On social media, they are falsely accused of pharma support. One particularly spiteful advocate says suicides are "a hoax"
On social media, they are falsely accused of pharma support. One particularly spiteful advocate says suicides are "a hoax"
8/As a clinician/scientist who cares for patients with pain and who has been willing to advocate, I have feared a marginal or stigmatized status from speaking up, even in scientifically defensible ways. Many barbs sent my way have featured caricature, or just anger.
9/But I will say (a) we owe it to our own ethics to take seriously the experience of patients who are undergoing a care change our health systems have imposed
(b) pushback toward me confirmed, for me, that speaking out remains absolutely necessary.
(b) pushback toward me confirmed, for me, that speaking out remains absolutely necessary.
10/No person should be left believing they are simply a liability to health systems, to doctors,nurses & pharmacies.
No person should be left like feeling like "the one with the scarlet letter"
We might have to afix scarlet letters to our own chests until we can work this out
No person should be left like feeling like "the one with the scarlet letter"
We might have to afix scarlet letters to our own chests until we can work this out
• • •
Missing some Tweet in this thread? You can try to
force a refresh